Infants Control of a Robotic Mobility Device Madeline E
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Master List of Games This Is a List of Every Game on a Fully Loaded SKG Retro Box, and Which System(S) They Appear On
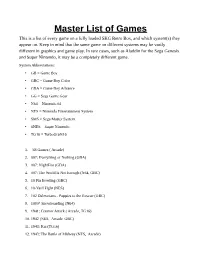
Master List of Games This is a list of every game on a fully loaded SKG Retro Box, and which system(s) they appear on. Keep in mind that the same game on different systems may be vastly different in graphics and game play. In rare cases, such as Aladdin for the Sega Genesis and Super Nintendo, it may be a completely different game. System Abbreviations: • GB = Game Boy • GBC = Game Boy Color • GBA = Game Boy Advance • GG = Sega Game Gear • N64 = Nintendo 64 • NES = Nintendo Entertainment System • SMS = Sega Master System • SNES = Super Nintendo • TG16 = TurboGrafx16 1. '88 Games ( Arcade) 2. 007: Everything or Nothing (GBA) 3. 007: NightFire (GBA) 4. 007: The World Is Not Enough (N64, GBC) 5. 10 Pin Bowling (GBC) 6. 10-Yard Fight (NES) 7. 102 Dalmatians - Puppies to the Rescue (GBC) 8. 1080° Snowboarding (N64) 9. 1941: Counter Attack ( Arcade, TG16) 10. 1942 (NES, Arcade, GBC) 11. 1943: Kai (TG16) 12. 1943: The Battle of Midway (NES, Arcade) 13. 1944: The Loop Master ( Arcade) 14. 1999: Hore, Mitakotoka! Seikimatsu (NES) 15. 19XX: The War Against Destiny ( Arcade) 16. 2 on 2 Open Ice Challenge ( Arcade) 17. 2010: The Graphic Action Game (Colecovision) 18. 2020 Super Baseball ( Arcade, SNES) 19. 21-Emon (TG16) 20. 3 Choume no Tama: Tama and Friends: 3 Choume Obake Panic!! (GB) 21. 3 Count Bout ( Arcade) 22. 3 Ninjas Kick Back (SNES, Genesis, Sega CD) 23. 3-D Tic-Tac-Toe (Atari 2600) 24. 3-D Ultra Pinball: Thrillride (GBC) 25. 3-D WorldRunner (NES) 26. 3D Asteroids (Atari 7800) 27. -

Custom Robo Jumpchain by Blade
Custom Robo Jumpchain By Blade Origins 000 cp - Drop In You are new to this world. You’ve got no friends here, unless you brought one with you. Nothing but the clothes on your back, and some money in your pocket. And a Ray. A Ray Mark 1, if you wanted to be really precise. 000 cp - Hobbyist You are… A fairly normal citizen of this world. You have a Custom Robo, just like everyone else, and have a little bit of talent with it. While it doesn’t consume every waking hour of your day, it is still your primary hobby. 50 cp - Bonus History : Support, requires Hobbyist Where there is a fighter, there will ultimately be a teacher. And maybe a manager, accountant, and coach. You are partnered up with a Tournament Fighter, and your job is to provide training and advice. Maybe you’ve chosen this path because you can’t dive, or maybe just because you really really suck at it. 50 cp - Tournament Fighter Whether it’s school, city, state, or otherwise, you’ve participated in - and probably won - at least one tournament. Basically, compared to a Hobbyist, you are captain serious, and it shows. Your Robo sparkles, you have dozens of spare parts, and maybe even a few bodies to boot. 50 cp - Bonus History : Police Officer, requires Tournament FIghter Your participation in tournaments has gotten you recognition from people other than your peers. The police squad took note of your amazing talent, and made you an offer. An offer that you accepted. Now go forth and enforce the law via mini mecha battles. -

Listado De Roms De Los Packs De NDS De ::. Nota
