Medieval Globe
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
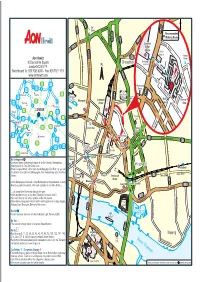
Aon Hewitt-10 Devonshire Square-London EC2M Col
A501 B101 Old C eet u Street Str r t A1202 A10 ld a O S i n Recommended h o A10 R r Walking Route e o d et G a tre i r d ld S e t A1209 M O a c Liverpool iddle t h sex Ea S H d Street A5201 st a tre e i o A501 g e rn R Station t h n S ee Police tr S Gr Station B e e t nal Strype u t Beth B134 Aon Hewitt C n Street i t h C y Bishopsgate e i l i t N 10 Devonshire Square l t Shoreditch R a e P y East Exit w R N L o iv t Shoreditcher g S St o Ra p s t London EC2M 4YP S oo re pe w d l o e y C S p t tr h S a tr o i A1202 e t g Switchboard Tel: 020 7086 8000 - Fax: 020 7621 1511 d i e h M y t s H i D i R d www.aonhewitt.com B134 ev h B d o on c s Main l a h e t i i r d e R Courtyard s J21 d ow e e x A10 r W Courtyard M11 S J23 B100 o Wormwood Devonshire Sq t Chis h e r M25 J25 we C c e l S J27 l Str Street a e M1 eet o l t Old m P Watford Barnet A12 Spitalfields m A10 M25 Barbican e B A10 Market w r r o c C i Main r Centre Liverpool c a r Harrow Pl A406 J28 Moorgate i m a k a e t o M40 J4 t ld S m Gates C Harrow hfie l H Gate Street rus L i u a B le t a H l J1 g S e J16 r o J1 Romford n t r o e r u S e n tr A40 LONDON o e d e M25 t s e Slough M t A13 S d t it r c A1211 e Toynbee h J15 A13 e M4 J1 t Hall Be J30 y v Heathrow Lond ar is on W M M P all e xe Staines A316 A205 A2 Dartford t t a London Wall a Aldgate S A r g k J1 J2 s East s J12 Kingston t p Gr S o St M3 esh h h J3 am d s Houndsditch ig Croydon Str a i l H eet o B e e A13 r x p t Commercial Road M25 M20 a ee C A13 B A P h r A3 c St a A23 n t y W m L S r n J10 C edldle a e B134 M20 Bank of e a h o J9 M26 J3 heap adn Aldgate a m sid re The Br n J5 e England Th M a n S t Gherkin A10 t S S A3 Leatherhead J7 M25 A21 r t e t r e e DLR Mansion S Cornhill Leadenhall S M e t treet t House h R By Underground in M c o Bank S r o a a Liverpool Street underground station is on the Central, Metropolitan, u t r n r d DLR h i e e s Whitechapel c Hammersmith & City and Circle Lines. -

861 Sq Ft Headquarters Office Building Your Own Front Door
861 SQ FT HEADQUARTERS OFFICE BUILDING YOUR OWN FRONT DOOR This quite unique property forms part of the building known as Rotherwick House. The Curve comprises a self-contained building, part of which is Grade II Listed, which has been comprehensively refurbished to provide bright contemporary Grade A office space. The property — located immediately to the east of St Katharine’s Dock and adjoining Thomas More Square — benefits from the immediate area which boasts a wide variety of retail and restaurant facilities. SPECIFICATION • Self-contained building • Generous floor to ceiling heights • New fashionable refurbishment • Full-height windows • New air conditioning • Two entrances • Floor boxes • Grade II Listed building • LG7 lighting with indirect LED up-lighting • Fire and security system G R E A ET T THE TEA TRE E D S A BUILDING OL S T E R SHOREDITCH N S HOUSE OLD STREET T R E E T BOX PARK AD L RO NWEL SHOREDITCH CLERKE C I HIGH STREET T Y R G O O A S D W S F H A O E R L U A L R T AD T H I O R T R N A S STEPNEY D’ O O M AL G B N A GREEN P O D E D T H G O T O WHITECHAPEL A N N R R R O D BARBICAN W O CHANCERY E A FARRINGDON T N O LANE D T T E N H A E M C T N O C LBOR A D O HO M A IGH MOORGATE G B O H S R R U TOTTENHAM M L R LIVERPOOL P IC PE T LO E COURT ROAD NDON WA O K A LL R N R H STREET H C L C E E O S A I SPITALFIELDS I IT A A W B N H D L E W STE S R PNEY WAY T O J R U SALESFORCE A E HOLBORN B T D REE TOWER E ST N I D L XFOR E G T O W R E K G ES H ALDGATE I A H E N TE A O M LONDON MET. -
