Reduced Fetal Movements
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Sexual Abuse of Elders Kearsley Home 1. Margaret Eckard
Sexual Abuse of Elders •Kathleen Brown •Associate Professor •University of Pennsylvania •School of Nursing Kearsley Home Retirement home for elderly women Located in West Philadelphia Gothic stone home over 200 years old 60 residents, ages 60-94 Security force on grounds Small in-patient unit; Highly trained staff 1. Margaret Eckard Popular, bubbly 92 year old resident One of longest residents at Kearsley January 23, 1983: missed at breakfast Nurse went to investigate; door ajar Body lying on floor next to rumpled bed Clad in nightgown; curled in fetal position Signs of rigor mortis starting to appear 1 Examination MD concerned over bruises on face; smears of blood around nose and mouth Streaks of blood in vagina and anus Decided not sufficiently disturbing to make an issue; decided natural death due to her age Funeral held 2. Katherine A. Maxwell 85 year old resident February 12, 1983: 21 inch snow storm Katherine failed to show for breakfast Door ajar; body lying on bed Pajamas spotted with blood Storm kept Dr. Webster from the Home Katherine Maxwell Body taken to hospital; no autopsy Blood believed to have occurred by natural causes at her death 2 3. Elizabeth Monroe Celebrated her 86th birthday with a party Next morning, failed to appear at breakfast Nurse found door ajar and her body in bed Face discolored; vaginal bleeding Dr. Webster away; substitute MD Sent body to undertaker Dr. Webster’s Concern Webster called the undertaker; suspicious over the 3 deaths ME’s office were not concerned over the 3 elderly victims’ deaths Webster insistent and ME accepted it for investigation but embalming made it difficult Ruled natural cause death 4. -

Rail Trespasser Fatalities Federal Railroad Administration Demographic and Behavioral Profiles
U.S. Department of Transportation Rail Trespasser Fatalities Federal Railroad Administration Demographic and Behavioral Profiles June 2013 NOTICE This document is disseminated under the sponsorship of the U.S. Department of Transportation in the interest of information exchange. The U.S. Government assumes no liability for its contents or use thereof. Any opinions, findings and conclusions, or recommendations expressed in this material do not necessarily reflect the views or policies of the U.S. Government, nor does mention of trade names, commercial products or organizations imply endorsement by the U.S. Government. The U.S. Government assumes no liability for the content or use of the material contained in this document. NOTICE The U.S. Government does not endorse products or manufacturers. Trade or manufacturers’ names appear herein solely because they are considered essential to the objective of this report. NOTE: This report was prepared by North American Management (NAM) at the direction of the Federal Railroad Administration (FRA) for the purpose of more accurately identifying the types of persons who trespass on railroad rights-of-way, and ultimately reducing the number of trespassing casualties, which contribute significantly to the total annual railroad-related deaths and injuries in the United States. This report is an extension of a March 2008 report produced by Cadle Creek Consulting titled, “Rail Trespasser Fatalities, Developing Demographic Profiles” (2008 Report). The entire 2008 Report can be found at http://www.fra.dot.gov/eLib/Details/L02669. The current report was generated as part of FRA’s continuing efforts to reduce trespassing on railroad rights-of-way and associated fatalities and injuries. -