.:: Listado de Roms de los Packs de NDS de www.zonads.net ::. Nota: Los nombres de los juegos pueden variar ligeramente del nombre real del juego con el que fueron subidos a la web y el orden de los juegos puede variar ligeramente (los teams, que no se aclaran...) Pack Roms 01 [0001-0100] 0001 Electroplankton (JP) 0002 Need for Speed - Underground 2 (US) 0003 Yoshi Touch & Go (US) 0004 Feel the Magic - XY XX (US)(M2) 0005 WarioWare - Touched! (US) 0006 Polarium (US) 0007 Puyo Pop Fever (JP)(M2) 0008 Pac-Pix (US) 0009 Space Invaders DS (JP) 0010 Cool 104 Joker & Setline (JP) 0011 Guru Guru Nagetto (JP) 0012 Asphalt - Urban GT (US) 0013 Yoshi Touch & Go (EU)(M5) 0014 Pac-Pix (EU)(M5) 0015 Catch! Touch! Yoshi! (JP) 0016 Meteos (JP) 0017 Ridge Racer DS (US) 0018 WarioWare - Touched! (EU)(M5) 0019 Mr. Driller - Drill Spirits (US) 0020 Chokkan Hitofude (JP) 0021 Project Rub (EU)(M6) 0022 Super Mario 64 DS (EU)(M5) 0023 Star Wars Episode III - Revenge of the Sith (EU)(M5) 0024 Robots (EU)(M5) 0025 Super Mario 64 DS (JP) 0026 Pokemon Dash (US) 0027 Mr. Driller - Drill Spirits (JP) 0028 Kirby - Canvas Curse (US) 0029 GoldenEye - Rogue Agent (US) 0030 Sprung - The Dating Game (US) 0031 Polarium (EU)(M5) 0032 Bomberman (JP) 0033 Kenshuui Tendo Dokuta (JP) 0034 Zoo Keeper (US) 0035 Touch! Kirby's Magic Paintbrush (JP) 0036 Daigasso! Band Brothers (JP) 0037 Super Mario 64 DS (US) 0038 Ping Pals (US) 0039 Another Code - 2tsu no Kioku (JP) 0040 Hanjuku Eiyuu DS - Egg Monster Hero (JP) 0041 Need for Speed - Underground 2 (EU)(M5) 0042 Nintendogs - Chihuahua & Friends (JP) 0043 Spider-Man 2 (US) 0044 Tennis no Ouji-Sama 2005 - Crystal Drive (JP) 0045 Urbz - Sims in the City, The (US) 0046 Yakuman DS (JP) 0047 Rayman DS (US)(M3) 0048 Mr. -

2014-07 EFF Gaming Exempiton Comment
Before the U.S. COPYRIGHT OFFICE, LIBRARY OF CONGRESS In the Matter of Exemption to Prohibition on Circumvention of Copyright Protection Systems for Access Control Technologies Docket No. 2014-07 Comments of the Electronic Frontier Foundation 1. Commenter Information Electronic Frontier Foundation Kendra Albert Mitch Stoltz (203) 424-0382 Corynne McSherry [email protected] Kit Walsh 815 Eddy St San Francisco, CA 94109 (415) 436-9333 [email protected] The Electronic Frontier Foundation (EFF) is a member-supported, nonprofit public interest organization devoted to maintaining the traditional balance that copyright law strikes between the interests of copyright owners and the interests of the public. Founded in 1990, EFF represents over 25,000 dues-paying members, including consumers, hobbyists, artists, writers, computer programmers, entrepreneurs, students, teachers, and researchers, who are united in their reliance on a balanced copyright system that ensures adequate incentives for creative work while facilitating innovation and broad access to information in the digital age. In filing these comments, EFF represents the interests of gaming communities, archivists, and researchers who seek to preserve the functionality of video games abandoned by their manufacturer. 2. Proposed Class Addressed Proposed Class 23: Abandoned Software—video games requiring server communication Literary works in the form of computer programs, where circumvention is undertaken for the purpose of restoring access to single-player or multiplayer video gaming on consoles, personal computers or personal handheld gaming devices when the developer and its agents have ceased to support such gaming. We ask the Librarian to grant an exemption to the ban on circumventing access controls applied to copyrighted works, 17 U.S.C. -
