Radioactive Colloids
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Guidebook to Particle Size Analysis Table of Contents
A GUIDEBOOK TO PARTICLE SIZE ANALYSIS TABLE OF CONTENTS 1 Why is particle size important? Which size to measure 3 Understanding and interpreting particle size distribution calculations Central values: mean, median, mode Distribution widths Technique dependence Laser diffraction Dynamic light scattering Image analysis 8 Particle size result interpretation: number vs. volume distributions Transforming results 10 Setting particle size specifications Distribution basis Distribution points Including a mean value X vs.Y axis Testing reproducibility Including the error Setting specifications for various analysis techniques Particle Size Analysis Techniques 15 LA-960 laser diffraction technique The importance of optical model Building a state of the art laser diffraction analyzer 18 LA-350 laser diffraction technique Compact optical bench and circulation pump in one system 19 ViewSizer 3000 nanotracking analysis A Breakthrough in nanoparticle tracking analysis 20 SZ-100 dynamic light scattering technique Calculating particle size Zeta Potential Molecular weight 25 PSA300 image analysis techniques Static image analysis Dynamic image analysis 27 Dynamic range of the HORIBA particle characterization systems 27 Selecting a particle size analyzer When to choose laser diffraction When to choose dynamic light scattering When to choose image analysis 31 References Why is particle size important? Particle size influences many properties of particulate materials and is a valuable indicator of quality and performance. This is true for powders, Particle size is critical within suspensions, emulsions, and aerosols. The size and shape of powders influences a vast number of industries. flow and compaction properties. Larger, more spherical particles will typically flow For example, it determines: more easily than smaller or high aspect ratio particles. -
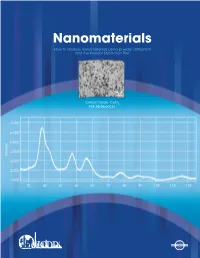
Nanomaterials How to Analyze Nanomaterials Using Powder Diffraction and the Powder Diffraction File™
Nanomaterials How to analyze nanomaterials using powder diffraction and the Powder Diffraction File™ Cerium Oxide CeO2 PDF 00-064-0737 7,000 6,000 5,000 4,000 Intensity 3,000 2,000 1,000 20 30 40 50 60 70 80 90 100 110 120 Nanomaterials Table of Contents Materials with new and incredible properties are being produced around the world by controlled design at the atomic and molecular level. These nanomaterials are typically About the Powder Diffraction File ......... 1 produced in the 1-100 nm size scale, and with this small size they have tremendous About Powder Diffraction ...................... 1 surface area and corresponding relative percent levels of surface atoms. Both the size and available (reactive) surface area can contribute to unique physical properties, Analysis Tools for Nanomaterials .......... 1 such as optical transparency, high dissolution rate, and enormous strength. Crystallite Size and Particle Size ������������ 2 In this Technical Bulletin, we are primarily focused on the use of structural simulations XRPD Pattern for NaCI – An Example .... 2 in order to examine the approximate crystallite size and molecular orientation in nanomaterials. The emphasis will be on X-ray analysis of nanomaterials. However, Total Pattern Analysis and the �������������� 3 Powder Diffraction File electrons and neutrons can have similar wavelengths as X-rays, and all of the X-ray methods described have analogs with neutron and electron diffraction. The use of Pair Distribution Function Analysis ........ 3 simulations allows one to study any nanomaterials that have a known atomic and Amorphous Materials ............................ 4 molecular structure or one can use a characteristic and reproducible experimental diffraction pattern. -

A Comparative Study of Particle Size Distribution of Graphene Nanosheets Synthesized by an Ultrasound-Assisted Method