![Download/Chb/MESBD/MESBD.Zip [Last Accessed August 4, 2011]](https://docslib.b-cdn.net/cover/8841/download-chb-mesbd-mesbd-zip-last-accessed-august-4-2011-608841.webp)
Download/Chb/MESBD/MESBD.Zip [Last Accessed August 4, 2011]
Durham Research Online Deposited in DRO: 10 March 2015 Version of attached le: Accepted Version Peer-review status of attached le: Peer-reviewed Citation for published item: Kendall, E. and Montgomery, J. and Evans, J. and Stantis, C. and Mueller, V. (2013) 'Mobility, mortality, and the middle ages : identication of migrant individuals in a 14th century black death cemetery population.', American journal of physical anthropology., 150 (2). pp. 210-222. Further information on publisher's website: http://dx.doi.org/10.1002/ajpa.22194 Publisher's copyright statement: This is the accepted version of the following article: Kendall, E.J., Montgomery, J., Evans, J.A., Stantis, C. and Mueller, V. (2013), Mobility, mortality, and the middle ages: Identication of migrant individuals in a 14th century black death cemetery population. American Journal of Physical Anthropology, 150 (2): 210-222, which has been published in nal form at http://dx.doi.org/10.1002/ajpa.22194. This article may be used for non-commercial purposes in accordance With Wiley Terms and Conditions for self-archiving. Additional information: Use policy The full-text may be used and/or reproduced, and given to third parties in any format or medium, without prior permission or charge, for personal research or study, educational, or not-for-prot purposes provided that: • a full bibliographic reference is made to the original source • a link is made to the metadata record in DRO • the full-text is not changed in any way The full-text must not be sold in any format or medium without the formal permission of the copyright holders. -
RDP SPEC GUIDE 09.Pdf
Flora London Marathon 2009 Pace Chart Mile Elite Wheel Wheel Elite 3:30 4:30 5:00 6:00 Women chair chair Men/ Pace Pace Pace Pace Spectator Men Women Mass Start 09:00 09:20 09:20 09:45 09:45 09:45 09:45 09:45 1 09:05 09:23 09:24 09:49 09:53 09:55 09:56 09:58 Guide 2 09:10 09:27 09:28 09:54 10:01 10:05 10:07 10:12 Flora London Marathon spectators are a crowd on the move! Most people like to try 3 09:15 09:31 09:32 09:59 10:09 10:15 10:19 10:26 and see runners at more than one location on the route and it’s great to soak up the 4 09:21 09:34 09:36 10:04 10:17 10:26 10:30 10:40 atmosphere, take in some of the landmarks, and perhaps pick up refreshments on 5 09:26 09:38 09:41 10:09 10:25 10:36 10:42 10:53 the way too. Here are some tips on getting around London to make your day safer 6 09:31 09:42 09:45 10:13 10:33 10:46 10:53 11:07 and more enjoyable. 7 09:36 09:45 09:49 10:18 10:41 10:57 11:05 11:21 8 09:42 09:49 09:53 10:23 10:49 11:07 11:16 11:35 here are hundreds of thousands of people lining On the opposite page is a specially formulated pace guide to 9 09:47 09:53 09:57 10:28 10:57 11:17 11:28 11:48 the route of the Flora London Marathon every year, help you follow the top flight action in the elite races. -

Children's Holiday Clubs & Sports Camps Tower Hamlets
