Metallic Biomaterials: Current Challenges and Opportunities
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Comparative Review of Natural and Synthetic Biopolymer Composite Scaffolds
polymers Review A Comparative Review of Natural and Synthetic Biopolymer Composite Scaffolds M. Sai Bhargava Reddy 1 , Deepalekshmi Ponnamma 2 , Rajan Choudhary 3,4,5 and Kishor Kumar Sadasivuni 2,* 1 Center for Nanoscience and Technology, Institute of Science and Technology, Jawaharlal Nehru Technological University, Hyderabad 500085, India; [email protected] 2 Center for Advanced Materials, Qatar University, Doha P.O. Box 2713, Qatar; [email protected] 3 Rudolfs Cimdins Riga Biomaterials Innovations and Development Centre of RTU, Faculty of Materials Science and Applied Chemistry, Institute of General Chemical Engineering, Riga Technical University, Pulka St 3, LV-1007 Riga, Latvia; [email protected] 4 Baltic Biomaterials Centre of Excellence, Headquarters at Riga Technical University, LV-1007 Riga, Latvia 5 Center for Composite Materials, National University of Science and Technology “MISiS”, 119049 Moscow, Russia * Correspondence: [email protected] Abstract: Tissue engineering (TE) and regenerative medicine integrate information and technology from various fields to restore/replace tissues and damaged organs for medical treatments. To achieve this, scaffolds act as delivery vectors or as cellular systems for drugs and cells; thereby, cellular material is able to colonize host cells sufficiently to meet up the requirements of regeneration and repair. This process is multi-stage and requires the development of various components to create the desired neo-tissue or organ. In several current TE strategies, biomaterials are essential compo- nents. While several polymers are established for their use as biomaterials, careful consideration of the cellular environment and interactions needed is required in selecting a polymer for a given Citation: Reddy, M.S.B.; Ponnamma, application. -
Overview of Biomaterials and Their Use in Medical Devices
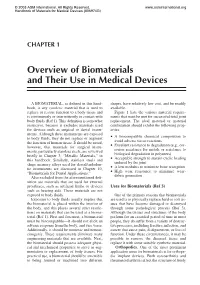
© 2003 ASM International. All Rights Reserved. www.asminternational.org Handbook of Materials for Medical Devices (#06974G) CHAPTER 1 Overview of Biomaterials and Their Use in Medical Devices A BIOMATERIAL, as defined in this hand- shapes, have relatively low cost, and be readily book, is any synthetic material that is used to available. replace or restore function to a body tissue and Figure 1 lists the various material require- is continuously or intermittently in contact with ments that must be met for successful total joint body fluids (Ref 1). This definition is somewhat replacement. The ideal material or material restrictive, because it excludes materials used combination should exhibit the following prop- for devices such as surgical or dental instru- erties: ments. Although these instruments are exposed A biocompatible chemical composition to to body fluids, they do not replace or augment • avoid adverse tissue reactions the function of human tissue. It should be noted, Excellent resistance to degradation (e.g., cor- however, that materials for surgical instru- • rosion resistance for metals or resistance to ments, particularly stainless steels, are reviewed biological degradation in polymers) briefly in Chapter 3, “Metallic Materials,” in Acceptable strength to sustain cyclic loading this handbook. Similarly, stainless steels and • endured by the joint shape memory alloys used for dental/endodon- A low modulus to minimize bone resorption tic instruments are discussed in Chapter 10, • High wear resistance to minimize wear- “Biomaterials for Dental Applications.” • debris generation Also excluded from the aforementioned defi- nition are materials that are used for external prostheses, such as artificial limbs or devices Uses for Biomaterials (Ref 3) such as hearing aids. -

When Does a Material Become a Biomaterial?
