AIRCRAFT ACCIDENT INVESTIGATION Report 831-1053
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Airport City Developments in Australia : Land Use Classification and Analyses
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Queensland University of Technology ePrints Archive QUT Digital Repository: http://eprints.qut.edu.au/ Walker, Arron R. and Stevens, Nicholas J. (2008) Airport city developments in Australia : land use classification and analyses. In: 10th TRAIL Congress and Knowledge Market, 14-15 October 2008, Rotterdam, The Netherlands. © Copyright 2008 [please consult the authors] Airport city developments in Australia Land use classification and analyses TRAIL Research School, Delft, October 2008 Authors Dr. Arron Walker, Dr. Nicholas Stevens Faculty of Built Environment and Engineering, School of Urban Development, Queensland University of Technology, Qld, Australia © 2008 by A. Walker, N. Stevens and TRAIL Research School Contents Abstract 1 Introduction.......................................................................................................1 2 Background........................................................................................................2 2.1 Aviation growth in Australia...............................................................................2 2.2 Airport ownership in Australia ...........................................................................3 2.3 Airport Planning under Airports Act 1996 .........................................................4 2.4 Diversification of airport revenue.......................................................................5 3 Land use analysis: methods and materials .....................................................5 -

Download Newsletter
ISSUE 26 | SEPTEMBER 2020 Archerfield Brisbane’s Metropolitan Airport Scholarship winner announced Griffith University aviation student, Chace Eldridge (pictured), has been awarded the inaugural H.C. Brinsmead Scholarship, funded by Archerfield Airport Corporation (AAC). The scholarship honours the pioneering work of Horace Brinsmead, who led what became Australia’s Civil Aviation Safety Authority (CASA) after World War 1. It is open to Griffith University Bachelor of Aviation and Bachelor of Aviation Management students. Chace, 20, is in his final year of Bachelor of Aviation studies and is focused on a career as a commercial pilot in Australia. He was recently accepted into the QANTAS Group Pilot Academy flight training program, which he hopes will provide a direct pathway to achieving his personal goal. The $4000 scholarship was awarded to a Griffith University student who reflects Brinsmead’s values of commitment and teamwork in the establishment of CASA. As well as studying and running his own fitness business, Chace is a Coordinator for the University’s Aviation Mentoring Program which matches students and aviation industry mentors. He is also a leader in the University’s MATES Program for aviation students, and last year mentored high school students at the University’s Flight Camp. Additionally, he is the Legal Officer on the National Committee of the Australian Youth Aerospace Association. “I want to thank AAC for this opportunity to further pursue my career ambitions,” Chace said. “Brinsmead was hugely impactful in shaping Australia to be one of the safest places to fly in the world. He was inspirational because he maintained his passionate beliefs about high standards in civilian aviation despite coming up against sections of the industry bitterly opposed to change.” Away from work and studies, Chace competes in football and cross country. -

Aircraft Accident Investigation Report 821-1004
Jj. AUSTRALIA,.^ •<<-<- Aircraft Accident Investigation Report 821-1004 Cessna 411AVH-AYE Archerfield, Queensland 5 January 1982 BUREAU OF AIR SAFETY INVESTIGATION Aircraft Accident Investigation Report 821-1004 Reprographics Pty Ltd Cessna 411A VH-AYE Archerfield Airport Queensland 5 January 1982 The Secretary to the Department of Aviation authorised the investigation of this accident and the publication of this report pursuant to the powers conferred by Air Navigation Regulations 278 and 283 respectively. Prepared by the Bureau of Air Safety Investigation March 1983 Australian Government Publishing Service Canberra 1983 © Commonwealth of Australia 1983 ISBN 0 644 00485 1 Printed by Commonwealth Print Unit, Melbourne Contents Synopsis 1 1. Factual information 1 . 1 History of the flight 1 .2 Injuries to persons 3 .3 Damage to aircraft 3 .4 Other damage 4 .5 Personnel information 4 .5.1 Flight crew 4 .5.2 Air Traffic Controllers 5 1.6 Aircraft information 5 .6.1 History and documentation 5 .6.2 Engines and propellers 6 .6.3 Maintenance 7 .6.4 Weight and balance 8 1.7 Meteorological information 8 1.8 Aids to navigation 9 1.9 Communications 9 1.10 Aerodrome information 9 1.11 Flight recorders 9 1.12 Wreckage and impact information 12 1.13 Medical and pathological information 12 1.14 Fire 12 1.15 Survival aspects 13 1.16 Tests and research 13 1.16.1 Engines 13 1.16.2 Engine controls 13 1.16.3 Propellers 14 1.16.4 Propeller governors 14 1.16.5 Turbochargers 15 .16.6 Turbocharger controllers 15 .16.7 Exhaust pipes 16 .16.8 Fuel and oil samples 16 .16.9 Landing gear operation 16 .16.10 Engine response to throttle movement 16 . -

