Healthcare in North Wales Is Changing
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Flintshire County Council Roadworks Bulletin
Flintshire County Council Roadworks Bulletin Streetscene and Trasportation Tel: 01352 701234 25/10/2019 - 01/11/2019 Email: [email protected] Category Work Type Contractor Location Start Date End Date Route No View on Map Highways Maintenance Flintshire C C / Cynnal a Chadw Streetscene Services High Street, Holywell 27-08-2019 29-11-2019 View on Map [Link] Road Closure / Cau Priffyrdd 01352 701234 ffordd Lawson Civil Construction & Engineering and Kiln Lane, Hope, Development / 30-09-2019 08-11-2019 B5373 View on Map [Link] Temporary Traffic Utilities Ltd - 0800 0831 Wrexham, UK Adeiladu a Datblygu Lights (2 Way) / 296 Goleuadau Traffig Dros Dro (2 ffordd) Highways Maintenance Ashtead Plant Hire Mold to New Brighton, / Cynnal a Chadw 21-10-2019 28-10-2019 A541 View on Map [Link] Company 08700 500792 Flintshire Priffyrdd Lane Closure / Cau Lôn Highways Maintenance Flintshire CC Wepre lane, Connahs / Cynnal a Chadw Streetscene Services 28-10-2019 29-10-2019 View on Map [Link] Quay/Northop Hall Road Closure / Cau Priffyrdd 01352 701234 ffordd Gas Utility Works / Wales & West Utilities Old A494 Cut Off 21-10-2019 11-11-2019 Temporary Traffic Gwaith Nwy 0845 371 5050 Unadopted, Mold View on Map [Link] Lights (2 Way) / Goleuadau Traffig Dros Dro (2 ffordd) Gas Utility Works / Wales & West Utilities Ruthin Road, Mold, UK 21-10-2019 26-11-2019 View on Map [Link] Temporary Traffic Gwaith Nwy 0845 371 5050 Lights (2 Way) / Goleuadau Traffig Dros Dro (2 ffordd) Highways Maintenance Flintshire CC Wepre Lane, Deeside, / Cynnal a Chadw -

INDEX to LEAD MINING RECORDS at FLINTSHIRE RECORD OFFICE This Index Is Not Comprehensive but Will Act As a Guide to Our Holdings
INDEX TO LEAD MINING RECORDS AT FLINTSHIRE RECORD OFFICE This index is not comprehensive but will act as a guide to our holdings. The records can only be viewed at Flintshire Record Office. Please make a note of all reference numbers. LOCATION DESCRIPTION DATE REF. NO. Aberduna Lease. 1872 D/KK/1016 Aberduna Report. 1884 D/DM/448/59 Aberdune Share certificates. 1840 D/KK/1553 Abergele Leases. 1771-1790 D/PG/6-7 Abergele Lease. 1738 D/HE/229 Abergele See also Tyddyn Morgan. Afon Goch Mine Lease. 1819 D/DM/1206/1 Anglesey Leases of lead & copper mines in Llandonna & Llanwenllwyfo. 1759-1788 D/PG/1-2 Anglesey Lease & agreement for mines in Llanwenllwyfo. 1763-1764 D/KK/326-7 Ash Tree Work Agreement. 1765 D/PG/11 Ash Tree Work Agreement. 1755 D/MT/105 Barber's Work Takenote. 1729 D/MT/99 Belgrave Plan & sections of Bryn-yr-orsedd, Belgrave & Craig gochmines 19th c D/HM/297-9 Belgrave Section. 1986 D/HM/51 Belgrave Mine, Llanarmon License to assign lease & notice req. performance of lease conditions. 1877-1887 D/GR/393-394 Billins Mine, Halkyn Demand for arrears of royalties & sale poster re plant. 1866 D/GR/578-579 Black Mountain Memo re lease of Black Mountain mine. 19th c D/M/5221 Blaen-y-Nant Mine Co Plan of ground at Pwlle'r Neuad, Llanarmon. 1843 D/GR/1752 Blaen-y-Nant, Llanarmon Letter re takenote. 1871 D/GR/441 Bodelwyddan Abandonment plans of Bodelwyddan lead mine. 1857 AB/44-5 Bodelwyddan Letter re progress of work. -
Appendix 2 of Draft Proposals
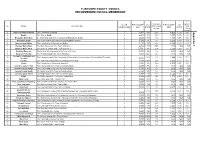
