SUMANDEEP VIDYAPEETH (Declared As Deemed to Be University U/S 3Of UGC Act 1956) (Accredited by NAAC 'A' Grade with 3.53 CGPA Scale)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

University Aishe Code
University Aishe Code Aishe Srno Code University Name 1 U-0122 Ahmedabad University (Id: U-0122) 2 U-0830 ANANT NATIONAL UNIVERSITY (Id: U-0830) 3 U-0125 Carlox Teachers University, Ahmedabad (Id: U-0125) Centre for Environmental Planning and Technology University, Ahmedabad (Id: U- 4 U-0127 0127) 5 U-0131 Dr. Babasaheb Ambedkar Open University, Ahmedabad (Id: U-0131) 6 U-0775 GLS UNIVERSITY (Id: U-0775) 7 U-0135 Gujarat Technological University, Ahmedbabd (Id: U-0135) 8 U-0136 Gujarat University, Ahmedabad (Id: U-0136) 9 U-0817 GUJARAT UNIVERSITY OF TRANSPLANTATION SCIENCES (Id: U-0817) 10 U-0137 Gujarat Vidyapith, Ahmedabad (Id: U-0137) 11 U-0139 Indian Institute of Technology, Gandhinagar (Id: U-0139) 12 U-0922 Indrashil University (Id: U-0922) INSTITUTE OF INFRASTRUCTURE TECHNOLOGY RESEARCH AND MANAGEMENT 13 U-0765 (IITRAM) (Id: U-0765) 14 U-0734 LAKULISH YOGA UNIVERSITY, AHMEDABAD (Id: U-0734) 15 U-0146 Nirma University, Ahmedabad (Id: U-0146) 16 U-0790 RAI UNIVERSITY (Id: U-0790) 17 U-0595 Rakshashakti University, Gujarat (Id: U-0595) 18 U-0123 Anand Agricultural University, Anand (Id: U-0123) 19 U-0128 Charotar University of Science & Technology, Anand (Id: U-0128) 20 U-0148 Sardar Patel University, Vallabh Vidyanagar (Id: U-0148) 21 U-0150 Sardarkrushinagar Dantiwada Agricultural University, Banaskantha (Id: U-0150) 22 U-0124 Maharaja Krishnakumarsinhji Bhavnagar University (Id: U-0124) 23 U-0126 Central Univeristy of Gujarat, Gandhinagar (Id: U-0126) 24 U-0594 Children University, Gandhinagar (Id: U-0594) Dhirubhai Ambani Institute -

Name of Regional Directorate of NSS- Ahmedabad State-Gujarat
Name of Regional Directorate of NSS- Ahmedabad State-Gujarat Regional Director Name Address Email ID Telephone/Mobile/Landline Number Sh. GirdharUpadhyay Regional Directorate of NSS, [email protected] 079-26565988 2ndfloor,PatnagarYojnaBhavan, 7999894816 Ellis bridge ,Ahmedabad-380006 Secretary, dealing with NSS Name Address E Mail ID Telephone/Mobile Number Shri S.J. Haider , IAS Block No.-5, [email protected] 079-23251301/303 Principle Secretary 7th,Floor Fax 07923251325 Education Department Sachivalaya, Government of Gujarat Gandhinagar,Gujarat State NSS Officer/Officer acting as SNO Name Address E Mail ID Telephone/Mobile Number ShriYashwant Kumar HPatel Commissionerate of Higher Education [email protected] 9427685870 State NSS Officer Govt. of Gujarat, Old Sachivalaya 079-23253993 Block No.12/2,Dr. Jivraj Mehta Bhavan, Gandhinagar ,Gujarat Programme Coordinator, NSS Name Address E Mail ID Telephone/Mobile Number 1 Dr Shreedhar Nimavat Veer Narmad South Gujarat [email protected], 0261-2203039 Programme co-ordinator, NSS University, [email protected] 8780077566 Veer Narmad South Gujarat University Campus, University, Surat UdhnaMagdalla Road, Surat-395007 2 Dr. J. D. Damor Hemchandracharya [email protected] 02766-230743,Ext.316 Hemchandrcharya North North Gujarat University, 9925046204, 7573010065 Gujarat University, Patan Raj Mahal Road, P.B. No. 21 Patan-384265 3 Dr. N. K. Dobariya Saurashtra University, [email protected] 02812578501 Saurashtra University, Rajkot Kalavad Road, 9687692940 Rajkot-360 005 4 Dr. JagrutiSuvera Sardar Patel University, [email protected] 02692-226823 Sardar Patel University, VallabhVidyanagar, [email protected] 9408507810 VallabhVidyanagar,Anand Dist : Anand- 388120 5 Dr. Arunbhai Gandhi, Gujarat Vidyapith, [email protected] 079-4001630 Gujarat Vidyapeeth, Ashram Road, 9428214260 Ahmedabad Ahmedabad-380014 6 Dr. -

