Using Osmolality to Diagnose and Treat Hyponatremia in Covid-19 Patients
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hyperosmolar Hyperglycemic State (HHS) Erica Kretchman DO October 19 2018 Speaker for Valeritas, Medtronic, Astrazenica, Boehringer Ingelheim
Hyperosmolar Hyperglycemic State (HHS) Erica Kretchman DO October 19 2018 Speaker for Valeritas, Medtronic, AstraZenica, Boehringer Ingelheim. These do not influence this presentation Objective • Review and understand diagnosis of Hyperosmolar Hyperglycemic State (HHS) and differentiating from Diabetic Ketoacidosis • Treatment of HHS • Complications of HHS Question 1 • Which of the following is NOT a typical finding in HHS? 1. Blood PH <7.30 2. Dehydration 3. Mental Status Changes 4. Osmotic diuresis Question 2 • Hypertonic fluids, such as 3% saline, are the first line of treatment to correct dehydration in HHS 1. True 2. False Question 3 • Which of the following statements is INCORRECT about Hyperosmolar Hyperglycemic State? 1. HHS occurs mainly in type 2 diabetics. 2. This condition presents without ketones in the urine. 3. Metabolic alkalosis presents in severe HHS. 4. Intravenous Regular insulin is used to treat hyperglycemia. Hyperosmolar Hyperglycemic State (HHS) • HHS and DKA are of two of the most serious complications form Diabetes • Hospital admissions for HHS are lower than the rate for DKA and accounts for less than 1 percent of all primary diabetic admissions • Mortality rate for patients with HHS is between 10 and 20 percent, which is approximately 10 times higher than that for DKA • Declined between 1980 and 2009 • Typically from precipitating illness - rare from HHS itself PRECIPITATING FACTORS • The most common events are infection (often pneumonia or urinary tract infection) and discontinuation of or inadequate insulin -

Effect on Ca++. the Clinical Significance of This Observation Re- Suggest That Physiologic Jaundice Results from a Markedly In- Quires Further Evaluation
ABSTRACTS 413 effect on Ca++. The clinical significance of this observation re- suggest that physiologic jaundice results from a markedly in- quires further evaluation. creased load of bilirubin presented to the liver either from increased bilirubin synthesis or enhanced intestinal reabsorb- Controlled clinical trial of phenobarbital (PB) and light for tion and marked limitation in the capacity to conjugate. management of neonatal hyperbilirubinemia in a predomi- Studies performed at 4 hours of age in a monky born 2 weeks nant Negro population. O. S. VALDES, H. M. MAURER, C. N. post-maturely revealed that hepatic transport and conjugation SHUMWAY, D. DRAPER, and A. HOSSAINI. Med. Coll. of Virginia, of bilirubin was fully mature, indicating that maturation of Richmond, Va. (Intr. by W. E. Laupus). each of these functions may occur in utero. Low birth weight infants, less than 24 hrs of age, were randomly assigned to receive either oral PB, 5 mg/kg/day for 5 A controlled study of intravenous fibrin hydrolysate supple- days, blue light (200-300 footcandles) continuously for 4 days, a ment in prematures <1.3 kg. M. HEATHER BRYAN, PATRICK combination of PB and light, or no treatment. 90% or more of WEI, RICHARD HAMILTON, SANFORD H. JACKSON, INGEBORC C. the infants in each group were Negroes. Infants with a positive RADDE, GRAHAM W. CHANCE, and PAUL R. SWYER. Univ. of Coomb's test were excluded. Toronto and The Research Inst., The Hosp. for Sick Children, Toronto, Ont. Canada. We have compared the effect of early supplemental intra- Total serum bilirubin concentration, mg% (mean ± S.E.) venous 3.5% fibrin hydrolysate plus 10% dextrose to 10% No. -