Children's Holiday Clubs & Sports Camps Tower Hamlets Children's Easter, Summer, Christmas holiday camps and February, May, October half term clubs around Tower Hamlets, multi sport & activities, learning, workshops, courses, sports camps, water sports, parkour, kayaking, dance, art, IT, football, tennis, performing arts, swimming, sailing and many other options, also over half terms and school breaks for kids in Tower Hamlets, Whitechapel, Wapping, Millwall, Mile End, Stepney, Bethnal Green, Canary Wharf, Blackwall, Bow, Bromley-by-Bow, Cambridge Heath, Docklands, East Smithfield, Fish Island, Globe Town, Isle of Dogs, Cubitt Town, Leamouth, Limehouse, Old Ford, Poplar, Ratcliff, St George in the East, Shadwell, Spitalfields, Wapping areas. SEE Link for RESIDENTIAL camps, SUMMER Schools, Children's Activities ALSO VIRTUAL CAMPS & ACTIVITIES - https://www.020.co.uk/v/virtual-camps-and-activities/london.shtml The Strings ClubFeatured OPEN. Multi award-winning, Ofsted registered holiday camp at Halley House, E8 2DJ and Gainsborough Primary School E9 5ND - offering only the very best in childcare and music for children aged 4 - 11. Childcare vouchers accepted. Don't miss out! Nr Tower Hamlets E8 and E9 07931 037 186 Queen Mary University Students Union Sports holiday camps for 8 to 13 yo in Tower Hamlets offering the opportunity to participate in fun activities during the school holidays whilst learning new skills which include football, cricket, basketball, badminton, short tennis and more. Mile End Road Campus E1 4DH 020 7882 5765 Museum of London Docklands Museum of London Docklands' free virtual activities are wild & wonderful from the live stream family rave to reggae week, short talks, unguided secret tours, London audio walks, history & exhibition tours on YouTube channel & Facebook. -
Preferred Office Location Boundary Review (2017)
London Borough of Tower Hamlets Preferred Office Locations Boundary review Peter Brett Associates Final July 2017 Office Address: 16 Brewhouse Yard, Clerkenwell, London EC1V 4LJ T: +44 (0)207 566 8600 E: [email protected] Project Ref 40408 Name Position Signature Date Prepared by Andrew Lynch Associate AL 19th May ‘17 Reviewed by Richard Pestell Director RP 23rd May ‘17 Approved by Richard Pestell Director RP 24th July ‘17 For and on behalf of Peter Brett Associates LLP Revision Date Description Prepared Reviewed Approved 23rd May 1 draft AL RP RP ‘17 24th July 2 Final AL RP RP ‘17 Peter Brett Associates LLP disclaims any responsibility to the client and others in respect of any matters outside the scope of this report. This report has been prepared with reasonable skill, care and diligence within the terms of the contract with the client and taking account of the manpower, resources, investigations and testing devoted to it by agreement with the client. This report has been prepared for the client and Peter Brett Associates LLP accepts no responsibility of whatsoever nature to third parties to whom this report or any part thereof is made known. Any such party relies upon the report at their own risk. © Peter Brett Associates LLP 2017 THIS REPORT IS FORMATTED FOR DOUBLE-SIDED PRINTING. ii London Borough of Tower Hamlets - Preferred Office Locations Boundary review CONTENTS 1 INTRODUCTION .......................................................................................................... 1 2 OVERVIEW OF THE BOROUGH-WIDE OFFICE FLOORSPACE DEMAND SUPPLY BALANCE ............................................................................................................................. 4 3 METHOD FOR BOUNDARY ASSESSMENTS ............................................................ 6 4 NORTH OF THE ISLE OF DOGS (CANARY WHARF) - BOUNDARY ASSESSMENT 7 The potential for intensification .................................................................................... -