When does a material become a biomaterial? Prof. Dr. Ir. Jan Van Humbeeck MTM-K.U.Leuven 1 When it is allowed making contact with human tissue 2 The goal of using biomaterials: Assisting in • Regenerating • Repairing • Supporting • Replacing defect tissues and esthetic parts. 3 Origin of defects in the body • Life quality: – congenital defects – development defects – diseases – accidents – aesthetic reasons • Tissue degeneration due to aging: – Osteoporosis – Hart failure – Wear of joints 4 A problem of aging Czech expression: If you’re over 60 and wake up one morning and nothing hurts, then you’re probably dead. 5 What is a biomaterial? • A biomaterial is a nonviable material used in a (medical) device, intended to interact with biological systems (biofunctionality). (Williams, 1987) • A biomaterial is a material intended to interface with biological systems to evaluate, treat, augment or replace any tissue, organ or function of the body. • A biomaterial is a material that should perform an intended function over a definite amount of time in a specific biological environment, as good as possible. • Biomaterials are inorganic or organic materials that are biocompatible and can be implanted in the human body to replace or repair failing tissue. 6 History of biomaterials • 1° generation-materials: based on replacing tissue or replacing a function with as low as possible interaction with the surrounding tissue. Those materials were found in the classic industrial markets. Those materials were selected because of their corrosion resistance or inertness when in contact with a tissue. • metals: SS, Ti, Co-Cr • polymers: UHMWPE, PMMA, PMDS • ceramics: Al2O3 7 Did Georg Washingthon A false toe made of out of wood and leather had a wooden set of teeth? was found on a 3,000-year-old mummified body of an Egyptian noblewoman Cripple with supporting pole. -

48-51 Characterization Martensitic Stainless Steel Surgica.Pdf
CHARACTERIZATION OF LOCALLY PRODUCED MARTENSITIC STAINLESS STEEL SURGICAL GRADE AISI 420A By Muhammad Kamran, Faraz Hussain, Taqi Zahid Butt, Fahad Riaz* Abstract The Martensitic stainless steel surgical grade AISI 420A is one of the major alloys being used in the production of surgical instruments in Pakistan. Till today, this alloy is being imported from Japan and France. Recently this grade has been developed in Pakistan. In this study this locally produced Martensitic stainless steel surgical grade AISI 420A was investigated. The sheet samples were tested for their composition, heat treated by austenizing at 1000 + 20°C, 0 quenched in N2 gas followed by tempering at 200 C and finally tested for their mechanical properties. It was observed that chemical composition fall within the standard composition with minor changes. It was also observed that hardness and tensile properties are within range. Introduction Pakistan is one of the largest countries producing and supplying surgical instruments all over the world. Tonnages of raw material are required for the production purposes. Surgical industry of Pakistan holds a history of more than 100 years, when some British doctors got their surgical instruments repaired from the skilled workers of Sialkot and that was the foundation of Sialkot surgical industry. [1] Surgical Instruments Manufacturers Association of Pakistan (SIMAP) was established during 1958 with an aim to help solving the problems of surgical community. Surgical association has more than 2300 members till date, who are grossly engaged in manufacturing of surgical instruments to meet their export commitments in the International Market. The value of exports of surgical instruments for the financial year 2007-2008 was US $255 Million. -

Biomaterial Scaffolds in Pediatric Tissue Engineering
0031-3998/08/6305-0497 Vol. 63, No. 5, 2008 PEDIATRIC RESEARCH Printed in U.S.A. Copyright © 2008 International Pediatric Research Foundation, Inc. Biomaterial Scaffolds in Pediatric Tissue Engineering MINAL PATEL AND JOHN P. FISHER Fischell Department of Bioengineering, University of Maryland, College Park, Maryland 20742 ABSTRACT: This article reviews recent developments and major immune system is not completely developed. However, pedi- issues in the use and design of biomaterials for use as scaffolds in atric patients have exhibited a higher regenerative capacity com- pediatric tissue engineering. A brief history of tissue engineering and pared with adults because younger cells have undergone less the limitations of current tissue-engineering research with respect to stress and age damage. This review studies novel biomaterials as pediatric patients have been introduced. An overview of the charac- scaffolds and pediatric