DIAMOND KNIFE in CATARACT SURGERY*T by DAVIS G
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ophthalmic Surgical Instruments
CIS SELF-STUDY LESSON PLAN Lesson No. CIS 272 (Instrument Continuing Education - ICE) Sponsored by: Ophthalmic Surgical Instruments BY JON WOOD, BAAS, CIS, CRCST, CLINICAL EDUCATOR, IAHCSMM Instrument Continuing Education (ICE) lessons provide members with ongoing education in the complex and ever-changing area of surgical LEARNING OBJECTIVES instrument care and handling. These lessons are 1. Identify common eye instruments used during an eye muscle procedure designed for CIS technicians, but can be of value 2. Review toxic anterior segment syndrome and ways to avoid the postoperative to any CRCST technician who works with surgical inflammatory reaction instrumentation. 3. Discuss the function of eye instrumentation during an eye muscle procedure Earn Continuing Education Credits: Online: Visit www.iahcsmm.org for online grading at a nominal fee. he success of every Central Objective 1: Identify common eye By mail: For written grading of individual lessons, Service/Sterile Processing instruments used during eye muscle send completed quiz and $15 to: (CS/SP) department and, procedures Purdue University - Online Learning ultimately, the success of every Instrumentation can differ from Ernest C. Young Hall, Room 526 155 S. Grant Street Tprocedure performed in surgery, depends healthcare facility to healthcare facility West Lafayette, IN 47907 on the quality of the instruments and is generally selected based upon the provided. Ensuring each surgical surgeon’s specific procedure needs and Scoring: Each quiz graded online at www.iahcsmm.org or through Purdue University, procedure has functional instruments preferences. The following is a list of with a passing score is worth two points (2 contact available and instrument sets that are common eye muscle instrumentation: hours) toward your CIS re-certification (6 points) correct, complete and ready for use when or CRCST re-certification (12 points). -

Product Catalog
precision crafted quality PRODUCT CATALOG www.medicaldevicepurchase.com 1-916-663-4165 2 precision crafted quality A letter from our CEO: Medical Device Purchase is a company started by my father and me almost 10 years ago. We knew the road ahead for MDP would be challenging and that we would inevitably face giant corporations that had been established in the industry for decades. Many said we would not even last two years. However, our approach was different from our competitors. We wanted to create a friendlier environment for healthcare professionals searching for industry-leading surgical products. How? By providing more—and higher quality—options. Our mission was to provide a welcoming environment where customers could enjoy a uniquely approachable buying experience. We wanted to build a brand that focused on creating efficiency and reliability so that our clients could spend more time on the things that really matter. Dr. Ray, our co-founder, passed away earlier this year, but the legacy of Medical Device Purchase lives on as we continue to grow and expand as a cutting edge company blazing new trails in the world of surgical products. Sincerely, Orin Ray www.medicaldevicepurchase.com 3 About MDP WHO WE ARE AND WHAT WE DO Medical Device Purchase is a leading supplier of premium quality surgical products, committed to satisfying the ever-growing demands of the healthcare community. We provide a new level of reliability, efficiency, and value by using applications, performance products, and technology unlike any any other supplier in the the industry. OUR MISSION As the cost of healthcare continues to rise, MDP remain committed to reducing your overhead. -
Equipment for a Colposcopic Examination CHAPTER 1 CHAPTER CHAPTER 5 CHAPTER This Chapter Describes the Which Allows the Colposcope Head to Interference
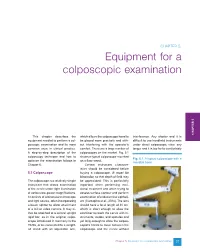