FLINTSHIRE COUNTY COUNCIL RECOMMENDED COUNCIL MEMBERSHIP % % variance variance No. OF ELECTORATE 2018 ELECTORATE 2023 No. NAME DESCRIPTION from County from COUNCILLORS 2018 RATIO 2023 RATIO average County average 1 Argoed and New Brighton The Community of Argoed 2 4,564 2,282 26% 4,856 2,428 29% 3 Appendix 2 Bagillt The Town of Bagillt 2 3,201 1,601 -12% 3,269 1,635 -13% 3 Broughton North East the North East ward of the Community of Broughton & Bretton 1 1,693 1,693 -6% 1,706 1,706 -10% 4 Broughton South The South ward of the Community of Broughton & Bretton 2 3,350 1,675 -7% 3,359 1,680 -11% 5 Brynford and Halkyn The Communities of Brynford and Halkyn 2 3,173 1,587 -12% 3,239 1,620 -14% 6 Buckley: Bistre East The Bistre East ward of the Town of Buckley 2 3,262 1,631 -10% N/A N/A N/A 7 Buckley: Bistre West The Bistre West ward of the Town of Buckley 2 3,230 1,615 -11% 3,566 1,783 -5% 8 Buckley: Mountain The Buckley Mountain ward of the Town of Buckley 1 2,049 2,049 13% N/A N/A N/A 9 Buckley: Pentrobin The Pentrobin ward of the Town of Buckley 2 4,063 2,032 12% N/A N/A N/A Caergwrle, Llanfynydd and 10 The Caergwrle ward of the Community of Hope and the Communities of Llanfynydd and Treuddyn 2,028 12% 4,180 2,090 11% Treuddyn 2 4,055 11 Caerwys The Town of Caerwys and the Community of Ysceifiog 1 2,018 2,018 12% 2,176 2,176 15% 12 Cilcain The Commuities of Cilcain and Nannerch 1 1,526 1,526 -16% 1,547 1,547 -18% 13 Connah's Quay Central The Central ward of the Town of Connah's Quay 2 3,509 1,755 -3% N/A N/A N/A 14 Connah's Quay: Golftyn -

Key Messages Setting the Future Direction for the Plan
Flintshire Local Development Plan March 2016 Key Messages Setting the future direction for the Plan. Tell us what you think. Contents 1. Introduction p3 2. Where are we now? p3 3. Where are we trying to get to? p4 4. The vision for the Plan p4 5. The issues facing the Plan p5 - Enhancing community life p5 - Delivering growth and prosperity p10 - Safeguarding the environment p15 6. The objectives for the Plan p19 7. Moving forward p21 8. Settlement categorisation p23 - Settlement surveys p23 - Settlement categorisation options p24 9. Next Steps p26 10. How to comment p27 Appendices: 1. Discussion Paper – settlement surveys and the formulation of a basic settlement banding p28 2. Discussion Paper – settlement categorisation options p43 Flintshire Local Development Plan | Key Messages Document 2 Flintshire Local Development Plan. Key Messages – Setting the direction for the Plan. Tell us what you think. 1 - Introduction 1.1 - The Council is preparing a Local Development Plan (LDP) to cover the 15 year period 2015 to 2030 and when adopted this will replace the adopted Unitary Development Plan (UDP). The LDP will contain policies and proposals which together will provide for the development needs of the County over the Plan period as well as protecting the social and environmental assets of the County. 2 - Where are we now? 2.1 - The Council is in the early stages of Plan preparation and the various stages are set out in the Council’s Delivery Agreement. A summary of progress to date is set out below: • undertaken a Call for Candidate Sites -

51 Eifl Road , Trefor, LL54 5HG £105,000