Severe Hyponatremia with Hypouricemia in a Patient with Medullary Hemorrhage: a Case Report
SUTIRTHA CHAKRABORTY, TAPAS K BANERJEE SEVERE HYPONATREMIA WITH HYPOURICEMIA IN A PATIENT WITH MEDULLARY HEMORRHAGE: A CASE REPORT The Journal of the International Federation of Clinical Chemistry and Laboratory Medicine SEVERE HYPONATREMIA WITH HYPOURICEMIA IN A PATIENT WITH MEDULLARY HEMORRHAGE: A CASE REPORT Sutirtha Chakraborty1, Tapas K Banerjee2 1Consultant & Chief, Dept. of Biochemistry, Peerless Hospital & B K Roy Research Centre, Kolkata 700094, India 2Sr. Consultant & Head, Dept. of Neurology, National Neurosciences Centre, Peerless Hospital, Kolkata,India Corresponding Author: Dr Sutirtha Chakraborty, MD Consultant & Chief, Dept. of Biochemistry Peerless Hospital & B K Roy Research Centre, Kolkata 700094 , India e‐mail: [email protected] Mobile +91 9874787638 ABSTRACT Hyponatremia is the commonest electrolyte abnormality in hospitalized patients and occurs due to various causes. Here we present a case of SIADH who was diagnosed using commonly available biochemical tests. This case report also discusses the interaction of the laboratory physician with the treating clinician and the approach needed to arrive at a correct diagnosis. It highlights the importance of serum uric acid and fractional excretion of urinary uric acid in the diagnosis of SIADH. It also discusses the approach needed to distinguish SIADH from Cerebral Salt wasting syndrome, where the presenting feature is also hyponatremia. KEY WORDS Hyponatremia, SIADH, Uric Acid. CASE REPORT A 68 year old gentleman was admitted to the Dept. of Neurology with a history of sudden onset uneasiness followed by slurring of speech and giddiness. Examination by the Consultant Neurologist showed that he was conscious and obeying commands with a Glasgow Coma Scale of 14/15.Power was grade 4/5 in all four limbs and DTRs preserved. -
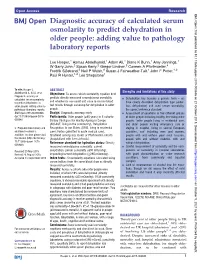
Diagnostic Accuracy of Calculated Serum Osmolarity to Predict Dehydration in Older People: Adding Value to Pathology Laboratory Reports
Open Access Research BMJ Open: first published as 10.1136/bmjopen-2015-008846 on 21 October 2015. Downloaded from Diagnostic accuracy of calculated serum osmolarity to predict dehydration in older people: adding value to pathology laboratory reports Lee Hooper,1 Asmaa Abdelhamid,1 Adam Ali,1 Diane K Bunn,1 Amy Jennings,1 W Garry John,2 Susan Kerry,2 Gregor Lindner,3 Carmen A Pfortmueller,4 Fredrik Sjöstrand,5 Neil P Walsh,6 Susan J Fairweather-Tait,1 John F Potter,1,2 Paul R Hunter,1,2 Lee Shepstone1 To cite: Hooper L, ABSTRACT et al Strengths and limitations of this study Abdelhamid A, Ali A, . Objectives: To assess which osmolarity equation best Diagnostic accuracy of predicts directly measured serum/plasma osmolality ▪ – calculated serum osmolarity Dehydration has become a generic term we and whether its use could add value to routine blood to predict dehydration in have clearly described dehydration type (water- older people: adding value to test results through screening for dehydration in older loss dehydration) and used serum osmolality, pathology laboratory reports. people. the correct reference standard. BMJ Open 2015;5:e008846. Design: Diagnostic accuracy study. ▪ Assessment of equations in five different groups doi:10.1136/bmjopen-2015- Participants: Older people (≥65 years) in 5 cohorts: of older people including healthy free-living older 008846 Dietary Strategies for Healthy Ageing in Europe people, frailer people living in residential care, (NU-AGE, living in the community), Dehydration and older people visiting emergency care or ▸ Prepublication history and Recognition In our Elders (DRIE, living in residential staying in hospital, living in several European additional material is care), Fortes (admitted to acute medical care), countries, and including men and women, available. -