nanomaterials Article A Comparative Study of Particle Size Distribution of Graphene Nanosheets Synthesized by an Ultrasound-Assisted Method Juan Amaro-Gahete 1,† , Almudena Benítez 2,† , Rocío Otero 2, Dolores Esquivel 1 , César Jiménez-Sanchidrián 1, Julián Morales 2, Álvaro Caballero 2,* and Francisco J. Romero-Salguero 1,* 1 Departamento de Química Orgánica, Instituto Universitario de Investigación en Química Fina y Nanoquímica, Facultad de Ciencias, Universidad de Córdoba, 14071 Córdoba, Spain; [email protected] (J.A.-G.); [email protected] (D.E.); [email protected] (C.J.-S.) 2 Departamento de Química Inorgánica e Ingeniería Química, Instituto Universitario de Investigación en Química Fina y Nanoquímica, Facultad de Ciencias, Universidad de Córdoba, 14071 Córdoba, Spain; [email protected] (A.B.); [email protected] (R.O.); [email protected] (J.M.) * Correspondence: [email protected] (A.C.); [email protected] (F.J.R.-S.); Tel.: +34-957-218620 (A.C.) † These authors contributed equally to this work. Received: 24 December 2018; Accepted: 23 January 2019; Published: 26 January 2019 Abstract: Graphene-based materials are highly interesting in virtue of their excellent chemical, physical and mechanical properties that make them extremely useful as privileged materials in different industrial applications. Sonochemical methods allow the production of low-defect graphene materials, which are preferred for certain uses. Graphene nanosheets (GNS) have been prepared by exfoliation of a commercial micrographite (MG) using an ultrasound probe. Both materials were characterized by common techniques such as X-ray diffraction (XRD), Transmission Electronic Microscopy (TEM), Raman spectroscopy and X-ray photoelectron spectroscopy (XPS). All of them revealed the formation of exfoliated graphene nanosheets with similar surface characteristics to the pristine graphite but with a decreased crystallite size and number of layers. -

Download (14Mb)
A Thesis Submitted for the Degree of PhD at the University of Warwick Permanent WRAP URL: http://wrap.warwick.ac.uk/125819 Copyright and reuse: This thesis is made available online and is protected by original copyright. Please scroll down to view the document itself. Please refer to the repository record for this item for information to help you to cite it. Our policy information is available from the repository home page. For more information, please contact the WRAP Team at: [email protected] warwick.ac.uk/lib-publications Anisotropic Colloids: from Synthesis to Transport Phenomena by Brooke W. Longbottom Thesis Submitted to the University of Warwick for the degree of Doctor of Philosophy Department of Chemistry December 2018 Contents List of Tables v List of Figures vi Acknowledgments ix Declarations x Publications List xi Abstract xii Abbreviations xiii Chapter 1 Introduction 1 1.1 Colloids: a general introduction . 1 1.2 Transport of microscopic objects – Brownian motion and beyond . 2 1.2.1 Motion by external gradient fields . 4 1.2.2 Overcoming Brownian motion: propulsion and the requirement of symmetrybreaking............................ 7 1.3 Design & synthesis of self-phoretic anisotropic colloids . 10 1.4 Methods to analyse colloid dynamics . 13 1.4.1 2D particle tracking . 14 1.4.2 Trajectory analysis . 19 1.5 Thesisoutline................................... 24 Chapter 2 Roughening up Polymer Microspheres and their Brownian Mo- tion 32 2.1 Introduction.................................... 33 2.2 Results&Discussion............................... 38 2.2.1 Fabrication and characterization of ‘rough’ microparticles . 38 i 2.2.2 Quantifying particle surface roughness by image analysis . -

Particle Size Analysis of 99Mtc-Labeled and Unlabeled Antimony Trisulfide and Rhenium Sulfide Colloids Intended for Lymphoscintigraphic Application
Particle Size Analysis of 99mTc-Labeled and Unlabeled Antimony Trisulfide and Rhenium Sulfide Colloids Intended for Lymphoscintigraphic Application Chris Tsopelas RAH Radiopharmacy, Nuclear Medicine Department, Royal Adelaide Hospital, Adelaide, Australia nature allows them to be retained by the lymph nodes (8,9) Colloidal particle size is an important characteristic to consider by a phagocytic mechanism, yet the rate of colloid transport when choosing a radiopharmaceutical for mapping sentinel through the lymphatic channels is directly related to their nodes in lymphoscintigraphy. Methods: Photon correlation particle size (10). Particles smaller than 4–5 nm have been spectroscopy (PCS) and transmission electron microscopy reported to penetrate capillary membranes