The Economics of Road Transport of Beef Cattle
THE ECONOMICS OF ROAD TRANSPORT OF BEEF CATTLE NORTHERN TERRITORY AND QUEENSLAND CHANNEL COUNTRY BUREAU OF AGRICULTURAL ECONOMICS \CANBERRA! AUSTRALIA C71 A.R.A.PURA SEA S5 CORAL SEA NORTHERN TER,RITOR 441I AND 'go \ COUNTRY DARWIN CHANNEL Area. ! Arnhem Land k OF 124,000 S9.mla Aborig R e ), QUEENSLAND DARWIN 1......../L5 GULF OF (\11 SHOWING CARPENTARIA NUMBERS —Zr 1, AREAS AND CATTLE I A N ---- ) TAKEN AT 30-6-59 IN N:C.AND d.1 31-3-59 IN aLD GULF' &Lam rol VI LO Numbers 193,000 \ )14 LEGEND Ar DISTRIT 91, 200 Sy. mls. ••• The/ Elarkl .'-lc • 'Tx/at:viand ER Area , 94 000'S‘frn Counb-v •• •1 411111' == = == Channal Cattle Numbers •BARKLY• = Fatizning Araas 344,0W •• 4* • # DISTRICT • Tannin! r Desert TABLELANDS, 9.4• • 41" amoowea,1 •• • • Area, :NV44. 211,800Sq./nil -N 4 ••• •Cloncurry ALICE NXil% SOCITIf PACIFIC DISTRI W )• 9uches `N\ OCEAN Cattle \ •Dajarra, -r Number 28,000 •Winbon 4%,,\\ SPRINGS A rn/'27:7 0 liazdonnell Ji Ranges *Alice Springs Longreach Simpson DISTRICT LCaWe Desert Numbers v 27.1000 ITh Musgra Ranges. T ullpq -_,OUNTRY JEJe NuTber4L. S A 42Anc SAE al- (gCDET:DWaD [2 ©MU OniVITELE2 NORTHERN TERRITORY AND QUEENSLAND CHANNEL COUNTRY 1959 BUREAU OF AGRICULTURAL ECONOMICS CANBERRA AUSTRALIA 4. REGISTERED AT THE G.P.O. SYDNEY FOR TRANSMISSION BY POST AS A BOOK PREFACE. The Bureau of Agricultural Economics has undertaken an investigation of the economics of road transport of beef cattle in the remote parts of Australia inadequately served by railways. The survey commenced in 1958 when investigations were carried out in the pastoral areas of Western Australia and a report entitled "The Economics of Road Transport of Beef Cattle - Western Australian Pastoral Areas" was subsequently issued. -
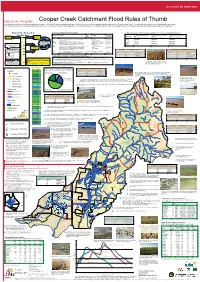
Cooper Creek Catchment Flood Rules of Thumb This Guide Has Used the Best Information Available at Present
QueenslandQueenslandthethe Smart Smart State State How to use this guide: Cooper Creek Catchment Flood Rules of Thumb This guide has used the best information available at present. It is intended to help you assess what type of flood is likely to occur in your area and indicate what amount of feed you might expect. You may wish to record your own flooding guides on the map. You can add more value to this guide by participating in an MLA EDGEnetwork Grazing Land Management (GLM) training package. GLM training helps you identify land types and flood zones and to develop a grazing management plan for your property Amount of rain needed Channel Country Flood descriptions Estimated Summer Flood Pasture Growth in the Channel Country Floodplains. Frequently flooded plains Occasionally flooded plains Swamps and depressions for flooding Flood type Description Land Hydrology Pasture growth Isolated Systems which supports: Flood type (C1) (C2) (C3) Widespread Widespread Rain 100 mm Localised Rain “HANDY” to flooded “GOOD” flood Then increases (kg DM/ha of useful feed) (kg DM/ha of useful feed) (kg DM/ha of useful feed) 95 “GOOD” flood Good Good floods are similar to handy floods, but cover a much higher C1, C3, C2 Flooded across most of 85 - 100% of to proportion of the floodplain (75% or more) and grow more feed per floodplains potential cattle Good 1200-2500 1500-3500 4500-8000 90 area than a handy flood. 80-100% inundation numbers 85 IF in 24-72 hrs Handy Handy floods occur when the water escapes from the gutters, C1, C3 Pushing out of gutters across 45 - 85% of Handy 750-1500 100-250 3500-6500 80 PRIOR, rains of (or useful) connecting up to form the large sheets of water. -