Post Office London Pub
1822 PUB POST OFFICE LONDON PUB PUBLICANS-continued. Lord Napier, Frederick Rix, 27 London fields, Mansion House, Percy IIamilton Gardner, 204 Metropolitan Tavern,Da.niel William Vousden-, Laurie Arms,Robert Tuck,1 Should ham street, Hackney NE Evelyn street, Deptford SE 95 Farringdon road E C &; Bryanston square W 32 Crawford place, - George IIenryStribling, 118 Great Church - John Mather Presley, 46 & 48 Kennington Tavern, Waiter Orchard1 79 West Edgware road W lane, llammersmith W park road S E bourne road N Leather Exchange Tavern, Mrs.Alois Pfeiffer, Lord Nelson, Mrs. Anne Elizabeth Da.vey, 1 Marion Arms, George Robert Jackson, 46 Middleton Arms, Frederick Longhurst, 14 Leather market, Bermondsey SE Manchester road, Poplar E Lansdowne road, Dalston NE Mansfield street, Kingsland road N E Lee Arms, Thomas William Savage, 27 Marl - William Hunter Gillingham, 17 Nelson Market House, Glaze Bros. Ltd. 9 Russell - William Joseph Young, 123 Queen's rood, borough road, Dalston N E street, City road E G street, Covent garden WC Dalston NE Leicester (The),Best's Brewery Co. Ltd.1 New - Charles Mackie Hurt, 18 Upper Charlton Market House Tavern, Ernest Hellard, Col Mildmay Park Tavern, James Palmer, 130 0oYPntry street W street, Fitzroy ~quare W umbia market, Columbia road E Ball's Pond road N Leigh Hoy, Jsph. Perkoff, 163 Hanbury st E - James Edwd. Marley, 386 Old Kent rd SE - Siduey Geo.Skepelhorn, 7 Finsbury mkt E C Milford Haven, John Wakely, 214 Cale Leighton Arms, Mrs. Ada Arnsby, 101 Breck - Albert Joseph Milton, 137 Trafalgar street, Market tavern, Ernest Percival Gladwin, 65 donian road N nock road N Walworth SE Brushfield street E Millwall Dock Hotel, Mrs. -

East Smithfield Wapping West
Docklands Sales, 3-5 Dock Street, London E1 8JN T 020 7480 0170 E [email protected] W www.ludlowthompson.com EAST SMITHFIELD WAPPING WEST SOLD REF: 1351344 2 Bed, Purpose Built Apartment, Private Balcony Two Balconies - Circa 1000 sq ft - Excellent Transport Links - Two Bedroom Apartment - Top Floor Apartment - Share of Freehold A stunning two bedroom apartment of approx 1000 sq ft on the top floor of this modern development in Tower Hill. The property has been finished to exacting standards throughout, with high specification fittings after the current owners completely renovated the property. Accommodation comprises of; a bright and spacious reception room with open plan kitchen, two double bedrooms, both with en suite bathrooms, as well as two private balconies with views of the City Skyline. Situated within a secur... continued below Train/Tube - Tower Gateway, Tower Hill, Aldgate, Aldgate East Local Authority/Council Tax - Tenure - Share of Freehold Docklands Sales, 3-5 Dock Street, London E1 8JN T 020 7480 0170 E [email protected] W www.ludlowthompson.com EAST SMITHFIELD WAPPING WEST Reception Room Kitchen Bedroom 1 Bedroom 2 Bathroom 1 Bathroom 2 Docklands Sales, 3-5 Dock Street, London E1 8JN T 020 7480 0170 E [email protected] W www.ludlowthompson.com EAST SMITHFIELD WAPPING WEST Overview Main Balcony Balcony, View 2 Exterior Docklands Sales, 3-5 Dock Street, London E1 8JN T 020 7480 0170 E [email protected] W www.ludlowthompson.com EAST SMITHFIELD WAPPING WEST Please note that this floor plan is produced for illustration and identification purposes only. It is NOT drawn to a scale. -