Effects of Hyperglycemia and Rapid Lowering of Plasma Glucose in Normal Rabbits
MILESTONES IN NEPHROLOGY J Am Soc Nephrol 11: 1776–1788, 2000 Mark A. Knepper, Feature Editor Studies on Mechanisms of Cerebral Edema in Diabetic Comas EFFECTS OF HYPERGLYCEMIA AND RAPID LOWERING OF PLASMA GLUCOSE IN NORMAL RABBITS ALLEN I. ARIEFF AND CHARLES R. KLEEMAN WITH THE TECHNICAL ASSISTANCE OF ALICE KEUSHKERIAN AND HELEN BAGDOYAN From the Departments of Medicine, Wadsworth Veterans Administration Center and Cedars-Sinai Medical Center, and the Cedars-Sinai Medical Research Institute, and University of California Los Angeles Medical Center, Los Angeles, California 90048 with comments by ALLEN I. ARIEFF AND RICHARD STERNS Reprinted from J. Clin. Invest. 52:571–583, 1973 A BSTRACT To investigate the pathophysiology of cerebral edema occurring during treatment of diabetic coma, the effects of hyperglycemia and rapid lowering of plasma glucose were AUTHOR COMMENTARY evaluated in normal rabbits. During 2 h of hyperglycemia (plasma glucose = 61 mM), both brain (cerebral cortex) and Allen I. Arieff muscle initially lost about 10% of water content. After 4 h of hyperglycemia, skeletal muscle water content remained low University of California, but that of brain was normal. Brain osmolality (Osm) (343 San Francisco mosmol/kg H2O) was similar to that of cerebrospinal fluid Sausalito, California (CSF) (340 mosmol/kg), but increases in the concentration of Na+, K+, Cl–, glucose, sorbitol, lactate, urea, myoinositol, and amino acids accounted for only about half of this increase. n 1936, Dillon, Riggs, and Dyer described a syndrome The unidentified solute was designated “idiogenic osmoles”. Iwhereby individuals who were being treated for diabetic When plasma glucose was rapidly lowered to normal with coma and apparently recovering suddenly deteriorated, with insulin, there was gross brain edema, increases in brain content worsening of coma, respiratory insufficiency, hypotension, of water, Na+, K+, Cl– and idiogenic osmoles, and a signifi tachycardia, high fever, and death (1). -

Water Deprivation Test and Desmopressin Test in Adults
BLOOD SCIENCES DEPARTMENT OF CLINICAL BIOCHEMISTRY Title of Document: Water Deprivation Test in Adults Q Pulse Reference No: BS/CB/DCB/EN/16 Version NO: 5 Authoriser: Sadie Redding Page 1 of 4 WATER DEPRIVATION TEST Introduction Diabetes insipidus (DI) involves deficient production or lack of effective action of antidiuretic hormone (ADH or arginine vasopressin). ADH stimulates the kidney to conserve fluid. Deficient production of ADH or lack of effective action of ADH causes a high urine output, thirst, dehydration, and low blood pressure in advanced cases. Disease of the hypothalamus/pituitary gland leading to a deficiency in ADH production is called cranial or central DI. Disease of the kidney leading to lack of response of the kidney to fluid conserving action of ADH is called nephrogenic DI. The principle of the water deprivation test is to assess the ability of the patient to concentrate urine when fluids are withheld. Water deprivation should normally cause increased secretion of ADH, resulting in the production of small volumes of concentrated urine. Initial tests Polyuria should be confirmed by 24hour urine volume. Rule out diabetes, UTI, hypercalcaemia, hypokalaemia, renal failure and thyrotoxicosis. Morning urine osmolality >600mOsm/kg rules out DI and therefore a water deprivation test is not necessary. Preparation Please contact the Duty Biochemist at least 24 hours before the test (ext.48437) Normal dinner and fluids are allowed the night before the test. No alcohol or caffeine. 7am light breakfast but NO fluids, tea, coffee or smoking. Supervision is required throughout to assess compliance and safety. Contraindications Hypovolaemia or hypernatraemia Procedure Print out a worksheet and record results in the table (appendix 1). -

Hypertonic Saline Test for the Investigation of Posterior Pituitary
Arch Dis Child 1998;79:431–434 431 Hypertonic saline test for the investigation of Arch Dis Child: first published as 10.1136/adc.79.5.431 on 1 November 1998. Downloaded from posterior pituitary function Angelika Mohn, Carlo L Acerini, Timothy D Cheetham, StaVord L Lightman, David B Dunger Abstract (ADH) concentrations. The test is well estab- The hypertonic saline test is a useful tech- lished in adults56 yet there is little reported nique for distinguishing partial diabetes experience of its use in children. insipidus from psychogenic polydipsia, We describe five cases in which the hyper- and for the diagnosis of complex disorders tonic saline test provided a clear diagnosis of of osmoreceptor and posterior pituitary various disorders of water balance where function. However, there is little infor- standard diagnostic procedures had failed or mation concerning its use in childhood. were deemed unreliable. The experience of using this test in five children (11 months to 18 years) who pre- Methods and materials sented diagnostic problems is reported. In All the tests were performed at the John two patients, in whom water deprivation RadcliVe Hospital, Oxford and informed con- tests were equivocal or impractical, an sent was obtained from the patients and/or inappropriately low antidiuretic hormone their parents. Before testing, each patient was (ADH) concentration (< 1 pmol/l) was assessed to exclude the presence of any demonstrated in the presence of an ad- confounding factor such as hypercalcaemia, equate osmotic stimulus (plasma osmola- hypokalaemia, glycosuria or any other cause of lity > 295 mosmol/kg). In two children— a solute diuresis. -