Strategic Framework MAP: QSC
ad D t Ro rut me e to Em v n all i S lack R t B re on e E s t d a m oa g ot a R le he ak rTe ar D t Y S et r m i n v o m r E e ls e e r G N v Developmental Ro e i ina ad reet y v ant a St i R Q iam Brolg r D i u c R n il a p C o d n i s e S a h o A i t m d o p s r t av e a R u o l m e e Road e h e r h S o t t T a h S t a S r d T d e A n o i m e t m m Inset 3 - Adavale o g e Jundah r rf oad a ield R ! d Strategic Framework h s a Roa in r t Ro T d k ve rea r Ri et e a i R L rcoo a p a k l B i ra u Ya Legend Q er ! iv Urban centres R Inset 1 - Quilpie n ! o ad Local centres s Ro m s o n ! h ow T D Localities nd ment Road mo velop am Diamantina De H Waterbody/waterway Mitche ll Street Windorah Railway t ! d e oa e R r t le Petroleum pipeline licences S Q a v u a n i lp d o ie A Arterial roads c W l a l i a e n do c k D ra Bla Connecting roads Berella St h reet Ro ad Road casement Cooper Developemntal Road Quilpie Shire boundary Quilpie Planning Scheme Zones Inset 2 - Eromanga iver Thomson R Scheme Thylungra Bulgroo Road Bulgro Recreation and Open Space o Ad ava d le a Ro Rural o ad Adavale R ! d a Rural Residential id n Refer ri T Ada Inset 3 vale Road Township While every care is taken to ensure the accuracy of this Lake Dartmouth product Quilpie Shire Council makes no representations or warranties about the accuracy, reliability, completeness or d suitability for any particular purpose and disclaims all a o R responsibility and all liability(including without limitation, d le a a liability in negligence) for all expenses, losses, damages o r v R a e (including indirect or consequential damages) and costs a d br v a i Ky D A you may incur as a result of the product being inaccurate ia R e m i o a p l or incomplete in any way or for any reason. -

Central West Health Profile
Medical Officer Opportunities Contents Location Information 1 Acknowledgement of Traditional Owners and Elders 2 Our Profile 3 Structure 4 Facility Information 6 Remuneration Packages 10 Testimonials 13 Living in Central West Queensland 15 Local Attractions 19 Festival Season 21 Published with the assistance of https://www.health.qld.gov.au/rrcsu ii Central West Hospital and Health Service - October 2018 | Medical Officer Opportunities Location Information Contact us: Medical Recruitment Central West Hospital and Health Service PO Box 510, Longreach Qld 4730 T: 4652 8030 F: 4652 8099 E: [email protected] 1 Central West Hospital and Health Service - October 2018 | Medical Officer Opportunities Acknowledgement of Traditional Owners and Elders Artworks attributed to Lionel Dempsey, Amy Blucher, Joyce Crombie, Jean Barr-Crombie, Jennifer Punch, Kiona Weldon, Madonna Dwyer, Pearl Eatts, Lyndal Monaghan and Zane Douglas We would like to pay our respect to the First Peoples, traditional custodians of the land and waterways and thank the custodians who act on behalf of their Peoples for their continued hospitality across the expanse of the health service. We acknowledge and celebrate the continuation of a living culture that has a unique role in the Central West Hospital and Health Service area. We also acknowledge our elders past and present as well as our emerging leaders of tomorrow and thank them for their wisdom and guidance as we seek to improve healthcare outcomes for all our population. The population of the central west region of Queensland reflects a 7.3 percentage who identify as being of Aboriginal and / or Torres Strait Islander descent. -