Property Details
EASTSMITHFIELD, LONDON, E1W THE A830 sq/ft two bed next to St. Katherine Docks PARTICULARS The Property Anoutstanding two double bedroom, two bathroom on East Smithfield, London, E1W thefourth floor of this well run block next to St. KatharineDocks. The apartment is well appointed and theaccommodation includes an open plan kitchen receptionroom, a principle bedroom with en-suite, a principlebathroom and a good sized second bedroom. Thereis a south facing Juliet balcony and the property Asking Price £530,000 hasthe added benefit of being offered for sale Leasehold chain-free. Location 2 Bedrooms Theproperty is situated on the fringes of City of 2 Bathrooms London,Wapping and Tower Hill and is virtually 1 Reception adjacentto the world famous 'Monte Carlo-style' surroundsof St Katharine Docks. There are fantastic Features localtransport links, which are all easily accessible with TowerHill, Tower Gateway, Aldgate, Aldgate East and 2Bedrooms, Juliet Balcony, 830 Sq/Ft, Wappingstations all being located within just minutes Lift,St Kathrine Docks, Lease Length- 125 ofthe apartment. Historic St Katharine Docks, Waitrose YearsFrom June 2002, Service Charge- supermarketin addition to a fine array of charming £4064Pa, Ground Rent- £250 Pa, Chain pubsand contemporary style restaurants and coffee Free,Ews1 - Passed housesboth on Wapping High Street and St Katharine Docksitself are also literally on the doorstep. A short strollup the nearby Thames-side promenade takes you toTower Bridge and across to Shad Thames and Bermondsey. Hamptons 41 Shad Thames Tower Bridge, London, SE1 2NJ 020 7407 3173 [email protected] www.hamptons.co.uk ForClarification Wewish to inform prospective purchasers that we have prepared these sales cupboards/shelves,etc. -
Buses from Shadwell from Buses
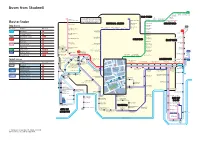
Buses from Shadwell 339 Cathall Leytonstone High Road Road Grove Green Road Leytonstone OLD FORD Stratford The yellow tinted area includes every East Village 135 Old Street D3 Hackney Queen Elizabeth Moorfields Eye Hospital bus stop up to about one-and-a-half London Chest Hospital Fish Island Wick Olympic Park Stratford City Bus Station miles from Shadwell. Main stops are for Stratford shown in the white area outside. Route finder Old Ford Road Tredegar Road Old Street BETHNAL GREEN Peel Grove STRATFORD Day buses Roman Road Old Ford Road Ford Road N15 Bethnal Green Road Bethnal Green Road York Hall continues to Bus route Towards Bus stops Great Eastern Street Pollard Row Wilmot Street Bethnal Green Roman Road Romford Ravey Street Grove Road Vallance Road 115 15 Blackwall _ Weavers Fields Grove Road East Ham St Barnabas Church White Horse Great Eastern Street Trafalgar Square ^ Curtain Road Grove Road Arbery Road 100 Elephant & Castle [ c Vallance Road East Ham Fakruddin Street Grove Road Newham Town Hall Shoreditch High Street Lichfield Road 115 Aldgate ^ MILE END EAST HAM East Ham _ Mile End Bishopsgate Upton Park Primrose Street Vallance Road Mile End Road Boleyn 135 Crossharbour _ Old Montague Street Regents Canal Liverpool Street Harford Street Old Street ^ Wormwood Street Liverpool Street Bishopsgate Ernest Street Plaistow Greengate 339 Leytonstone ] ` a Royal London Hospital Harford Street Bishopsgate for Whitechapel Dongola Road N551 Camomile Street 115 Aldgate East Bethnal Green Z [ d Dukes Place continues to D3 Whitechapel Canning -