GMEC) Strategic Clinical Networks Reduced Fetal Movement (RFM
Greater Manchester & Eastern Cheshire (GMEC) Strategic Clinical Networks Reduced Fetal Movement (RFM) in Pregnancy Guidelines March 2019 Version 1.3a GMEC RFM Guideline FINAL V1.3a 130619 Issue Date 15/02/2019 Version V1.3a Status Final Review Date Page 1 of 19 Document Control Ownership Role Department Contact Project Clinical Lead Manchester Academic Health [email protected] Science Centre, Division of Developmental Biology and Medicine Faculty of Biology, Medicine and Health, The University of Manchester. Project Manager GMEC SCN [email protected] Project Officer GMEC SCN [email protected] Endorsement Process Date of Presented for ratification at GMEC SCN Maternity Steering Group on:15th February ratification 2019 Application All Staff Circulation Issue Date: March 2019 Circulated by [email protected] Review Review Date: March 2021 Responsibility of: GMEC Maternity SCN Date placed on March 2019 the Intranet: Acknowledgements On behalf of the Greater Manchester and Eastern Cheshire and Strategic Clinical Networks, I would like to take this opportunity to thank the contributors for their enthusiasm, motivation and dedication in the development of these guidelines. Miss Karen Bancroft Maternity Clinical Lead for the Greater Manchester & Eastern Cheshire SCN GMEC RFM Guideline FINAL V1.3a 130619 Issue Date 15/02/2019 Version V1.3a Status Final Review Date Page 2 of 19 Contents 1 What is this Guideline for and Who should use it? ......................................................................... 4 2 What -

The Stunted Development of in Vitro Fertilization in the United States, 1975-1992
EMBRYONIC POLICIES: THE STUNTED DEVELOPMENT OF IN VITRO FERTILIZATION IN THE UNITED STATES, 1975-1992 Erin N. McKenna A Thesis Submitted to the Graduate College of Bowling Green State University in partial fulfillment of the requirements for the degree of MASTER OF ARTS May 2006 Committee: Dr. Leigh Ann Wheeler, Advisor Dr. Walter Grunden ii Abstract The federal government’s failure to fund research on in vitro fertilization has had an important legacy and significant consequences in the United States. Due to the dismantling of the Ethics Advisory Board in 1980, no government funding was provided for research for in vitro fertilization (IVF), embryo transfer (ET), and gamete intra-fallopian transfer (GIFT). The lack of government funding, regulation, and involvement has resulted in the false advertising of higher success rates to lure patients into the infertility specialists’ offices. In their desperation to have children, consumers of such medical technologies paid exorbitant fees that often remained uncovered by insurance companies. The federal government enacted legislation in 1992 attempting to alleviate some of the aspects of exploitation of the consumer-patient. The government’s recognition of the importance of such procedures was hit and miss, though, much like the reproductive technology itself. The legacy is one that has resulted in American citizens who now turn to developing countries such as Israel and India, where the treatment is drastically cheaper and often more effective. I attempt to explain the federal government’s response to New Reproductive Technologies (NRTs), beginning with in vitro fertilization, thus exploring why and how this debate has inextricably been linked to the ongoing abortion debate. -