CHAPTER 5. Equipment for a colposcopic examination CHAPTER 1 CHAPTER CHAPTER 5 CHAPTER This chapter describes the which allows the colposcope head to interference. Any shorter and it is equipment needed to perform a col- be placed more precisely and with- difficult to use handheld instruments poscopic examination and its more out interfering with the operator’s under direct colposcopic view; any common uses in clinical practice. comfort. There are a large number of longer and it is too far to comfortably A step-by-step description of the colposcopes on the market. Fig. 5.1 colposcopy technique and how to shows a typical colposcope mounted Fig. 5.1. A typical colposcope with a optimize the examination follows in on a floor stand. movable base. Chapter 6. Certain instrument character- istics should be considered before 5.1 Colposcope buying a colposcope. It must be binocular, so that depth of field may The colposcope is a relatively simple be appreciated. This is particularly instrument that allows examination important when performing exci- of the cervix under light illumination sional treatment and when trying to at various low-power magnifications. assess surface contour and perform It consists of a binocular microscope examination of endocervical epitheli- and light source, often incorporating um (Carcopino et al., 2014). The lens a beam splitter to allow attachment should have a focal length of 30 cm, of a still or video camera. It may ei- which is short enough to allow the ther be attached to a central upright examiner to reach the cervix with in- rigid bar, as in the original colpo- struments, swabs, and spatulas and scope introduced in Germany in the yet long enough to allow the colpos- 1920s, or be connected to a weight- copist’s hands to move between the ed stand with an adjustable arm, colposcope and the cervix without Chapter 5. -

Advanced Surgical Product Catalog
Advanced Surgical Product Catalog To learn more about these and other innovative products, call 866-4CONMED or visit www.CONMED.com Contents Ordering Information ....................................................................... 2 INSTRUMENTS Laparoscopic Instruments ACCESS ® LaparoVue Visibility System ..................................................... 28 ® AirSeal iFS DetachaTip® Instruments .......................................................... 29 iFS Connector for Bottle Gas ....................................................... 4 Disposable Hand Instruments.................................................... 32 iFS Carts, Valves, & Towers ......................................................... 4 Uterine Manipulator High Pressure Hoses for Bottle Gas ............................................. 4 VCare® Plus ............................................................................. 33 iFS Preventative Maintenance and Service Plans .......................... 4 VCare® DX Plus ....................................................................... 33 iFS Connector for House/Central Gas ........................................... 5 Suction/Irrigation iFS Low Pressure Hoses for House/Central Gas ............................ 5 ™ AirSeal® Tube Sets & Access Ports ................................................... 6 Core Suction/Irrigation Systems .............................................. 34 ® BluView™ Trocars .......................................................................... 7 Universal Plus ....................................................................... -

Ethicon Product Catalog Products by Category at Ethicon, We Develop Meaningful Solutions That Enhance Surgical Outcomes and Improve the Lives of Patients
Ethicon Product Catalog Products by Category At Ethicon, we develop meaningful solutions that enhance surgical outcomes and improve the lives of patients. For more than 80 years, we have listened to the voice of our customers, working in partnership with clinicians, hospitals, payors, and other healthcare stakeholders to gain deep experience and perspective into ways to redefine surgery. Our global scope, along with our broad surgical portfolio, let us provide market-appropriate, value-driven solutions that help patients around the world live longer, healthier lives. Access Surgical Stapling Ethicon offers you flexibility across Our surgical stapling portfolio surgical specialties. so you can choose addresses the challenges of tissue the right trocar, with the right level of thickness. tissue movement during performance, when and where it is firing. staple line security, and tissue needed. The ENDOPATH® Trocar Portfolio tension to provide you with greater brings value to every procedure. stapling precision in surgery. 