Nintendo Wi-Fi Connection For
NNiinntetennddoo WWii--FFii CCoonnnneecctitioonn foforr WWiiii Henry Cheng Senior Software Engineer Software Development Support Group NNinintteennddoo WWi-i-FFii CCoonnnneeccttioionn isis aa lologgoo!! NNinintteennddoo WWi-i-FFii CCoonnnneeccttioionn isis ""ininffrraassttrruuccttuurree""!! Authentication Matching Internet Ranking Data Storage Data Download NNinintteennddoo WWi-i-FFii CCoonnnneeccttioionn isis ""ccoommmmuunnitityy""!! NNinintteennddoo WWi-i-FFii CCoonnnneeccttioionn isis livlivee!! Pokémon Diamond Bomberman Land Touch Star Fox Command Status – Up! Status – Up! Status – Up! Pokémon Pearl Final Fantasy III Tenchu: Dark Secret Status – Up! Status – Up! Status – Up! Custom Robo Arena Digimon World DS LostMagic Status – Up! Status – Up! Status – Up! Spectrobes Konductra Bomberman Land Touch Status – Up! Status – Up! Status – Up! Winning Eleven Soccer Contact Tetris DS Status – Up! Status – Up! Status – Up! Diddy Kong Racing DS Clubhouse Games Animal Crossing: Wild World Status – Up! Status – Up! Status – Up! Yu-Gi-Oh GX Spirit Caller Mario vs. DK2 Mario Kart DS Status – Up! Status – Up! Status – Up! Castlevania: Portrait of Ruin Open Season Tony Hawk Status – Up! Status – Up! Status – Up! HHaarrddwwaarree NDEV RVT-H, RVT-R Wi-Fi access point, USB Ethernet, Nintendo Wi-Fi USB connector, Internet connection NNeetwtwoorrkk CCoonnfifigguurraatitioonn SSooftwftwaarree RVLDWC or RVLDWC-DL RevoEx RVL_SDK RRVVLLDDWWCC net connect NAS name check storage ranking http anyone match friend game Download server Net disconnect Friends Management -

Nintendo 64 – All Region Full Collection Checklist
Nintendo 64 – All Region Full Collection Checklist TITLE REGION C B M VALUE 1080° Snowboarding JP, NA, PAL 64 Hanafuda: Tenshi no Yakusoku JP 64 Ozumo JP 64 Ozumo 2 JP Adventure 64" JP Aero Fighters Assault JP, NA, PAL •Sonic Wings Assault JP AeroGauge JP, NA, PAL AI Shogi 3 JP Aidyn Chronicles: The First Mage NA, PAL Air Boarder 64 JP, PAL All Star Tennis '99 NA, PAL •Yannick Noah All Star Tennis '99 FRA All-Star Baseball 2000 NA, PAL All-Star Baseball 2001 NA All-Star Baseball 99 NA, PAL Animal Crossing JP •Dobutsu no Mori JP Armorines: Project S.W.A.R.M. NA, PAL Army Men: Air Combat NA Army Men: Sarge's Heroes NA, PAL Army Men: Sarge's Heroes 2 NA Asteroids Hyper 64 NA Automobili Lamborghini JP, NA, PAL •Super Speed Race 64 JP Bakuretsu Muteki Bangai-O JP Bakusho Jinsei 64: Mezase! Resort O JP Banjo-Kazooie JP, NA, PAL •Banjo to Kazooie no Daiboken JP Key: C = Cartridge | B = Box | M = Manual Click Title To Check Current Selling Value Nintendo 64 – All Region Full Collection Checklist Banjo-Tooie JP, NA, PAL •Banjo to Kazooie no Daiboken 2 JP Bass Hunter 64 NA, PAL Bass Masters 2000 NA Bass Rush: ECOGEAR PowerWorm Championship JP Batman Beyond: Return of the Joker NA, PAL •Batman of the Future: Return of the Joker PAL BattleTanx NA BattleTanx: Global Assault NA, PAL Battlezone: Rise of the Black Dogs NA Beetle Adventure Racing! •As Aventuras do Fusca BRZ JP, NA, PAL •HSV Adventure Racing AUS Big Mountain 2000 JP, NA •Snow Speeder JP Bio F.R.E.A.K.S. -
Liste Des Jeux - GPD XD Plus Version 256Go
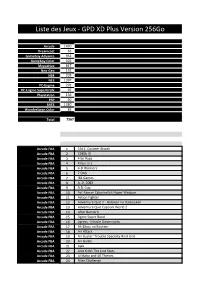