Pregnancy Tracker
Women’sPregnancy WelcomeHealth Specialists Packet #5 Pregnancy Tracker It can be confusing to figure out “how far along” you are. A normal pregnancy is dated most times by a patient’s last menstrual period. If a patient is uncertain of when her last menstrual period occurred than an ultrasound may be used to date the pregnancy. A normal pregnancy lasts 42 weeks and your due date is 40 weeks from your last menstrual period. A full term pregnancy is any pregnancy beyond 37 weeks. What to Expect Each Month of Your Pregnancy Office Hours: Our office hours are 9:00-12:00 and 1:00-4:00 Monday through Friday. We are closed on the weekends. If you need to reach a doctor after hours or on the weekend please dial 770-474-0064 and instructions will be given. Calculating Your Due Date The estimated date of delivery (EDD), also known as your due date, is most often calculated from the first day of your last menstrual period. In order to estimate your due date take the date that your last normal menstrual cycle started, add 7 days and count back 3 months. Pregnancy is assumed to have occurred 2 weeks after your last cycle and therefore 2 weeks are added to the beginning of your pregnancy. Pregnancy actually lasts 10 months (40 weeks) and not 9 months. Most women go into labor within 2 weeks of their due date either before or after their actual EDD. For more information, please visit www.girldocs.com First Month (0-4 weeks) Fetal Growth Your Health Sperm fertilizes the egg in one of the fallopian tubes and During this time it is important you take a multivitamin then 5-7 days later the fertilized egg implants (attaches) supplement that contains folic acid 0.4 milligrams daily. -
Turning Your Breech Baby to a Head-Down Position (External Cephalic Version)
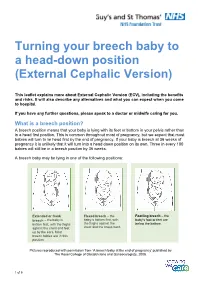
Turning your breech baby to a head-down position (External Cephalic Version) This leaflet explains more about External Cephalic Version (ECV), including the benefits and risks. It will also describe any alternatives and what you can expect when you come to hospital. If you have any further questions, please speak to a doctor or midwife caring for you. What is a breech position? A breech position means that your baby is lying with its feet or bottom in your pelvis rather than in a head first position. This is common throughout most of pregnancy, but we expect that most babies will turn to lie head first by the end of pregnancy. If your baby is breech at 36 weeks of pregnancy it is unlikely that it will turn into a head down position on its own. Three in every 100 babies will still be in a breech position by 36 weeks. A breech baby may be lying in one of the following positions: Extended or frank Flexed breech – the Footling breech – the breech – the baby is baby is bottom first, with baby’s foot or feet are bottom first, with the thighs the thighs against the below the bottom. against the chest and feet chest and the knees bent. up by the ears. Most breech babies are in this position. Pictures reproduced with permission from ‘A breech baby at the end of pregnancy’ published by The Royal College of Obstetricians and Gynaecologists, 2008. 1 of 5 What causes breech? Breech is more common in women who are expecting twins, or in women who have a differently-shaped womb (uterus). -

Prospective Study of Maternal Perception of Decreased Fetal Movement in Third Trimester and Evaluation of Its Correlation with Perinatal Compromise
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Nandi N et al. Int J Reprod Contracept Obstet Gynecol. 2019 Feb;8(2):687-691 www.ijrcog.org pISSN 2320-1770 | eISSN 2320-1789 DOI: http://dx.doi.org/10.18203/2320-1770.ijrcog20190306 Original Research Article Prospective study of maternal perception of decreased fetal movement in third trimester and evaluation of its correlation with perinatal compromise Nupur Nandi, Ritika Agarwal* Department of Obstetrics and Gynecology, Teerthankar Mahaveer Medical College and Research Center, Moradabad, Uttar Pradesh, India Received: 14 November 2018 Accepted: 29 December 2018 *Correspondence: Dr. Ritika Agarwal, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Background: Intrauterine fetal movements are sign of fetal life and well being. Perception of decreased fetal movements by the expecting mother is a common concern for both the mother and her obstetrician. Inadequate evaluation of reported decreased fetal movements may lead to catastrophic perinatal outcome. These necessitates us to identify the mothers perceiving decreased fetal movements, evaluating them to identify any risk factor, and follow up them to know the correlation with perinatal outcome. Methods: Antenatal mothers with singleton pregnancy at third trimester are recruited from OPD/ Emergency of Obstetrics and Gynaecology departments of Teerthankar Mahaveer Medical College and Research Center, Moradabad, Uttar Pradesh, India. Both case and control group comprise of 80 mothers matched by demographic profile, with perception of decreased fetal movements only in case group. -