Renaissance (Vol 8- Issue 2 Sep 19) -Parcon Special Edition
RENAISSANCE PARCON 2019 Special Edition For National Conference on "Physiotherapy and Rehabilitation: Evidences leading to New Horizons" September 2019 Hosted by: College of Physiotherapy Sumandeep Vidyapeeth (Declared as an Institution Deemed to be University u/s 3 of the UGC act, 1956) NAAC 'A' Grade, 3.53 CGPA & Conferred with UGC-CATEGORY-1 status Piparia, Waghodia (Tk.), Vadodara – 391760 Telephone: +91 2668 245029 Email: [email protected] Conference Supported by: Gujarat Council on Science and Technology (GUJCOST) Department of Science and Technology, Government of Gujarat : Supported By : The conference is organized with the financial support of Gujarat Council on Science and Technology, Department of Science and Technology, Government of Gujarat Block: B, 7th Floor, M.S Building, Nr. Pathikashram, Sector-11, Gandhinagar, Gujarat. : Academic Partner : National Journal of Integrated Research in Medicine MESSAGES Dr. Mansukh. K. Shah Founder President Sumandeep Vidyapeeth Trust Message I am immensely pleased to know that The College of Physiotherapy has organized a National Conference on Physiotherapy and Rehabilitation on 20th and 21st September, which is being graced by Nationally reputed faculty from all over India. The College of Physiotherapy since its inception in 2001, was one of the founding pillars of Sumandeep Vidyapeeth which got notified in 2007. Since then the College has kept astride with the development and progress of Sumandeep Vidyapeeth specially in the fields of Academics, Research and optimal patient care. This is thanks to the sincere and dedicated faculty in the college, supportive staff and academically oriented students. The National Conference will provide a great opportunity to all faculty and delegates to explore new horizons in Physiotherapy and Rehabilitation. -

Consolidated List of All Universities
UNIVERSITY GRANTS COMMISSION Total No. of Universities in the Country as on 01.02.2020 Universities Total No. State Universities 409 Deemed to be Universities 127 Central Universities 50 Private Universities 349 Total 935 1 S.No ANDHRA PRADESH Date/Year of Notification/ Establishment 1. Acharya Nagarjuna University, Nagarjuna Nagar-522510, Dt. Guntur, 1976 Andhra Pradesh. (State University) 2. Adikavi Nannaya University, 25-7-9/1, Jayakrishnapuram, 2006 Rajahmundry – 533 105, East Godavari District, Andhra Pradesh. (State University) 3. Andhra University, Waltair, Visakhapatnam-530 003, Andhra Pradesh. 1926 (State University) 4. Bharatiya Engineering Science and Technology Innovation University, 17.02.2019 Gownivaripalli, Gorantla Mandal, Anantapur, Andhra Pradesh (Private University) 5. Central University of Andhra Pradesh, IT Incubation Centre Building, 05.08.2019 JNTU Campus, Chinmaynagar, Anantapuramu, Andhra Pradesh- 515002 6. Centurion University of Technology and Management, Gidijala Junction, 23.05.2017 Anandapuram Mandal, Visakhapatnam – 531173, Andhra Pradesh. (Private University) 7. Damodaram Sanjivayya National Law University, Plot No. 116, Sector 2008 11 MVP Colony, Visakhapatnam – 530 017, Andhra Pradesh. (State University) 8. Dr. Abdul Haq Urdu University, Kurnool- 518001, Andhra Pradesh 14.12.2018 (State University) 9. Dr. B.R. Ambedkar University, Etcherla, Dt. Srikakulam-532410, 2008 Andhra Pradesh. (State University) 10. Dravidian University, Srinivasanam, -517 425, Chittoor District, 1997 Andhra Pradesh. (State University) 11. Dr. Y.S.R. Horticultural University, PO Box No. 7, 2011 Venkataramannagudem, West Godavari District – 536 101, Andhra Pradesh. (State University) 12. Dr. N.T.R. University of Health Sciences (Formerly Andhra Pradesh 1986 University of Health Sciences), Vijayawada-520 008, Andhra Pradesh. (State University) 13. -