51 Eifl Road , Trefor, LL54 5HG £105,000 ■ Former Quarrymans Cottage ■ Small Rural Village ■ Convenient for Pwllheli & Caernarfon ■ Two Bedrooms & Large Landing ■ Front Garden ■ Available Immediately 51 Eifl Road , Trefor, LL54 5HG This inner terrace, former quarrymans cottage, is offered for sale by Tudor Estate Agents & Chartered Surveyors. The property is located in the centre of the village which is convenient for commuting to Pwllheli and Caernarfon and on the north coast of the glorious Llyn Peninsula. The cottage briefly comprises the following:‐ Lounge. Kitchen. Utility. Bathroom. Large study landing. Two bedrooms. Easily maintained garden to the front. GROUND FLOOR Lounge 11'11 x 15'1 (3.63m x 4.60m) Night storage heater. Open beams. Stairs to first floor. Door to: Kitchen 12'3 x 8'10 (3.73m x 2.69m) Maximum measurements to recess. Door to: Utility 8'0 x 8'2 (2.44m x 2.49m) Single drainer stainless steel sink unit. Outside door. Door to: Bathroom 4'1 x 8'2 (1.24m x 2.49m) Low level w.c. Panelled bath. Pedestal washbasin. Cylinder for hot water. FIRST FLOOR Landing 12'0 x 6'9 (3.66m x 2.06m) Now used as an office study area. Night storage heater. Front Bedroom 11'10 x 7'10 (3.61m x 2.39m) Rear Bedroom 12'3 x 8'9 (3.73m x 2.67m) OUTSIDE Front garden. SERVICES We understand that mains water, electricity and drainage are connected to the property. Prospective purchasers should make their own enquiries as to the suitability and adequacy of these services. -

DP-1689-16-21 Letter to All Assembly Members from Ken Skates AM In
Ken Skates AC/AM Ysgrifennydd y Cabinet dros yr Economi a Thrafnidiaeth Cabinet Secretary for Economy and Transport Eich cyf/Your ref Ein cyf/Our ref: MA-P-KS-0544-18 To All Assembly Members 21 March 2018 Dear Friend In February I announced Active Travel funding of £8.1m, and a total of fifty-four active travel and road safety schemes across Wales received a share of the funding made available. Since this announcement I am pleased to confirm that a further £700,000 has been awarded to Local Authorities for active travel schemes. This funding will accelerate delivery of a range of active travel improvements linked to Welsh Government transport priorities in support of the landmark Active Travel (Wales) Act 2013. A list of all the funding for active travel schemes awarded to Local Authorities is attached to this letter for your information. Yours sincerely Ken Skates AC/AM Ysgrifennydd y Cabinet dros yr Economi a Thrafnidiaeth Cabinet Secretary for Economy and Transport Canolfan Cyswllt Cyntaf / First Point of Contact Centre: Bae Caerdydd • Cardiff Bay 0300 0604400 Caerdydd • Cardiff [email protected] CF99 1NA [email protected] Rydym yn croesawu derbyn gohebiaeth yn Gymraeg. Byddwn yn ateb gohebiaeth a dderbynnir yn Gymraeg yn Gymraeg ac ni fydd gohebu yn Gymraeg yn arwain at oedi. We welcome receiving correspondence in Welsh. Any correspondence received in Welsh will be answered in Welsh and corresponding in Welsh will not lead to a delay in responding. 2017-18 - In-year Active Travel funding Schemes approved for funding Local Authority Scheme Name Scheme Amount Brief Scheme Details Grant Allocated £ Bridgend Croesty & Pencoed SRIC 75,000 Widening of section of footway on Northern side of Coychurch Road, vegetation clearance along footway Southern side of Coychurch Road and enhanced lighting along Coychurch Road. -

Consideration of Candidate Sites Against the Preferred Strategy/ Invitation for Alternative Sites