Brisbane's Metropolitan Airport Archerfield
ISSUE 17 | MARCH 2018 Archerfield Brisbane’s Metropolitan Airport Some Outback Air Race organisers are also competitors, like the ‘3 Amigos’ team - Peter Williams (Treasurer), Malcolm MacDonald (‘Chief Photographer’) and Tony Mitchell (‘Chief Entertainment Officer’). Archerfield Airport hosts Outback Air Race start to support RFDS Archerfield Airport will host a record field of 43 aircraft leader and the great grand-nephew of Sir Charles Kingsford- for the start of the 2018 Outback Air Race in August. Smith (see page 3). This unique and fun 12 day event is a GPS-based navigation time After leaving Archerfield Airport, competitors will fly to Bundaberg, trial over 4,000km of remote Australia. It’s held every three years Longreach, Mount Isa, Adels Grove, Daly Waters, Katherine/ to raise funds for the Royal Flying Doctor Service (RFDS) – and Tindal and Kununurra before finishing the event in Broome, Western this year’s race has special significance as the RFDS celebrates Australia on August 31. the 90th anniversary of its first flight from Cloncurry in 1928. The race has been held since 1996 and tests pilots’ basic The staggered start on Sunday August 19 will be preceded by navigational and planning skills. As well as offering a once-in-a- social activities for the event’s 100 competitors and their families. lifetime experience, it has so far raised more than $2 million for Members of the public will be encouraged to view departing the RFDS. aircraft from vantage points outside the airport boundary. The Although team nominations have closed, sponsorship is still aircraft lineup includes Cessna, Piper, Trinidad, Glasair, Bristell available. -
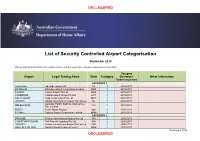
Airport Categorisation List
UNCLASSIFIED List of Security Controlled Airport Categorisation September 2018 *Please note that this table will continue to be updated upon new category approvals and gazettal Category Airport Legal Trading Name State Category Operations Other Information Commencement CATEGORY 1 ADELAIDE Adelaide Airport Ltd SA 1 22/12/2011 BRISBANE Brisbane Airport Corporation Limited QLD 1 22/12/2011 CAIRNS Cairns Airport Pty Ltd QLD 1 22/12/2011 CANBERRA Capital Airport Group Pty Ltd ACT 1 22/12/2011 GOLD COAST Gold Coast Airport Pty Ltd QLD 1 22/12/2011 DARWIN Darwin International Airport Pty Limited NT 1 22/12/2011 Australia Pacific Airports (Melbourne) MELBOURNE VIC 1 22/12/2011 Pty. Limited PERTH Perth Airport Pty Ltd WA 1 22/12/2011 SYDNEY Sydney Airport Corporation Limited NSW 1 22/12/2011 CATEGORY 2 BROOME Broome International Airport Pty Ltd WA 2 22/12/2011 CHRISTMAS ISLAND Toll Remote Logistics Pty Ltd WA 2 22/12/2011 HOBART Hobart International Airport Pty Limited TAS 2 29/02/2012 NORFOLK ISLAND Norfolk Island Regional Council NSW 2 22/12/2011 September 2018 UNCLASSIFIED UNCLASSIFIED PORT HEDLAND PHIA Operating Company Pty Ltd WA 2 22/12/2011 SUNSHINE COAST Sunshine Coast Airport Pty Ltd QLD 2 29/06/2012 TOWNSVILLE AIRPORT Townsville Airport Pty Ltd QLD 2 19/12/2014 CATEGORY 3 ALBURY Albury City Council NSW 3 22/12/2011 ALICE SPRINGS Alice Springs Airport Pty Limited NT 3 11/01/2012 AVALON Avalon Airport Australia Pty Ltd VIC 3 22/12/2011 Voyages Indigenous Tourism Australia NT 3 22/12/2011 AYERS ROCK Pty Ltd BALLINA Ballina Shire Council NSW 3 22/12/2011 BRISBANE WEST Brisbane West Wellcamp Airport Pty QLD 3 17/11/2014 WELLCAMP Ltd BUNDABERG Bundaberg Regional Council QLD 3 18/01/2012 CLONCURRY Cloncurry Shire Council QLD 3 29/02/2012 COCOS ISLAND Toll Remote Logistics Pty Ltd WA 3 22/12/2011 COFFS HARBOUR Coffs Harbour City Council NSW 3 22/12/2011 DEVONPORT Tasmanian Ports Corporation Pty. -