3 48 Adjunctive Hemostats Uterine & The Ethicon portfolio of Adjunctive Hemostats is Pelvic Surgery an area dedicated to aid in surgery by focusing on an array of technologies to minimize bleeding Ethicon has worked with gynecologists to challenges. Solutions comprise innovative, create innovative new solutions for a greater biologically based products for surgical conditions choice of procedure. Enhanced technique that are often difficult or expensive to manage. combined with innovative technologies helps to improve surgical performance. 9 57 Energy Wound Closure With the broadest advanced energy portfolio. Ethicon has pioneered advances Ethicon provides you with unmatched choice in skin closure that enable you to for your laparoscopic and open surgical needs. -

Surgical Instruments
BR SURGICAL • SURGICAL PROCEDURE EXPERTS INSTRUMENTS | SETS ENDOSCOPIC VIDEO EQUIPMENT OVER 20,000 SURGICAL INSTRUMENTS & PROCEDURE SETS ENDOSCOPIC VIDEO EQUIPMENT & RELATED MEDICAL DEVICES SURGICAL BR SURGICAL, LLC • 3500 Beachwood Court • Suite 107 • Jacksonville, Florida 32224 Office: (904) 642-1366 • Fax: (904) 642-1368 • Toll Free: (888) 642-1366 INSTRUMENTS www.brsurgical.com OVER 20,000 SURGICAL INSTRUMENTS & PROCEDURE SETS ENDOSCOPIC VIDEO EQUIPMENT & RELATED MEDICAL DEVICES BR SURGICAL, LLC F Precision crafted German stainless steel instruments F Surgical instrument pattern is equal to or better than industry standard F All instruments put through our stringent inspection process to ensure consistent high quality F Continuous quality improvements F INDUSTRY BEST WARRANTY Surgical instruments are guaranteed to be free of defects in materials and workmanship for the life of the instrument F FREE LIFETIME SHARPENING on Gold Series biopsy punches Customer sends the biopsy punch with return address to BR Surgical and we take care of the rest F Customer issues handled to their complete satisfaction Scan this QR Code with your smartphone or tablet and connect with us online! BR SURGICAL, LLC • 3500 Beachwood Court • Suite 107 • Jacksonville, Florida 32224 Office: (904) 642-1366 • Fax: (904) 642-1368 • Toll Free: (888) 642-1366 www.brsurgical.com CONTENTS Instrument Care . .2 Repair Service . 3 Limited Return Policy . .3 Custom Instruments . .3 Warranty Cross Reference Information . 3 Endoscope Cleaning & Sterilizing Information . .4 Hysteroscopy Video System . .6 BR Surgical, LLC Hysteroscopy Accessories . .7 instruments are Cystoscopy Video System . 8 ENT/Sinus Video System . 9 guaranteed to be Flexible Rhinolaryngoscope Video System . 10 free of defects Flexible Rhinolaryngoscope . -

Obstetrics/Gynecology
OB/GYN Obstetrics/Gynecology Scissors . 638-648 Needle Holders . 649-650 Forceps . 651-682 Clamps. 683-689 Retractors . 690-693 Vaginal Specula . 695-713 Dilators & Probes . 714-718 Curettes. 719-725 Accessories . 726 Obstetrics/Gynecology Scissors WERTHEIM Scissors Catalog Tip Blade Length (in.) Number BC702R B/B CVD 5 3/4 BC703R B/B CVD 8 BC704R B/B CVD 9 BC702R-BC704R 1 /1 BC702R OB/GYN 1 /1 BC703R 1 /1 BC704R SIMS Scissors Catalog Tip Blade Length (in.) Number BC708R B/B CVD 8 1/4 1 BC708R /2 1 /1 638 Obstetrics/Gynecology Scissors SIMS Scissors (continued) Catalog Tip Blade Length (in.) Number BC721R B/B STR 8 BC723R B/B STR 9 BC741R B/B CVD 8 BC743R B/B CVD 9 BC721R-BC743R 1 /1 BC721R OB/GYN 1 /1 BC723R 1 /1 BC741R 1 /1 BC743R 639 Obstetrics/Gynecology Scissors SIMS Scissors Catalog Tip Blade Length (in.) Number BC746R S/B CVD 8 BC748R S/B CVD 9 BC731R S/S STR 8 BC746R-BC748R 1 /1 OB/GYN BC746R 1 /1 BC748R 1 BC731R /2 1 /1 640 Obstetrics/Gynecology Scissors JORGENSEN Scissors Catalog Tip Blade Length (in.) Number MD491 B/B CVD 9 1 MD491 /2 1 /1 OB/GYN SIEBOLD Uterine Scissors Catalog Tip Blade Length (in.) Number BC760R B/B CVD 9 3/4 1 BC760R /2 1 /2 641 Obstetrics/Gynecology Scissors BOZEMANN Uterine Scissors Catalog Tip Blade Length (in.) Number BC761R B/B CVD 8 3/4 1 BC761R /2 1 /2 OB/GYN SIMS-SIEBOLD Uterine Scissors Catalog Tip Blade Length (in.) Number BC762R B/B STR 10 1 BC762R /2 1 /1 642 Obstetrics/Gynecology DUROTIP® TC Scissors DUROTIP TC MAYO Dissecting Scissors Catalog Tip Blade Length (in.) Number BC558R B/B STR 9 -