Chapter 12 Vaginal Breech Delivery
FOURTH EDITION OF THE ALARM INTERNATIONAL PROGRAM CHAPTER 12 VAGINAL BREECH DELIVERY Learning Objectives By the end of this chapter, the participant will: 1. List the selection criteria for an anticipated vaginal breech delivery. 2. Recall the appropriate steps and techniques for vaginal breech delivery. 3. Summarize the indications for and describe the procedure of external cephalic version (ECV). Definition When the buttocks or feet of the fetus enter the maternal pelvis before the head, the presentation is termed a breech presentation. Incidence Breech presentation affects 3% to 4% of all pregnant women reaching term; the earlier the gestation the higher the percentage of breech fetuses. Types of Breech Presentations Figure 1 - Frank breech Figure 2 - Complete breech Figure 3 - Footling breech In the frank breech, the legs may be extended against the trunk and the feet lying against the face. When the feet are alongside the buttocks in front of the abdomen, this is referred to as a complete breech. In the footling breech, one or both feet or knees may be prolapsed into the maternal vagina. Significance Breech presentation is associated with an increased frequency of perinatal mortality and morbidity due to prematurity, congenital anomalies (which occur in 6% of all breech presentations), and birth trauma and/or asphyxia. Vaginal Breech Delivery Chapter 12 – Page 1 FOURTH EDITION OF THE ALARM INTERNATIONAL PROGRAM External Cephalic Version External cephalic version (ECV) is a procedure in which a fetus is turned in utero by manipulation of the maternal abdomen from a non-cephalic to cephalic presentation. Diagnosis of non-vertex presentation Performing Leopold’s manoeuvres during each third trimester prenatal visit should enable the health care provider to make diagnosis in the majority of cases. -

Computerized Fetal Heart Rate Analysis, Doppler Ultrasound and Biophysical Profile Score in the Prediction of Acid–Base Status of Growth-Restricted Fetuses
Ultrasound Obstet Gynecol 2007; 30: 750–756 Published online 10 August 2007 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.4101 Computerized fetal heart rate analysis, Doppler ultrasound and biophysical profile score in the prediction of acid–base status of growth-restricted fetuses S. TURAN*†, O. M. TURAN*†, C. BERG‡, D. MOYANO†, A. BHIDE§, S. BOWER†, B. THILAGANATHAN§, U. GEMBRUCH‡, K. NICOLAIDES†, C. HARMAN* and A. A. BASCHAT* *Department of Obstetrics, Gynecology and Reproductive Sciences, University of Maryland, Baltimore, MD, USA, †Harris Birthright Research Centre for Fetal Medicine, King’s College Hospital and §Fetal Medicine Unit, St George’s Hospital Medical School, London, UK and ‡Department of Obstetrics and Prenatal Medicine, Friedrich-Wilhelm University, Bonn, Germany KEYWORDS: arterial Doppler; biophysical profile scoring; computerized CTG; cord pH; fetal growth restriction; non-stress test; venous Doppler ABSTRACT patients with an equivocal or normal BPS. Abnormal DV Doppler correctly identified false positives among Objective To investigate the performance of non-stress patients with an abnormal BPS. cCTG reduced the rate test (NST), computerized fetal heart rate analysis (cCTG), of an equivocal BPS from 16% to 7.1% when substituted biophysical profile scoring (BPS) and arterial and venous for the traditional NST. Elevated DV Doppler index and Doppler ultrasound investigation in the prediction of umbilical venous pulsations predicted a low pH with 73% acid–base status in fetal growth restriction. sensitivity and 90% specificity (P = 0.008). Methods Growth-restricted fetuses, defined by abdomi- Conclusion In fetal growth restriction with placental nal circumference < 5th percentile and umbilical artery insufficiency, venous Doppler investigation provides the (UA) pulsatility index > 95th percentile, were tested by best prediction of acid–base status. -