Liste des Jeux - GPD XD Plus Version 256Go Arcade 1430 Dreamcast 66 Gameboy Advance 951 Gameboy Color 502 Megadrive 817 Neo-Geo 152 N64 205 NES 1397 PC-Engine 291 PC-Engine SuperGrafx 97 Playstation 136 PSP 60 SNES 1380 WonderSwan Color 83 Total 7567 Arcade FBA 1 1941: Counter Attack Arcade FBA 2 1945k III Arcade FBA 3 4 En Raya Arcade FBA 4 4 Fun in 1 Arcade FBA 5 4-D Warriors Arcade FBA 6 7 Ordi Arcade FBA 7 '88 Games Arcade FBA 8 A. D. 2083 Arcade FBA 9 A.B. Cop Arcade FBA 10 Act-Fancer Cybernetick Hyper Weapon Arcade FBA 11 Action Fighter Arcade FBA 12 Adventure Quiz 2 - Hatena? no Daibouken Arcade FBA 13 Adventure Quiz Capcom World 2 Arcade FBA 14 After Burner II Arcade FBA 15 Agent Super Bond Arcade FBA 16 Agress - Missile Daisenryaku Arcade FBA 17 Ah Eikou no Koshien Arcade FBA 18 Air Attack Arcade FBA 19 Air Buster: Trouble Specialty Raid Unit Arcade FBA 20 Air Gallet Arcade FBA 21 Ajax Arcade FBA 22 Alex Kidd: The Lost Stars Arcade FBA 23 Ali Baba and 40 Thieves Arcade FBA 24 Alien Challenge Arcade FBA 25 Alien Storm Arcade FBA 26 Alien Syndrome Arcade FBA 27 Aliens Arcade FBA 28 Ambush Arcade FBA 29 Amidar Arcade FBA 30 Angel Kids Arcade FBA 31 Anteater Arcade FBA 32 Aqua Jack Arcade FBA 33 Arabian Arcade FBA 34 Arbalester Arcade FBA 35 Arcadia Arcade FBA 36 Ark Area Arcade FBA 37 Arkanoid - Revenge of DOH Arcade FBA 38 Arkanoid Plus! Arcade FBA 39 Armed Police Batrider Arcade FBA 40 Atomic Robo-kid Arcade FBA 41 Aztarac Arcade FBA 42 Battle Chopper Arcade FBA 43 Battle Garegga Arcade FBA 44 Big Twin Arcade FBA 45 Black Hole Arcade FBA 46 Black Panther Arcade FBA 47 Blandia Arcade FBA 48 Block Gal Arcade FBA 49 Block Hole Arcade FBA 50 Block Out Arcade FBA 51 Blood Bros. -

CONSOLIDATED FINANCIAL STATEMENTS Nintendo Co., Ltd
earnings releases July 28, 2004 Nintendo Co., Ltd. 11-1 Kamitoba hokotate-cho, Minami-ku, Kyoto 601-8501 Japan CONSOLIDATED FINANCIAL STATEMENTS Nintendo Co., Ltd. and Consolidated Subsidiaries FINANCIAL HIGHLIGHTS Three months ended June 30, 2003 and 2004, and year ended March 31, 2004 The amounts presented herein are rounded down under one million yen except as otherwise denominated. Numbers in parentheses are negative. Yen in Millions Three months ended Three months ended Year ended Jun. 30, 2004 Jun. 30, 2003 Mar. 31, 2004 Net sales 82,153 83,821 514,805 Percentage change from the same period of the previous year (2.0%) Operating income 17,467 7,245 107,683 Percentage change from the same period of the previous year 141.1% Income before income taxes and extraordinary items 36,505 17,713 50,140 Percentage change from the same period of the previous year 106.1% Net income 22,635 11,450 33,194 Percentage change from the same period of the previous year 97.7% Net income per share ¥169.32 ¥85.52 ¥246.93 During the first quarter ended June 30, 2004, in the electronic entertainment products division, sales of GAME BOY ADVANCE SP handheld system continued to expand. In the software category, titles such as the simple yet profound "Mario vs. Donkey Kong", the latest release from the popular "Kirby" series "Kirby & The Amazing Mirror", and the second edition of "FAMICOM MINI" series (which enables users to enjoy FAMICOM software on the GAME BOY ADVANCE system) enjoyed favorable sales. As for home console related products, "Pikmin 2" was released in Japan. -
![WHY DO PEOPLE IMAGINE ROBOTS] This Project Analyzes Why People Are Intrigued by the Thought of Robots, and Why They Choose to Create Them in Both Reality and Fiction](https://docslib.b-cdn.net/cover/7812/why-do-people-imagine-robots-this-project-analyzes-why-people-are-intrigued-by-the-thought-of-robots-and-why-they-choose-to-create-them-in-both-reality-and-fiction-6717812.webp)