Archaeological Investigations at 103—106 Shoreditch High Street, Hackney
ARCHAEOLOGICAL INVESTIGATIONS AT 103—106 SHOREDITCH HIGH STREET, HACKNEY Peter Boyer With contributions by Lucy Allott, Philip Armitage, Märit Gaimster, Kevin Hayward, Chris Jarrett and Kevin Rielly SUMMARY eastern side of Shoreditch High Street in the London Borough of Hackney (Fig 1). During 2008 and 2009 archaeological investigations It was bounded to the south by the Crown were undertaken at 103—106 Shoreditch High Street. Plaza Hotel and to the north and east by The earliest material discovered on site consisted of a commercial and residential properties. The scatter of residual Roman finds. However, the earliest Ordnance Survey National Grid Reference datable activity was medieval and comprised the for the centre of the site is TQ 3346 8253 and establishment of boundary ditches and the excavation the surface elevation lay at approximately of quarry pits along the eastern side of the High Street 16.5m OD. on the edge of the village of Shoreditch. During the An archaeological desk-based assessment 16th and 17th centuries the site was partly used as produced in advance of redevelopment a rubbish dump; faunal material recovered from these (Gailey 2007) indicated that the site, which lay deposits included evidence of both animal carcass within an Archaeology Priority Zone (APZ), processing and relatively high status dining, while the had a potential for the survival of Roman and associated finds included a piece of carved stag-horn medieval remains, despite extensive basement inlay. Over time the amount of activity on site steadily truncation within the western portion of the increased, reflecting the transformation of Shoreditch site. -
East Smithfield Wapping West
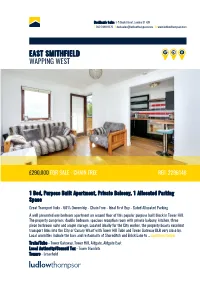
Docklands Sales, 3-5 Dock Street, London E1 8JN T 020 7480 0170 E [email protected] W www.ludlowthompson.com EAST SMITHFIELD WAPPING WEST £290,000 FOR SALE - CHAIN FREE REF: 2296148 1 Bed, Purpose Built Apartment, Private Balcony, 1 Allocated Parking Space Great Transport links - 60% Ownership - Chain Free - Ideal First Buy - Gated Allocated Parking A well presented one bedroom apartment on second floor of this popular purpose built block in Tower Hill. The property comprises; double bedroom, spacious reception room with private balcony, kitchen, three piece bathroom suite and ample storage. Located ideally for the City worker, the property boasts excellent transport links into the City or Canary Wharf with Tower Hill Tube and Tower Gateway DLR very close by. Local amenities include the bars and restaurants of Shoreditch and Brick Lane to ... continued below Train/Tube - Tower Gateway, Tower Hill, Aldgate, Aldgate East Local Authority/Council Tax - Tower Hamlets Tenure - Leasehold Docklands Sales, 3-5 Dock Street, London E1 8JN T 020 7480 0170 E [email protected] W www.ludlowthompson.com EAST SMITHFIELD WAPPING WEST Kitchen Bedroom Reception Room Bedroom Alt Living Room Alt Exterior Docklands Sales, 3-5 Dock Street, London E1 8JN T 020 7480 0170 E [email protected] W www.ludlowthompson.com EAST SMITHFIELD WAPPING WEST Balcony View Docklands Sales, 3-5 Dock Street, London E1 8JN T 020 7480 0170 E [email protected] W www.ludlowthompson.com EAST SMITHFIELD WAPPING WEST Please note that this floor plan is produced for illustration and identification purposes only. It is NOT drawn to a scale.