Flintshire Local Development Plan 2015 - 2030 Preferred Strategy Consultation Document Background Paper Consideration of Candidate Sites against the Preferred Strategy/ Invitation for Alternative Sites November 2017 Introduction Site Assessment Methodology The Local Development Plan (LDP) will contain planning policies to guide development and The Council are using a four stage process as a methodology for the assessment of Candidate land use allocations to meet the development needs in Flintshire up to 2030. In addition it sets Sites which can be summarised as follows: out the policy framework for making decisions on planning applications. • Initial filtering of sites by size and proposed land use; This Background Paper has been published alongside the Preferred Strategy document in • Detailed appraisal of filtered sites; order to identify whether or not each Candidate Site broadly complies with the strategic • Assessment against the plans Preferred Strategy in terms of the level and distribution of approach to the location of future growth as set out within the LDP Preferred Strategy. It also growth; and provides an opportunity for interested groups, organisations and persons to make comments • Assessment of sites against other studies such as the Local Housing Market on those Candidate Sites put forward for development. Later on in the document guidance is Assessment study together with the Sustainability Appraisal. given as to how to make comments on the sites together with an indication of the type of representations the Council are seeking. It should be noted that these stages are not mutually independent of each other but rather the assessment process is an on-going iterative process as the preparation of the plan progresses. -

Centenary 1909 -2009
Centenary 1909 -2009 MOLD GOLF CLUB Cilcain Road, Pantymwyn, Nr Mold, Flintshire CH7 5EH Competitions Greens Committee Committee Telephones: 01352 741513 (Clubhouse); 01352 740318 (Professional) E-mail: [email protected] Peter Roach Les Jeffcott Colin Jones Barry Brine Barry Haigh Keith Chamberlin CENTENARY YEAR 2009 OFFICERS Keith Chamberlin Bob Dukeson Gordon Hughes Nev George Ladies’ representa- J Dewi Ingman tive Iestyn Ingman Dewi W Ingman House Committee J Richard Jones Tony Moore Don Farrington Bob Naybour Mike Hayes Rishi Sharma Brian Clarke Roger Howes Mike Worsnip Mike Jones Finance Ladies’ representa- Committee tive Stephen Jones Social Committee Roy Fisher Janet Spence David Thurston Barry Haigh Roy Fisher Richard Jones Management Committee: Back row, from Don Farrington (House Chairman). Glyn Evans Jim Mash left: Peter Roach (Greens Chairman), Front row, from left: Margaret Ellis Margaret Ellis Dave Stephens J Dewi Ingman, Stephen Jones (Finance (Lady Vice-Captain); Martyn Norma Newall Tim Davies Chairman), Chris Mills (Secretary/Man- Scholes (Captain), Dave Ashworth Angela Morris Gaynor Jones ager), Dave Faulkner, Les Jeffcott (President), Elizabeth Harrison (Lady Tony Moore Charles Bull (Competitions Chairman), Tudor Hughes, Captain); Glyn Evans (Vice-Captain). Joy Burton Don Layfield Irene Leech Cover picture by Mike Worsnip 2 Captains’ foreword T WAS a great honour and privilege to be elected as the hours of editing which have culminated in the production of Captains of Mold Golf Club on the occasion of the club’s this unique book. It will serve as a lasting tribute to those hun- ICentenary Year. Thanks should be accorded to the founders dreds of committed members who over the century have freely for establishing the club and to all the members and staff over given their hearts and minds, the labour of their hands and not the last hundred years for all their conscientious work which infrequently the contents of their pockets “for the club” as they has given us today a golf course of which we can all be proud. -