Maternal Movement and Position Changes to Facilitate Labor Progress Have Been Discussed in the Literature for Decades
ELAINE ZWELLING, PHD, RN, LCCE, FACCE Abstract The benefi ts of maternal movement and position changes to facilitate labor progress have been discussed in the literature for decades. Recent routine interventions such as amniotomy, induction, fetal monitoring, and epidural anesthesia, as well as an increase in maternal obesity, have made position changes during labor challenging. The lack of maternal changes in position throughout labor can contribute to dystocia and increase the risk of cesarean births for failure to progress or descend. This article provides a historical review of the research fi ndings related to the effects of maternal positioning on the labor process and uses six physiological principles as a framework to offer sug- gestions for maternal positioning both before and after epidural anesthesia. Key Words Birth; Childbirth; Labor, fi rst stage; Labor, second stage; Maternity nursing; Obstetrical nursing; Maternal postures; Maternal positioning. Overcoming the Challenges: Maternal Movement 72 volume 35 | number 2 March/April 2010 or centuries laboring women chose to remain dural anesthesia, found that women who were able to mobile and upright, using positions such as change positions regularly or maintain upright positions standing, sitting, kneeling, hands and knees, or during labor were more comfortable and required less Fsquatting (Gupta & Nikodem, 2000; Johnson, pain medication (Atwood, 1976; de Jong et al., 1997; En- Johnson, & Gupta, 1991). Today immobility throughout gelmann, 1977; Johnson et al., 1991). For instance, Ada- the labor process has become a common occurrence for chi, Shimada, and Usul (2003) found in their study of 58 many childbearing women. Increased medical manage- laboring women that a sitting position decreased labor ment, obesity, lack of patient understanding about the pain in contrast with supine positioning. -

Rivera's Opening Brief
No. 09-1060 ________________________________________________________________________ In the Appellate Court of Illinois Second District PEOPLE OF THE STATE OF ILLINOIS, ) ) Plaintiff-Appellee, ) Appeal from the ) Nineteenth Judicial ) Circuit Court ) v. ) Case. No. 92 CF 2751 ) JUAN A. RIVERA, JR., ) Hon. Christopher C. Starck ) Judge Presiding. Defendant-Appellant. ) ________________________________________________________________________ BRIEF OF DEFENDANT-APPELLANT JUAN A. RIVERA, JR. ________________________________________________________________________ Lawrence Marshall Counsel of Record Stanford Law School 559 Nathan Abbott Way Stanford, California 94306 Thomas P. Sullivan Jane E. Raley Terri L. Mascherin Jeffrey Urdangen Jenner & Block LLP Bluhm Legal Clinic 353 N. Clark Street Northwestern University Chicago, Illinois 60654 School of Law 357 E. Chicago Ave. Chicago, Illinois 60611 Counsel for Defendant-Appellant Juan A. Rivera, Jr. ________________________________________________________________________ ORAL ARGUMENT REQUESTED i _____________________________________________________________________ POINTS AND AUTHORITIES NATURE OF THE CASE ...................................................................................................1 JURISDICTION ..................................................................................................................1 ISSUES PRESENTED FOR REVIEW ...............................................................................1 STATEMENT OF FACTS ..................................................................................................2 -

Role of Vibroacoustic Stimulation Test in Prediction of Fetal Outcome in Terms of Apgar Score
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Singh K et al. Int J Reprod Contracept Obstet Gynecol. 2015 Oct;4(5):1427-1430 www.ijrcog.org pISSN 2320-1770 | eISSN 2320-1789 DOI: http://dx.doi.org/10.18203/2320-1770.ijrcog20150724 Research Article Role of vibroacoustic stimulation test in prediction of fetal outcome in terms of Apgar score Kalpana Singh*, Chankya Das Department of Obstetrics & Gynaecology, Guwahati Medical College & Hospital, Guwahati, Varanasi, Uttar Pradesh, India Received: 05 August 2015 Accepted: 19 August 2015 *Correspondence: Dr. Kalpana Singh, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Background: Role of vibroacoustic stimulation test in prediction of fetal outcome in terms of Apgar score. Aim: To know the efficacy of vibroacoustic stimulation test in prediction of fetal outcome. Methods: The study was conducted in department of obstetrics and gynecology at Guwahati Medical College, in duration of 2007-2009. Total 200 high risk patients underwent VAST. Results: VAST done among all these patients and according to fetal response divided into VAST reactive and non- reactive. In 162 (81%) patients VAST was reactive and 38 (19%) non-reactive. Among VAST (162) reactive patients, 126 (77.77%) went for spontaneous vaginal delivery and for 36 (22.22%) induction planned. Induction failed in 9 patients and cesarean section done. Total babies shifted to NICU 13 (6.5%), 4 babies expired (2%) and 9 (4.5%) improved.