WHY DO PEOPLE IMAGINE ROBOTS] This Project Analyzes Why People Are Intrigued by the Thought of Robots, and Why They Choose to Create Them in Both Reality and Fiction
Project Number: LES RBE3 2009 Worcester Polytechnic Institute Project Advisor: Lance E. Schachterle Project Co-Advisor: Michael J. Ciaraldi Ryan Cassidy Brannon Cote-Dumphy Jae Seok Lee Wade Mitchell-Evans An Interactive Qualifying Project Report submitted to the Faculty of WORCESTER POLYTECHNIC INSTITUTE in partial fulfillment of the requirements for the Degree of Bachelor of Science [WHY DO PEOPLE IMAGINE ROBOTS] This project analyzes why people are intrigued by the thought of robots, and why they choose to create them in both reality and fiction. Numerous movies, literature, news articles, online journals, surveys, and interviews have been used in determining the answer. Table of Contents Table of Figures ...................................................................................................................................... IV Introduction ............................................................................................................................................. I Literature Review .................................................................................................................................... 1 Definition of a Robot ........................................................................................................................... 1 Sources of Robots in Literature ............................................................................................................ 1 Online Lists ..................................................................................................................................... -

Nintendo Games
The Video Game Guy, Booths Corner Farmers Market - Garnet Valley, PA 19060 (302) 897-8115 www.thevideogameguy.com System Game Genre NES 720 Sports NES 1942 Other NES 10-Yard Fight Football NES 190 in 1 Cartridge Other NES 1943 the Battle of Midway Other NES 3-D WorldRunner Action & Adventure NES 76 in 1 Cartridge Other NES 8 Eyes Action & Adventure NES A Boy and His Blob Trouble on Blobolonia Action & Adventure NES Abadox Action & Adventure NES Action 52 Action & Adventure NES Addams Family Action & Adventure NES Addams Family Pugsley's Scavenger Hunt Action & Adventure NES Advanced Dungeons and Dragons Dragon Strike Strategy NES Advanced Dungeons and Dragons Heroes of the Lance Strategy NES Advanced Dungeons and Dragons Hillsfar Strategy NES Advanced Dungeons and Dragons Pool of Radiance Strategy NES Adventure Island Action & Adventure NES Adventure Island 3 Action & Adventure NES Adventure Island ii Action & Adventure NES Adventures in the Magic Kingdom Action & Adventure NES Adventures of Bayou Billy Action & Adventure NES Adventures of Dino Rikki Action & Adventure NES Adventures of Lolo Action & Adventure NES Adventures of Lolo 2 Action & Adventure NES Adventures of Lolo 3 Puzzle NES Adventures of Rocky and Bullwinkle and Friends Action & Adventure NES Adventures of Tom Sawyer Action & Adventure NES After Burner Other NES Air Fortress Other NES Airwolf Action & Adventure NES Al Unser Turbo Racing Racing NES Aladdin Action & Adventure NES Alfred Chicken Action & Adventure NES Alien 3 Action & Adventure NES Alien Syndrome Action & -