and therefore (TEM) were used to determine the particle size of antimony may be unavailable to migrate through the lymphatic chan- trisulfide and rhenium sulfide colloids, and membrane filtration (MF) was used to determine the radioactive particle size distri- nel. In contrast, larger particles (ϳ500 nm) clear very bution of the corresponding 99mTc-labeled colloids. Results: slowly from the interstitial space and accumulate poorly in Antimony trisulfide was found to have a diameter of 9.3 Ϯ 3.6 the lymph nodes (11) or are trapped in the first node of a nm by TEM and 18.7 Ϯ 0.2 nm by PCS. Rhenium sulfide colloid lymphatic chain so that the extent of nodal drainage in was found to exist as an essentially trimodal sample with a contiguous areas cannot always be discerned (5). After dv(max1) of 40.3 nm, a dv(max2) of 438.6 nm, and a dv of 650–2200 injection, the radiocolloid travels to the sentinel node 99m nm, where dv is volume diameter. -

Tsi Knows Nanoparticle Measurement
TSI KNOWS NANOPARTICLE MEASUREMENT NANO INSTRUMENTATION UNDERSTANDING, ACCELERATED AEROSOL SCIENCE MEETS NANOTECHNOLOGY TSI CAN HELP YOU NAVIGATE THROUGH NANOTECHNOLOGY Our Instruments are Used by Scientists Throughout a Nanoparticle’s Life Cycle. Research and Development Health Effects–Inhalation Toxicology On-line characterization tools help researchers shorten Researchers worldwide use TSI instrumentation to generate R&D timelines. Precision nanoparticle generation challenge aerosol for subjects, quantify dose, instrumentation can produce higher quality products. and determine inhaled portion of nanoparticles. Manufacturing Process Monitoring Nanoparticle Exposure and Risk Nanoparticles are expensive. Don’t wait for costly Assess the workplace for nanoparticle emissions and off line techniques to determine if your process is locate nanoparticle sources. Select and validate engineering out of control. controls and other corrective actions to reduce worker exposure and risk. Provide adequate worker protection. 2 AEROSOL SCIENCE MEETS NANOTECHNOLOGY What Is a Nanoparticle? Types of Nanoparticles A nanoparticle is typically defined as a particle which has at Nanoparticles are made from a wide variety of materials and are least one dimension less than 100 nanometers (nm) in size. routinely used in medicine, consumer products, electronics, fuels, power systems, and as catalysts. Below are a few examples of Why Nano? nanoparticle types and applied uses: The answer is simple: better material properties. Nanomaterials have novel electrical, -

NIST Recommended Practice Guide : Particle Size Characterization
NATL INST. OF, STAND & TECH r NIST guide PUBLICATIONS AlllOb 222311 ^HHHIHHHBHHHHHHHHBHI ° Particle Size ^ Characterization Ajit Jillavenkatesa Stanley J. Dapkunas Lin-Sien H. Lum Nisr National Institute of Specidl Standards and Technology Publication Technology Administration U.S. Department of Commerce 960 - 1 NIST Recommended Practice Gu Special Publication 960-1 Particle Size Characterization Ajit Jillavenkatesa Stanley J. Dapkunas Lin-Sien H. Lum Materials Science and Engineering Laboratory January 2001 U.S. Department of Commerce Donald L. Evans, Secretary Technology Administration Karen H. Brown, Acting Under Secretary of Commerce for Technology National Institute of Standards and Technology Karen H. Brown, Acting Director Certain commercial entities, equipment, or materials may be identified in this document in order to describe an experimental procedure or concept adequately. Such identification is not intended to imply recommendation or endorsement by the National Institute of Standards and Technology, nor is it intended to imply that the entities, materials, or equipment are necessarily the best available for the purpose. National Institute of Standards and Technology Special Publication 960-1 Natl. Inst. Stand. Technol. Spec. Publ. 960-1 164 pages (January 2001) CODEN: NSPUE2 U.S. GOVERNMENT PRINTING OFFICE WASHINGTON: 2001 For sale by the Superintendent of Documents U.S. Government Printing Office Internet: bookstore.gpo.gov Phone: (202)512-1800 Fax: (202)512-2250 Mail: Stop SSOP, Washington, DC 20402-0001 Preface PREFACE Determination of particle size distribution of powders is a critical step in almost all ceramic processing techniques. The consequences of improper size analyses are reflected in poor product quality, high rejection rates and economic losses. -