Land Adjacent to Lilac Cottage, Sychdyn, Flintshire
CPAT Report No. 1438 Land Adjacent to Lilac Cottage, Sychdyn, Flintshire Archaeological Evaluation YMDDIRIEDOLAETH ARCHAEOLEGOL CLWYD-POWYS CLWYD-POWYS ARCHAEOLOGICAL TRUST Client name: Mr A Roberts CPAT Project No: 2131 Project Name: Land adjacent to Lilac Cottage Grid Reference: SJ 24643 66548 County/LPA: Flintshire CPAT Report No: 1438 Event PRN: 140125 Report status: Final Confidential: Yes Prepared by: Checked by: Approved by: Ian Grant Nigel Jones Nigel Jones Principal Archaeologist Principal Archaeologist Senior Archaeologist 5 August 2016 8 August 2016 8 August 2016 Bibliographic reference: Grant, I., 2016. Land adjacent to Lilac Cottage, Sychdyn, Flintshire: Archaeological Evaluation. CPAT Report No. 1438. YMDDIRIEDOLAETH ARCHAEOLEGOL CLWYD-POWYS CLWYD-POWYS ARCHAEOLOGICAL TRUST 41 Broad Street, Welshpool, Powys, SY21 7RR, United Kingdom +44 (0) 1938 553 670 [email protected] www.cpat.org.uk ©CPAT 2016 The Clwyd-Powys Archaeological Trust is a Registered Organisation with the Chartered Institute for Archaeologists CPAT Report No 1438 Land adjacent to Lilac Cottage, Sychdyn Archaeological Evaluation CONTENTS SUMMARY ................................................................................................................................................... II 1 INTRODUCTION ................................................................................................................................. 1 2 HISTORICAL BACKGROUND ............................................................................................................... -

Pen Pentre SYCHDYN
Pen Pentre SYCHDYN An exclusive development of 2, 3, 4 and 5 bedroom family homes 1 A wonderful place to call home Located just over a mile from Mold, Stewart Milne’s latest collection of family homes enjoys a host of excellent amenities and transport links to towns throughout North Wales and Cheshire. There are good schools nearby, a convenience store with a post office and a congenial hostelry. Virtually on your doorstep are some of the most beautiful walks in North Wales. In this enviable setting, Stewart Milne Homes have created a new community, completely complementary to the local environment. Designed by the company’s award-winning architects, Pen Pentre is a stunning collection of spacious, light and airy homes, each positioned to take full advantage of its surroundings. 2 1 Nothing beats coming home to Pen Pentre If, at weekends, you like to cast off your working clothes and get out into the countryside, Sychdyn is the ideal spot. Moel Famau, the highest hill in the Clwydian range, is only ten miles away. The Dee Estuary is a haven for wildlife. Throughout Flintshire there are wild, upland heaths, quiet riversides and wooded valleys you can never get tired of exploring. At Stewart Milne Homes, we never That’s why this brochure includes not forget that a home isn’t just where you only the details you’d expect – sizes, live, it’s how you live. And that moving specifications and styles – but also to a new home is a fresh, exciting start shows something of the life you’ll live at – and often one of life’s most exciting Pen Pentre. -
PLACE-NAMES of FLINTSHIRE