Heritage Citation
Heritage Citation Archerfield Airport - Hangar & Interwar Buildings Key details Addresses At 381 Beatty Road, Archerfield, Queensland 4108 Type of place Airport Period Interwar 1919-1939, World War II 1939-1945 Style Functionalist Lot plan L2_SP200283 Key dates Local Heritage Place Since — 1 July 2002 Date of Citation — April 2008 Criterion for listing (A) Historical; (C) Scientific; (D) Representative; (F) Technical; (H) Historical association Archerfield Aerodrome was Brisbane’s commercial airport from 1931 until 1949. It is linked to a number of historic flights by aviation pioneers such as Charles Kingsford Smith and Lores Bonney. During World War II, it became a major airbase for the US Army’s 5th Air Force and Archerfield also operated and repaired aircraft from the RAAF, the Royal Navy and units of the Netherlands East Indies forces. Significant buildings on the site include the Interwar Functionalist style terminal building (1941), several interwar hangars and other interwar buildings and two hangars constructed during World War II. History The area immediately surrounding the aerodrome has only been known as Archerfield since 1929. From about 1826, the surrounding district was known as Cowper’s [later Cooper’s] Plains. It was named after the Moreton Bay Penal Settlement’s first medical officer, Dr Henry Cowper, who, during his regular visits to Limestone Hill Date of Citation — April 2008 Page 1 [Ipswich], camped overnight on the government cattle run established on the grassy plains east of Oxley Creek, about 7 miles south of the Brisbane township. The first freehold land in the district was made available in the 1850s while the remaining land was taken up for farming in the 1860s and 1870s. -

COAG National Bushfire Inquiry
Appendix D Fire history in Australia This appendix summarises the available information on major bushfire events in each state and territory as far back as records allow. There are many inconsistencies and gaps in the available information because there are no nationally agreed criteria for defining a ‘significant fire year’ or a ‘major fire event’. The available information shows the following: • Major fire events are a periodic feature in all states and territories. • The areas of land that are affected by fire continue to be significant. • There have been 59 recorded bushfire events where there has been loss of life, with a positive trend being the significant decline in the loss of life from bushfires in the last 20 years. • There have been 24 fire events resulting in major stock losses (defined as more than 1000 head). • There have been 21 fire events resulting in large-scale loss of houses (defined as more than 50 houses). Table D.1 Fire history in Australia, by state and territory No. of Area of fire Date deaths (ha) Losses Location(s) Northern Territory 1968–1969 40 000 000 Killarney – Top Springs 1969–1970 45 000 000 Dry River – Victoria River fire 1974–1975 45 000 000 Barkly Tableland, Victoria River district, near Newcastle Waters 2002 38 000 000 Queensland 1917 3 Large fires near Hughenden, followed by a fire on Warenda Station 1918 October 2 >100 000 sheep Fires spread over a huge area from Charleville to Blackall, Barcaldine, Hughenden 1918 October 5 Saltern Creek 1926 Forests, farms, sugar South-east corner of Queensland -

Tiree in 100 Objects – 63 – Chest
THE HISTORY OF TIREE IN 100 OBJECTS - no. 63 THE SEA CHEST OF DÙGHALL AN ÒIR This wooden sea chest, covered with crocodile skin, was brought back from Australia by Dugald MacKinnon. He was known on Tiree as Dùghall an Òir 'Dugald of the gold', having emigrated to Australia and come back a wealthy man. Dùghall 'ic Nèill 'ic Iain 'Dugald the son of Neil the son of Iain', was born in Taigh an t- Sìthein 'the house of the fairy knoll' in Scarinish in 1840, the son of a boatman. He worked as a contractor and married Mary MacLean, also from Scarinish, when he was thirty-nine. The couple had a daughter, Donaldina, in 1881 and emigrated to Australia three years later. Despite his nickname implying he had made his fortune in the gold rushes, he appears to have worked on a number of stations in the outback of Queensland as the country was opened up to sheep: Adavale, Langlo Downs, Cairns and Toompine. Latterly the family lived in Charleville, 450 miles inland from Brisbane. Tragically, within two years of their arrival Donaldina was dead, and in 1907 Dugald's wife also died. Within months of this loss, he returned to Tiree. He appears to have been well liked, as several letters from old friends in the Queensland bush have survived: "I got your letter alright last week and was very glad to learn that you had reached Tiree in good fettle. I can quite believe that you find many things changed since you were home last … I expect that a good many of you old acquaintances are gone and that you are a greater stranger in Tiree than you are in Charleville.