Introduction to Dynamic Light Scattering for Particle Size Determination
www.horiba.com/us/particle Jeffrey Bodycomb, Ph.D. Introduction to Dynamic Light Scattering for Particle Size Determination © 2016 HORIBA, Ltd. All rights reserved. 1 Sizing Techniques 0.001 0.01 0.1 1 10 100 1000 Nano-Metric Fine Coarse SizeSize Colloidal Macromolecules Powders AppsApps Suspensions and Slurries Electron Microscope Acoustic Spectroscopy Sieves Light Obscuration Laser Diffraction – LA-960 Electrozone Sensing Methods DLS – SZ-100 Sedimentation Disc-Centrifuge Image Analysis PSA300, Camsizer © 2016 HORIBA, Ltd. All rights reserved. 3 Two Approaches to Image Analysis Dynamic: Static: particles flow past camera particles fixed on slide, stage moves slide 0.5 – 1000 um 1 – 3000 um 2000 um w/1.25 objective © 2016 HORIBA, Ltd. All rights reserved. 4 Laser Diffraction Laser Diffraction •Particle size 0.01 – 3000 µm •Converts scattered light to particle size distribution •Quick, repeatable •Most common technique •Suspensions & powders © 2016 HORIBA, Ltd. All rights reserved. 5 Laser Diffraction Suspension Powders Silica ~ 30 nm Coffee Results 0.3 – 1 mm 14 100 90 12 80 10 70 60 8 50 q(%) 6 40 4 30 20 2 10 0 0 10.00 100.0 1000 3000 Diameter(µm) © 2016 HORIBA, Ltd. All rights reserved. 6 What is Dynamic Light Scattering? • Dynamic light scattering refers to measurement and interpretation of light scattering data on a microsecond time scale. • Dynamic light scattering can be used to determine – Particle/molecular size – Size distribution – Relaxations in complex fluids © 2016 HORIBA, Ltd. All rights reserved. 7 Other Light Scattering Techniques • Static Light Scattering: over a duration of ~1 second. Used for determining particle size (diameters greater than 10 nm), polymer molecular weight, 2nd virial coefficient, Rg. -
Maggie Williams Particle Size, Shape and Sorting: What Grains Can Tell Us
Particle size, shape and sorting: what grains can tell us Maggie Williams Most sediments contain particles that have a range of sizes, so the mean or average grain size is used in description. Mean grain size of loose sediments is measured by size analysis using sieves Grain size >2mm Coarse grain size (Granules<pebble<cobbles<boulders) 0.06 to 2mm Medium grain size Sand: very coarse-coarse-medium-fine-very fine) <0.06mm Fine grain size (Clay<silt) Difficult to see Remember that for sediment sizes > fine sand, the coarser the material the greater the flow velocity needed to erode, transport & deposit the grains Are the grains the same size of different? What does this tell you? If grains are the same size this tells you that the sediment was sorted out during longer transportation (perhaps moved a long distance by a river or for a long time by the sea. If grains are of different sizes the sediment was probably deposited close to its source or deposited quickly (e.g. by a flood or from meltwater). Depositional environments Environment 1 Environment 2 Environment 3 Environment 4 Environment 5 Environment 6 Sediment size frequency plots from different depositional environments • When loose sediment collected from a sedimentary environment is washed and then sieved it is possible to measure the grain sizes in the sediment accurately. • The grain size distribution may then be plotted as a histogram or as a cumulative frequency curve. • Sediments from different depositional environments give different sediment size frequency plots. This shows the grain size distribution for a river sand. -

Determination of Particle Size Distribution in Sediments