1 PLACE-NAMES of FLINTSHIRE HYWEL WYN OWEN KEN LLOYD GRUFFYDD 2 LIST A. COMPRISES OF THE NAMED LOCATIONS SHOWN ON THE ORDNANCE SURVEY LANDRANGER MAPS, SCALE 1 : 50,000 ( 2009 SELECTED REVISION ). SHEETS 116, 117, 126. 3 PLACE-NAMES NGR EARLY FORM(S) & DATE SOURCE / COMMENT Abbey Farm SJ 0277 The Abby 1754 Rhuddlan PR Plas newydd or Abbey farm 1820 FRO D/M/830. Plas Newydd or Abbey Farm 1849 FRO D/M/804. Aberduna SJ 2062 Dwi’n rhyw amau nad yw yn Sir y Fflint ? Aberdunne 1652 Llanferres PR Aberdynna 1674 “ “ Aberdynne 1711 “ “ Aberdinna 1726 “ “ Aber Dinna 1739 “ “ Aberdyne 1780 “ “ Aberdine 1793 “ “ Abermorddu SJ 3056 Abermoelduy 1378 CPR,1377-81, 233. Aber mole (sic) 1587 FRO, D/GW/1113. Aber y Moel du 1628 BU Bodrhyddan 719. Abermorddu 1771 Hope PR Abermorddu 1777 Hope PR Abermordy 1786 Hope PR Abermorddu 1788 Hope PR Abermordy 1795 Hope PR Abermorddy 1795 John Evans’ Map. Abermordey 1799 Hope PR Abermorddu 1806 Hope PR Abermorddy 1810 Hope PR Abermorddu 1837 Tithe Schedule Abermorddu 1837 Cocking Index, 13. Abermorddu 1839 FHSP 21( 1964 ), 84. Abermorddu 1875 O.S.Map. [ Cymau ] Referred to in Clwyd Historian, 31 (1993 ), 15. Also in Hope Yr : Aber-ddu 1652 NLW Wigfair 1214. Yr Avon dhŷ 1699 Lhuyd, Paroch, I, 97. Yr Aberddu 1725 FHSP, 9( 1922 ), 97. Methinks where the Black Brook runs into the Alun near Hartsheath ~ or another one? Adra-felin SJ 4042 Adravelin 1666 Worthenbury PR Radevellin 1673 Worthenbury PR Adrevelin 1674 Worthenbury PR Adafelin 1680 Worthenbury PR Adwefelin, Adrefelin 1683 Worthenbury PR Adavelin 1693 Worthenbury PR Adavelin 1700 Worthenbury PR Adavelen 1702 Worthenbury PR 4 Adruvellin 1703 Bangor Iscoed PR Adavelin 1712 Worthenbury PR Adwy’r Felin 1715 Worthenbury PR Adrefelin 1725 Worthenbury PR Adrefelin 1730 Worthenbury PR Adravelling 1779 Worthenbury PR Addravellyn 1780 Worthenbury PR Addrevelling 1792 Worthenbury PR Andravalyn 1840 O.S.Map.(Cassini) Aelwyd-uchaf SJ 0974 Aelwyd Ucha 1632 Tremeirchion PR Aylwyd Ucha 1633 Cwta Cyfarwydd, 147. -

10 Maes Y Wern, Gwernymynydd Offers Around
10 Maes Y Wern, Gwernymynydd Offers around • THREE BEDROOM SEMI DETACHED HOUSE • VILLAGE LOCATION • LOUNGE WITH FEATURE FIRE • HI GLOSS MODERN KITCHEN • CONSERVATORY • SHOWER ROOM • FRONT & REAR GARDENS • CLOSE TO LOGGERHEADS & 10 Maes Y Wern, Gwernymynydd * VILLAGE LOCATION * THREE BEDROOM SEMI DETACHED * GOOD SIZE PLOT * MODERN HI GLOSS KITCHEN * CONSERVATORY Reid & Roberts are delighted to offer For Sale this Well Presented Three Bedroom Semi Detached House in the sought after Village of Gwernymyndd which is a short distance from Loggerheads Country Park and Mold Town Centre. The property has a well kept front garden and a pathway leads to the front entrance door which leads into the Well Lit Lounge having a Feature Cast Iron Log Effect Fire a door leads into a good Kitchen with High Gloss Units and Integral applicances. The Conservatory leads out onto a Large Decking Area overlooking the Rear Garden. To the first floor you will find a Landing leading off to the Three Bedrooms and Shower Room. Outside you will find gardens to the front and rear which is larger than average and mainly laid to lawn, you will find an outside toilet to the rear of the property. 'Off Road' Parking can be found in the Car Park across the road from the property which is solely for residents of Maes y Wern. Gwernymynydd is a popular village community standing off the A494(T) Ruthin Road, some 2 miles from the county town of Mold. There is a popular primary schools and inn in the village whilst Mold provides a wide range of facilities catering for most daily requirements and is served with a regular bus service.