Review of Serum Chemistry Interpretation in Neonatal Foals
APPLIED MEDICINE: CLINICAL PATHOLOGY AND DERMATOLOGY Review of Serum Chemistry Interpretation in Neonatal Foals Bryan M. Waldridge, DVM, MS, Dipomate ABVP (Equine Practice), Diplomate ACVIM Interpretation of serum chemistry results in foals can be very confusing because reference ranges are usually based on adult samples, and many values are increased in foals compared with adults. Un- derstanding the expected differences in serum chemistry results between foals and adult horses improves the recognition of abnormalities and facilitates making an accurate diagnosis. Author’s address: PO Box 1843, Georgetown, KY 40324; e-mail: [email protected]. © 2013 AAEP. 1. Introduction Serum alkaline phosphatase (ALP) activity is 2,3,6,7 Reference ranges for many serum chemistry values highest during the first 2 to 8 weeks of life and 7 6 in adult horses cannot reliably diagnose disease in remains elevated for 8 weeks to at least 90 days. foals.1–4 Placental abnormalities may influence There is a wide individual variation and large stan- dard deviation of ALP activity in foals, which limits clinicopathologic results in neonates during the first 2 1 its effectiveness to diagnose hepatobiliary disease. few days of life. Most hepatic indices in foals are 8 significantly different from adult horses, especially Hank et al measured activity of specific ALP during the neonatal period. Ideally, age-specific isoenzymes and determined that 80% to 92% of total ALP activity is from bone. However, Dumas and reference ranges should be used in foals, but it is 9 difficult to sample a large enough population of clin- Spano reported that increased ALP activity in foals ically normal foals and few laboratories are able to is mainly of hepatic origin. -

The Measurement of Serum Osmolality and Its Application to Clinical
Jornal Brasileiro de Patologia e Medicina Laboratorial ISSN: 1676-2444 [email protected] Sociedade Brasileira de Patologia Clínica/Medicina Laboratorial Brasil Faria, Daniel K.; Mendes, Maria Elizabete; Sumita, Nairo M. The measurement of serum osmolality and its application to clinical practice and laboratory: literature review Jornal Brasileiro de Patologia e Medicina Laboratorial, vol. 53, núm. 1, febrero, 2017, pp. 38-45 Sociedade Brasileira de Patologia Clínica/Medicina Laboratorial Rio de Janeiro, Brasil Available in: http://www.redalyc.org/articulo.oa?id=393549993007 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative REVIEW ARTICLE J Bras Patol Med Lab, v. 53, n. 1, p. 38-45, February 2017 The measurement of serum osmolality and its application to clinical practice and laboratory: literature review 10.5935/1676-2444.20170008 A medida da osmolalidade sérica e sua aplicação na prática clínica e laboratorial: revisão da literatura Daniel K. Faria; Maria Elizabete Mendes; Nairo M. Sumita Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (FMUSP), São Paulo, Brazil. ABSTRACT Introduction: Serum osmolality is an essential laboratory parameter to understand several clinical disorders such as electrolyte disturbances, exogenous intoxication and hydration status. Objective: This study aims to update knowledge about the osmolality examination through research papers published to date. Materials and methods: The survey was conducted on PubMed database. It highlights main concepts, both historical and physiological aspects, and the clinical applications of the serum osmolality test. -
Hyponatraemia- Principles, Investigation and Management
Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents • Background • Investigation • Classification • Normal Osmolality • General management and SIADH • Cases Background • Relatively common: - Estimated 15-30% prevalence in all acute admissions - Prevalence 2.48% in community with 0.97% incidence in 1985 • Associated with gait disturbance, cognitive disturbance, osteoporosis and mortality - (Not causative) Background • Hyponatraemia: Serum sodium of less than 135mmol/L - Mild: 130-135 - Moderate:125-129 - Severe: <125 • Acute is <48 hours, Chronic is >48 hours. • Reflects serum osmolality • Hyponatraemia causes cell overhydration Background adaptation Pseudo Background hyponatraemia Lipid Pseudo True hyponatraemia hyponatraemia Normal 1L /1Kg Na 1L Na 1Kg Na 1L /1Kg Na 135 125 135 125 Osm/Kg-280 Osm/Kg-280 Osm/Kg-265 Background Background - Symptoms • Mild: - Asymptomatic - Headache, anorexia, nausea, lethargy • Moderate: - Confusion, muscle cramps, weakness, confusion, ataxia • Severe: - Drowsiness, coma, vomiting, brainstem herniation, seizures • Rapid correction: - Cerebral pontine demyelinolysis Assessment Examination Investigations • Capillary refill • U+Es • Tissue turgor • LFTs • Radial pulse- ?tachycardia • Osmolality (paired serum and urine) • Mucous membranes • Urine Sodium and Potassium • JVP • Thyroid function Tests • Heart sound- ?flow murmurs • 9am Cortisol ?S3 • CXR • Breath sounds- ?crepitations • CT Head (?SIADH) • Ascites • Peripheral oedema If required: • Lipid profile • Protein -