Determination of Particle Size Distribution in Sediments DETERMINATION OF PARTICLE SIZE DISTRIBUTION (GRAVEL, SAND, SILT AND CLAY) IN SEDIMENT SAMPLES Scott Laswell+, Susanne J. McDonald*, Alan D. Watts* and James M. Brooks* *TDI-Brooks International/B&B Laboratories Inc. College Station, Texas 77845 +Laser Geo-Environmental Austin, Texas 78748 ABSTRACT Grain size distribution in marine sediments is determined using the Wentworth scale. The major size classes determined are gravel (-2 phi to –5 phi), sand (+4 phi to –1 phi), silt (+5 phi to +7 phi) and clay (+8 phi and smaller). Determining particle size in sediments is important due to potential correlations with contaminant levels. Sediments are pre-treated with hydrogen peroxide to remove organic matter prior to particle size determination. 1.0 INTRODUCTION Higher contaminant concentrations are often associated with finer grain sediments. Consequently, useful correlations can be made between particle size distribution and contaminant concentrations. Particle size distribution is a cumulative frequency distribution, or a frequency distribution of relative amounts of particles in a sample within specified size ranges (phi scale is normally used). The size of a discrete particle is characterized as a linear dimension, and is designated as a particle diameter. The use of sieves and settling tubes, as described below, results in a sediment description based on particle size and density, reported as percentages of the total sample weight. 2.0 APPARATUS AND MATERIALS 2.1 EQUIPMENT · Balance, -

Effect of Particle Size on Microstructure and Strength of Porous Spinel Ceramics Prepared by Pore-Forming in Situ Technique
Bull. Mater. Sci., Vol. 34, No. 5, August 2011, pp. 1109–1112. c Indian Academy of Sciences. Effect of particle size on microstructure and strength of porous spinel ceramics prepared by pore-forming in situ technique WEN YAN∗, NAN LI, YUANYUAN LI, GUANGPING LIU, BINGQIANG HAN and JULIANG XU The Key State Laboratory Breeding Base of Refractories and Ceramics, Wuhan University of Science and Technology, Wuhan 430081, China MS received 5 November 2010; revised 10 March 2011 Abstract. The porous spinel ceramics were prepared from magnesite and bauxite by the pore-forming in situ technique. The characterization of porous spinel ceramics was determined by X-ray diffractometer (XRD), scanning electron microscopy(SEM), mercury porosimetry measurement etc and the effects of particle size on microstructure and strength were investigated. It was found that particle size affects strongly on the microstructure and strength. With decreasing particle size, the pore size distribution occurs from multi-peak mode to bi-peak mode, and lastly to mono-peak mode; the porosity decreases but strength increases. The most apposite mode is the specimens from the grinded powder with a particle size of 6·53 μm, which has a high apparent porosity (40%), a high compressive strength (75·6 MPa), a small average pore size (2·53 μm) and a homogeneous pore size distribution. Keywords. Porous spinel ceramics; particle size; magnesite; bauxite; microstructure; strength. 1. Introduction by injection molding or gel casting (Xie 1998; Liu et al 2001; She and Ohji 2003). Porous alumina ceramics were There is a large energy consumption in the metallurgical prepared by decomposition of Al(OH)3 to form pores in situ industry. -

"Particle Size Distribution/Fibre Length and Diameter
110 Adopted: OECD GUIDELINE FOR TESTING OF CHEMICALS 12 May 1981 "Particle Size Distribution/Fibre Length and Diameter Distributions" Method A: Particle Size Distribution (effective hydrodynamic radius) Method B: Fibre Length and Diameter Distributions 1. I N T R O D U C T O R Y I N F O R M A T I O N •P r e r e q u i s i t e s Method A: – Water insolubility Method B: – Information on fibrous nature of product – Information on stability of fibre shape under electron-microscopic conditions •G u i d a n c e i n f o r m a t i o n Method A: – Melting point Method B: – Melting point •Q u a l i f y i n g s t a t e m e n t s Both test methods can be applied to pure and commercial grade substances. Method A: This method can only be applied to water-insoluble (< 10-6 g/l), powdered type products. The equivalence of the six national and international standard methods for particle size distribution was not tested, and is currently not known. There is a particular problem in relation to sedimentation and Coulter counter measurements. Method B: This method applies only for fibrous products. The effect of impurities on particle shape should be considered. Users of this Test Guideline should consult the Preface, in particular paragraphs 3, 4, 7 and 8. 110 page 2 "Particle Size Distribution/Fibre Length and Diameter Distributions" •R e c o m m e n d a t i o n s Method A: Equivalence of the methods for determination of particle size distribution should be tested in the laboratory.