tissue-engineering applications. teristics of an ideal tissue-engineering scaffold for pediatric applica- tions has been presented, including a description of the different types of scaffolds. Applications of scaffolds materials have been high- CHARACTERISTICS OF AN IDEAL SCAFFOLD lighted in the fields of drug delivery, bone, cardiovascular, and skin tissue engineering with respect to the pediatric population. This Before developing a scaffold for any tissue-engineering review highlights biomaterials as scaffolds as an alternative treatment application, the material and biologic properties have to be method for pediatric surgeries due to the ability to create a functional evaluated. Initially, depending upon the application, mechan- cell-scaffold environment. (Pediatr Res 63: 497–501, 2008) ical properties should be studied keeping in mind the sur- rounding environment of the scaffold once placed in an in vivo he field of tissue engineering involves replacement of system. -

Mechanical Properties of Biomaterials
Mechanical Properties of Biomaterials Academic Resource Center Determining Biomaterial Mechanical Properties • Tensile and Shear properties • Bending properties • Time dependent properties Tensile and Shear properties • Types of forces that can be applied to material: a) Tensile b) Compressive c) Shear d) Torsion Tensile Testing • Force applied as tensile, compressive, or shear. • Parameters measured: Engineering stress (σ) and Engineering strain (ԑ). • σ = F/A0 : Force applied perpendicular to the cross section of sample • ԑ = (li-l0)/l0: l0 is the length of sample before loading, li is the length during testing. Compression Testing • Performed mainly for biomaterials subjected to compressive forces during operation. E.g. orthopedic implants. • Stress and strain equations same as for tensile testing except force is taken negative and l0 larger than li. • Negative stress and strain obtained. Shear Testing • Forces parallel to top and bottom faces • Shear stress (τ) = F/A0 • Shear strain (γ)= tanθ ; θ is the deformation angle. • In some cases, torsion forces may be applied to sample instead of pure shear. Elastic Deformation • Material 1: Ceramics • Stress proportional to strain. • Governed by Hooke’s law: σ = ԑE; τ=Gγ • E :Young’s modulus G: Shear modulus - measure of material stiffness. • Fracture after applying small values of strain: ceramics are brittle in nature. Elastic and Plastic deformation. • Material 2: Metal • Stress proportional to strain with small strain; elastic deformation. • At high strain, stress increases very slowly with increased strain followed by fracture: Plastic deformation. Elastic and Plastic deformation. • Material 3: Plastic deformation polymer • Stress proportional to strain with small strain; elastic deformation. • At high strain, stress nearly independent of strain, shows slight increase: Plastic deformation. -

Silk-Based Biomaterials for Tissue Engineering
C H A P T E R 1 Silk-based Biomaterials for Tissue Engineering V. Kearns, A.C. MacIntosh, A. Crawford and P.V. Hatton* Summary ilks are fibrous proteins, which are spun by a variety of species including silkworms and spiders. Silks have common structural components and have a hierarchical structure. Silkworm silk must be S degummed for biomedical applications in order to remove the immunogenic sericin coating. It may subsequently be processed into a variety of forms, often via the formation of a fibroin solution, including films, fibres and sponges, and used in combination with other materials such as gelatine and hydroxyapatite. Spider silks do not have a sericin coating and may be used in natural fibre form or processed via formation of a spidroin solution. Both silkworm and spider silks have been reported to support attachment and proliferation of a variety of cell types. Silks have subsequently been investigated for use in tissue engineering. This chapter provides a general overview of silk biomaterials, discussing their processing, biocompatibility and degradation behaviour and paying particular attention to their applications in tissue engineering. KEYWORDS: Silk; Fibroin; Spidroin; Tissue engineering. *Correspondence to: Professor Paul V Hatton, Centre for Biomaterials & Tissue Engineering, School of Clinical Dentistry, University of Sheffield, Claremont Crescent, Sheffield, S10 2TA, UK. Email: [email protected] Tel: +44 (114) 271 7938 Fax: +44 (114) 279 7050. Topics in Tissue Engineering, Vol. 4. Eds. N Ashammakhi, R Reis, & F Chiellini © 2008. Kearns et al. Silk Biomaterials 1. INTRODUCTION Silks are fibrous proteins, which are spun into fibres by a variety of insects and spiders [1]. -