WHO Technical Guidance and Specifications of Medical Devices For
WHO technical guidance and specifications of medical devices for screening and treatment of precancerous lesions in the prevention of cervical cancer WHO technical guidance and specifications of medical devices for screening and treatment of precancerous lesions in the prevention of cervical cancer ISBN 978-92-4-000263-0 (electronic version) ISBN 978-92-4-000264-7 (print version) © World Health Organization 2020 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization. Suggested citation. WHO technical guidance and specifications of medical devices for screening and treatment of precancerous lesions in the prevention of cervical cancer. -
Euro-Med® • LEEP Non-Conductive Rose-Coated Instruments
STORAGE ® Thoroughly dried instrument(s) should be stored individually in a moisture-free area in a Euro-Med • LEEP Non-Conductive protective tray with partitions. Protect with cloth or gauze if stored in drawers. Rose-Coated Instruments WARRANTY Specula • Retractors • Forceps • Hooks • Tenaculums • Rulers CooperSurgical, Inc., warrants that the LEEP coated instruments (the “Product”) will be free from defects in materials and workmanship for a period of two (2) years from the original Instructions for Use Non-Sterile: sterilize before use date of purchase. If the Product should become inoperable due to a defect in material or DESCRIPTION workmanship during this two-year warranty period, CooperSurgical will, at its option, repair The Euro-Med® LEEP Non-Conductive Rose-Coated Instruments are reusable, manual or replace the Product. This limited warranty does not include replacement or service to instruments designed for use in LEEP procedures in a offi ce or operating room setting. repair damage resulting from improper installation, external electrical fault, accident, disaster, The Euro-Med LEEP Instruments are made from coated stainless-steel and can be sterilized use for a purpose other than that for which originally designed or indicated in this manual, in an autoclave. The Euro-Med LEEP Instruments are available in a variety of styles that negligence, modifi cation, service or repair by personnel not authorized by CooperSurgical or include Specula, Retractors, Forceps, Hooks, Tenaculums and Rulers. Many of the Specula normal wear and tear, and also does not apply to disposable or single- or limited-use items styles include either permanent or disposable smoke evacuator tubing. -

Surgical Instruments
Surgical Instruments McKesson Surgical Instruments are a cost-effective line of instruments ideally suited for routine, minor surgical use in the office setting. Forged from Pakistan stainless steel to offer the precision and durability needed by healthcare professionals, we offer a variety of office-grade instruments, including scissors, needle holders, forceps, scalpels and specula. Features and Benefits • Office Grade: Quality instruments for routine, in-office surgical use • Forged from Pakistan stainless steel to offer precision and durability • Reusable and reliable • Not made with natural rubber latex Never Compromise on Care SM With McKesson Brands, you’ll never have to compromise. We deliver quality If you are not completely satisfied with products at competitive prices, backed by our 100% satisfaction guarantee. any McKesson Brands product, you may We have decades of experience in the market, and we offer you support and return it for a full refund or credit. work to help ensure you have the products you need, when you need them — making it even easier for you to provide the best care for your patients. The product information contained in this document, including the product images and additional product materials, was collected from various supplier sources. All product claims and specifications are those of the product suppliers and have not been independently verified by McKesson Medical-Surgical or its affiliates (“McKesson”). McKesson is not responsible for errors or omissions in the product information. The properties of a product may change or be inaccurate following the posting or printing of the product information in the document, either in the print or online version. -