Diabetic Ketoacidosis (DKA) Author: Leigh Vaughn
Diabetic Ketoacidosis (DKA) Author: Leigh Vaughn DKA definition: Elevated glucose, presence of ketones, metabolic acidosis (triad) + dehydration, with absolute or relative insulin deficiency increase counter regulator hormones breakdown of fat and muscle. Not a hyperosmolar state like Hyperglycemic Hyperosmolar State (HHS). Epidemiology: • Most common at onset Type 1 DM, recurrent episodes common • Can occur in Type 2 DM. More often affects young • Death can be related to cerebral edema or the precipitating trigger/illness for the DKA. • Mortality < 1%, significantly lower than mortality of HHS Triggers (The “I’s”): • Initial (new onset) disease • Insulin omission (adherence, access, absorption) • Infection • Ischemia (ACS, stroke) • Intra-abdominal (pancreatitis, cholecystitis, ischemic bowel, pregnancy) • Ingestions (ETOH, substance abuse, meds-steroids, antipsychotics, thiazides, pentamidine), Pathophysiology: • 3 causes of increased glucose: Gluconeogenesis, Glycogenolysis, Impaired glucose utilization • Increase glucose + deficiency of insulin + stress (trigger) increases the secretion of glucagon, catecholamines, cortisol, and growth hormone (counter-regulatory hormones) promotion of lipolysis increases FFA delivery to the liver FFA converted by free fatty acyl CoA into ketones Clinical presentation: • Develops over hours to days; not days to weeks, like HHS. • Polyuria, Polydipsia, Polyphagia, Fatigue, Muscle cramps (from Acidosis), Flushed facial appearance, Kussmaul’s respirations and dyspnea (from acidosis) Nausea and -

Evaluation of Hyponatremia: a Little Physiology Goes a Long Way
REVIEW BENJAMIN J. FREDA, DO MICHAEL B. DAVIDSON, DO PHILLIP M. HALL, MD Department of Nephrology and Hypertension, Department of Internal Medicine, The Cleveland Staff Consultant, Department of Nephrology and The Cleveland Clinic Foundation Clinic Foundation Hypertension, The Cleveland Clinic Foundation Evaluation of hyponatremia: A little physiology goes a long way ■ ABSTRACT YPONATREMIA (a low plasma sodium con- H centration) is among the most common Hyponatremia is common in hospitalized patients. By laboratory abnormalities that physicians taking a careful and logical approach, one can promptly encounter, yet its causes are among the more recognize the causative factor or factors in nearly all complex in medicine. cases. Most cases of hyponatremia are due to impaired In a study of more than 2,800 hospitalized renal water excretion, and recognizing the cause and patients, 15% had plasma sodium concentra- pathophysiologic process makes it possible to provide tions below the lower end of the reference focused individualized care and avoid mistreatment. range of 134 mmol/L.1 Almost 5% had levels less than 125 mmol/L. ■ KEY POINTS In some instances, hyponatremia repre- sents a true medical emergency, requiring In evaluating hyponatremia, the clinician should immediate intervention to prevent cerebral determine the chronicity or acuity of the hyponatremia, edema. More commonly, hyponatremia may confirm that the patient has true plasma hypo-osmolality, reflect the severity of a causative underlying determine the extracellular fluid volume status, assess illness and be a marker of morbidity and mor- laboratory tests and urine sodium values, and assess any tality. For example, the plasma sodium con- centration is a powerful predictor of severity of exogenous free water intake.