Physical Property Testing Equipment for Biomaterials and Medical Applications C220-E010
Physical Property Testing Equipment for Biomaterials and Medical Applications C220-E010 Contributing to the Development and Reliability of Advanced Medical Treatments Physical Property Testing Equipment for Biomaterials and Medical Applications Company names, product/service names and logos used in this publication are trademarks and trade names of Shimadzu Corporation or its affiliates, whether or not they are used with trademark symbol “TM” or “®”. Third-party trademarks and trade names may be used in this publication to refer to either the entities or their products/services. Shimadzu disclaims any proprietary interest in trademarks and trade names other than its own. For Research Use Only. Not for use in diagnostic procedures. The contents of this publication are provided to you “as is” without warranty of any kind, and are subject to change without notice. Shimadzu does not assume any responsibility or liability for any damage, whether direct or indirect, relating to the use of this publication. www.shimadzu.com/an/ © Shimadzu Corporation, 2013 Printed in Japan 3655-10225-30AIT Shimadzu Material Testing Machines Support the Development of Advanced Medical Treatments Although the world's population was just two billion in 1927, it reached seven billion in 2011 and is expected to hit ten billion by the end of the 21st century. Advanced countries such as Japan are becoming aging societies. Autograph AG Series EZTest Series Autograph AGS Series Autograph AG Series Such dramatic growth in population and life-expectancy is said to result from more sophisticated medicine, Precision Universal Tester, Table-Top Type Compact Table-Top Universal Tester Precision Universal Tester, Table-Top Type Precision Universal Tester, Floor Type which, in turn, will require more advanced medical technology. -

Bioceramic Materials
Bioceramic Materials María González Esguevillas MacMillan Group Meeting April 18, 2019 Introduction to Bioceramics Bioceramic: Any ceramic, glass, or glass-ceramic used as a biomaterial, which is a material intended to interface with biological systems to evaluate, treat, augment, or replace any tissue, organ, or function of the body. bio- -ceramic greek [keramikos] greek [bios] — relating to products made from clay, — life — pottery and brick — Baino, F. et al Frontiers in Bioeng. and Biotech. 2015, 3, 202 Yeoh, F-Y. et al J. Biomaterials App. 2011, 27, 345. Introduction to Bioceramics Bioceramic: A large class of specially designed ceramics for the repair and reconstruction of diseased or damaged parts of the body BONES TISSUES Why are important? What is the difference between these treatments and others? Baino, F. et al Frontiers in Bioeng. and Biotech. 2015, 3, 202 Yeoh, F-Y. et al J. Biomaterials App. 2011, 27, 345. Introduction to Bioceramics WhyBioceramic: are important? BONESA large class of specially designed ceramics for the repair and reconstruction of diseased or damagedTISSUES What is the difference partsbetween of the these body treatments and others? DISEASE TREATMENTS Causes: virus, bacteria, autoimmune, cancer, genetic diseases Target identification Treatment Baino, F. et al Frontiers in Bioeng. and Biotech. 2015, 3, 202 Yeoh, F-Y. et al J. Biomaterials App. 2011, 27, 345. Introduction to Bioceramics WhyBioceramic: are important? BONESA large class of specially designed ceramics for the repair and reconstruction of diseased or damagedTISSUES What is the difference partsbetween of the these body treatments and others? Composition Diseases 25 % water Fractures 30 % Organic mineral: Osteoporosis cells (osteoblast, osteoclast, osteocytes, Osteomyelitis connective tissue) and collagen Osteosarcoma (cancer) 45 % Inorganic mineral calcium phosphates (HA) and carbonates Hyp dysplasia What was the solution for these diseases? capable to regenerate tissues Baino, F. -

GORE ® ENFORM Biomaterial
OPTIMAL HANDLING AND TISSUE RESPONSE GORE® ENFORM Biomaterial Comprised of synthetic bioabsorbable polyglycolic acid (PGA) and trimethylene carbonate (TMC) copolymer. Completely absorbed, leaving no material behind in the body. Uniquely flexible material Textured surface to improve conformability Material thickness of 2.2 mm 20X Fluid 10–100 µm transfer pore size DESIGNED for optimal Angiogenic1,2 tissue infiltration and fluid transfer Cellular infiltration Small to medium caliber blood vessels throughout Collagen deposition Mature, organized collagen Optimized conformability Unprecedented flexibility of a synthetic soft tissue reinforcement. Conforms to match anatomy and better accommodate the surgeon’s choice of technique. GORE® ENFORM Preperitoneal Biomaterial