A Classical Wooden Vaginal Speculum Mentioned in Old Medical Manuscripts
6.DGÖR÷lu, O. Ögenler, ø. Uzel History of Medicine A Classical Wooden Vaginal Speculum Mentioned in Old Medical Manuscripts 6HOLP.DGÕR÷OX0'3K'12\DgJHQOHU0'3K'ƔøOWHU8]HO0'3K'3 Abstract 7KHVXEMHFWRIWKLVSDSHULVWKHVWRU\RIDQDQFLHQWPHGLFDOLQVWUXPHQW7KLVLQVWUXPHQWLVDZRRGHQYDJLQDOVSHFXOXPXVHGLQFODVVLFDODQG ,VODPLFPHGLFLQH,WVGUDZLQJVFDQEHIRXQGLQ$EXOFDVLVDO=DKUDZL¶VDQGùHUHIHGGLQ6DEXQFXR÷OX¶VLOOXVWUDWHGERRNVRIVXUJHU\ Keywords:+LVWRU\RIJ\QHFRORJ\DQGREVWHWULFVKLVWRU\RIPHGLFLQHKLVWRU\RIPHGLFDOLQVWUXPHQWV Cite this article as: .DGÕR÷OX6gJHQOHU28]HOø$FODVVLFDOZRRGHQYDJLQDOVSHFXOXPPHQWLRQHGLQROGPHGLFDOPDQXVFULSWVArch Iran Med. 2017; 193 – 195. Introduction In the 6th FHQWXU\ $HWLXV RI $PLGD >th century] mentioned the vaginal speculum in his works. In the 7th century, Paulus of he word speculum, Latin for “mirror”, is used for devices $HJLQD>FLUFD±@QRWHGHPSOR\LQJWKHYDJLQDOVSHFXOXP T that allow us to examine and treat tubular body parts with a for diagnosis and treatment of cervical diseases and described the OXPHQORFDWHGEH\RQGLQWURGXFWRU\RUL¿FHVE\SXVKLQJWKH medical procedures for treatment of cervix uteri using this device. walls apart from the inside.1 Vaginal speculum is the most In the Islamic medicine, Ali ibn Abbas Majusi Ahvazi (Hally commonly used type. A vaginal speculum enables us to see the $EEDV >FLUFD ± @ GHVFULEHG KRZ WR XVH WKH VSHFXOXP cervix uteri, rendering possible the diagnostic and therapeutic in situations related to gynecological diseases and childbirth. processes related to that part and the inside of the uterus. ,QKLVERRNøEQ6LQD $YLFHQQD >FLUFD±@UHIHUUHGWR Vaginal speculum, the main instrument of gynecological XVHRIDPLUURUUHÀHFWLQJWKHOLJKWZLWKDYDJLQDOVSHFXOXPIRU H[DPLQDWLRQ KDV D ORQJ KLVWRU\ UHÀHFWLQJ WKH FRHYROXWLRQ RI WKH ¿UVW WLPH DQG H[SODLQHG WKH V\PSWRPV DQG WUHDWPHQWV RI medicine and medical technology. It is an interesting device with gynecological diseases.8 All the authors note that the size of the a multitude of variations from the past to the present. -

RICA Surgical Products, Inc
RICA RICA® Surgical Products, Inc. www.ricasurgical.com Surgical Instrument Packs Surgical Instruments TM SteriBest Instrument Trays ® ® Pilling and KMedic Instruments Hemoclip® Ligation Clip System Weck ® Visistat® Skin Staplers Thermal Controlled Products Paw Protector ® Cage Racks Instrument Care Products Instrument Repairs 9207 Ivanhoe Street Schiller Park, Illinois 60176 847-671-5600 1-800-889-3218 Fax: 847-671-5690 © 2018 RICA Surgical Products, Inc. TABLE OF CONTENTS Welcome to RICA Surgical Products, Inc. .................................................................................i Instrument Quality Grades .........................................................................................................ii RICA Surgical Instrument Guarantee / Warranty ..................................................................iii Surgical Instruments Instrument Packs ............................................................................................................. 1 Scissors .............................................................................................................................. 6 Dressing and Tissue Forceps ........................................................................................ 11 Hemostatic Forceps ....................................................................................................... 13 Needle Holders .............................................................................................................. 15 Knife Handles ................................................................................................................