Consolidated Financial Highlights
CONSOLIDATED FINANCIAL HIGHLIGHTS January 25, 2007 Nintendo Co., Ltd. 11-1 Kamitoba hokotate-cho, Minami-ku, Kyoto 601-8501 Japan 1. Consolidated Results for the Nine Months Ended December 2005 and 2006, and Year Ended March 2006 (1) Consolidated operating results (Amounts below one million are rounded down) Income before income taxes Net sales Operating income Net income and extraordinary items million yen % million yen % million yen % million yen % Nine months ended Dec. 31, '06 712,589 72.8 167,633 102.5 220,713 50.5 131,916 43.1 Nine months ended Dec. 31, '05 412,339 (1.7) 82,783 (19.7) 146,694 27.2 92,185 36.1 Year ended Mar. 31, '06 509,249 90,349 160,759 98,378 Net income per share yen Nine months ended Dec. 31, '06 1,031.32 Nine months ended Dec. 31, '05 713.96 Year ended Mar. 31, '06 762.28 [Note] Percentage for net sales, operating income etc. show increase (decrease) from previous third quarter period. With respect to the handheld game products of the electronic entertainment division, both "Nintendo DS" hardware and software recorded very strong sales for the nine month period ended December 31, 2006. "Nintendo DS" hardware has been the fastest rising game platform ever in the Japan market, and, in addition, has sold well in overseas markets. As a result, sales in the first three quarters have reached 18.88 million units on a worldwide basis. As for ” Nintendo DS ” software, net sales have also accelerated, supported by a number of millon-seller titles. -

1080° Avalanche 18 Wheeler: American Pro Trucker 2002 FIFA
1080° Avalanche 18 Wheeler: American Pro Trucker 2002 FIFA World Cup 4x4 EVO 2 The Adventures of Jimmy Neutron Boy Genius: Attack of the Twonkies The Adventures of Jimmy Neutron Boy Genius: Jet Fusion Aggressive Inline Alien Hominid All-Star Baseball 2002 All-Star Baseball 2003 All-Star Baseball 2004 Amazing Island American Chopper 2: Full Throttle Animal Crossing Animaniacs: The Great Edgar Hunt The Ant Bully Aquaman: Battle for Atlantis Army Men: Air Combat - The Elite Missions Army Men RTS: Real Time Strategy Army Men: Sarge's War ATV Quad Power Racing 2 Auto Modellista Avatar: The Last Airbender Backyard Baseball Backyard Football Backyard Sports Baseball 2007 Bad Boys: Miami Takedown Baldur's Gate: Dark Alliance Barbarian Barnyard Baten Kaitos: Eternal Wings and the Lost Ocean Baten Kaitos Origins Batman Begins Batman: Dark Tomorrow Batman: Rise of Sin Tzu Batman Vengeance Battalion Wars Beach Spikers Beyblade VForce: Super Tournament Battle Beyond Good & Evil Big Air Freestyle Big Mutha Truckers Billy Hatcher and the Giant Egg Bionicle Bionicle Heroes Black & Bruised Blood Omen 2 BloodRayne Bloody Roar: Primal Fury BlowOut BMX XXX Bomberman Generation Bomberman Jetters Bratz: Forever Diamondz Bratz: Rock Angelz Buffy the Vampire Slayer: Chaos Bleeds Burnout Burnout 2: Point of Impact Bust-a-Move 3000 Cabela's Big Game Hunter 2005 Adventures Cabela's Dangerous Hunts 2 Cabela's Outdoor Adventures Call of Duty: Finest Hour Call of Duty 2: Big Red One Capcom vs. SNK 2 EO Carmen Sandiego: The Secret of the Stolen Drums Cars Casper: Spirit Dimensions Catwoman Cel Damage Chaos Field Charlie and the Chocolate Factory Charlie's Angels Chibi-Robo! The Chronicles of Narnia: The Lion, the Witch and the Wardrobe City Racer Codename: Kids Next Door - Operation: V.I.D.E.O.G.A.M.E.