Feel the difference Comments from surgeons after handling the product in simulated use conditions: Very soft, very friendly handling.” “ Very pliable, don’t think the patient would feel the device at all.” “ Handles easily, pliable, easy to suture wet or dry.” “ Very cloth-like feel, almost feels like cotton fibers. “ Feels easy to handle both wet and dry.” Material is pretty solid, I like it.” “ Feels soft, sutures easy but still solid, very confident.” “ The GORE® ENFORM Biomaterial is designed to reinforce soft tissue during the phases of wound healing by filling soft-tissue deficits. Typical procedures include: • Abdominal wall reconstruction • Hernia repair • Muscle flap (i.e. TRAM, DIEP) procedures 3D matrix ENGINEERED to work with the body during the critical healing phase Tissue healing • Optimal handling • Rapid, high quality tissue promotion • Full and predictable absorption 30 90 180 days days days Device implant site Device Device Muscle 500 µm 500 µm 500 µm Muscle Infiltration Integration Regeneration to enable vascularization to support healthy tissue to leave only healthy tissue formation Uniform, mature collagen replaces the bioabsorbable matrix*, 2 * Results may not correlate to clinical performance in humans. -

Biomaterials Science: a Multidisciplinary Endeavor Buddy D
I NTRODUCTION Biomaterials Science: A Multidisciplinary Endeavor Buddy D. Ratner, Allan S. Hoffman, Frederick J. Schoen, Jack Lemons or implants. Although this is a text on materials, it will quickly BIOMATERIALS AND BIOMATERIALS SCIENCE become apparent that the subject cannot be explored without also considering biomedical devices and the biological response Biomaterials Science: An Introduction to Materials in to them. Indeed, both the effect of the materials/device on the Medicine addresses the properties and applications of materials recipient and that of the host tissues on the device can lead to (synthetic and natural) that are used in contact with biologi- device failure. Furthermore, a biomaterial must always be con- cal systems. These materials are commonly called biomaterials. sidered in the context of its final fabricated, sterilized form. For Biomaterials, an exciting field with steady, strong growth example, when a polyurethane elastomer is cast from a solvent over its approximately half century of existence, encompasses onto a mold to form the pump bladder of a heart assist device, it aspects of medicine, biology, chemistry, and materials science. can elicit different blood reactions than when injection molding It sits on a foundation of engineering principles. There is also a is used to form the same device. A hemodialysis system serv- compelling human side to the therapeutic and diagnostic appli- ing as an artificial kidney requires materials that must function cation of biomaterials. This textbook aims to (1) introduce in contact with a patient’s blood and also exhibit appropriate these diverse elements, particularly focusing on their interrela- membrane permeability and mass transport characteristics. -
Molybdenum at Work in the Dentist's Office
Molybdenum at work in the dentist’s office Dental instruments need to be hard for the dentist to work efficiently and precisely, and tough enough not to break during procedures. At the same time they have to be hygienic, corrosion resistant and easily sterilized. The molybdenum-containing hardenable surgical stainless steel Type 440A fits these requirements and new, even harder and tougher grades are on the horizon. Dentists recommend a semiannual curettes and probes need a sharp life between sharpening and reduces check-up and a visit to the hygienist. edge to reduce the pressure exerted by the total maintenance time. Regular flossing and brushing can help the dentist, helping to avert damage slow the accumulation of plaque and to the patient’s teeth or the tool itself. Dull As in all medical practices, hygiene is tartar, but only dental hygienists can dental tools are more difficult to work key for safe and successful procedures. effectively reach small crevices between with. They reduce control, and with that, Dental tools are sterilized after each the teeth and clean near the gum the quality and precision of the work. They use, usually with high-temperature steam line. To accomplish this and many other also require more time for a procedure, under pressure in an autoclave, with tasks, they often use tools made of increasing fatigue of the practitioner, not dry heat or with chemical vapor. Stainless a hardenable molybdenum-containing to mention that of the patient. Periodic steel does not corrode in any of these stainless steel. sharpening is therefore an essential part procedures.