Sumandeep Nursing College
Sumandeep Vidyapeeth Accredited by NAAC “A” grade with 3.53 CGPA Sumandeep nursing college Report on 5th national level conference TopIc: “RESEARcH METHoDoLoGY: ENHANCING INNOVATIVE AND FUTURISTIC PRACTICE IN NURSING” SUMANDEEP VIDYAPEETH SUMANDEEP NURSING COLLEGE Piparia, Waghodia, Vadodara – 391760 5TH NATIONAL LEVEL CONFERENCE – 2019 Date/ time: 4TH & 5TH JULY, 2019, 8.30 A.M to 4.30 P.M Organizing Chair Person: Dr. Ravindra H.N, Principal, SNC Organizing Seceretory: Mr. Nirmal Raj, HOD& Asso. Professor, Pediatric nursing Dept. Venue: SBKS MI & AUDITORIUM, SUMANDEEP VIDYAPEETH, PIPARIYA,WAGHODIYA, VADODARA BENEFICIARIES: - Nursing Students ( B.Sc. , P.B.B.Sc., M.Sc. Nursing from Sumandeep nursing college and Other colleges ) Teaching Faculties ( From Sumandeeep nursing college as well as other colleges) Theme Of 5th National Conference: Research methodology: Enhancing innovative & futuristic practice in nursing RESOURCE PERSON: Total 10 eminent resource persons were there for different sessions: Dr. T. Sivabalan, DR.PRAGNA DABHI,DR.CHANDRAMANI B. MORE , DR.ANIL SHARMA , SHRI KANDARP N TALATI, DR.MEDHA WADHWA, DR.MONALI SHAH, DR.JAYSHREE GANJIWALE, DR.NEERAJ PANDIT, MR. MAYUR SHINDE SCHEDULE PLAN 4TH JULY 2019 Time Event 8.30-9.00am Registration 9.00-9:15am Key note address by Principal Sir 9:30-10.30am Scientific Session 1 10.30-11am Inauguration Ceremony 11-11.15am Tea Break 11.15-11.45am Scientific Session 2 11:45-12:45pm Scientific Session 3 1.00-2.00pm Lunch 2.00-3.00pm Scientific Session 4 3.15-4:15pm Scientific Session 5 4:15pm Tea Break 5th July 2019 Time Event 9.00-10:30am Scientific Session :6 10:30-10:45am Tea break 10:45-12:00pm Scientific Session 7 12-1.00 pm Scientific Session:8 1.00-2.00pm Lunch 2.30-3.30pm Scientific Session 9 3.30-5.00pm Scientific Session 10 5.00pm Valedictory session INTRODUCTION Research is a major force in Nursing, and the evidence generated from research is changing practice, education, and health policy. -
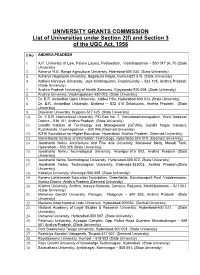
List of Universities Under Section 2(F) and Section 3 of the UGC Act, 1956
UNIVERSITY GRANTS COMMISSION List of Universities under Section 2(f) and Section 3 of the UGC Act, 1956 S.No ANDHRA PRADESH 1. A.P. University of Law, Palace Layout, Pedawaltair, Visakhapatnam – 530 017 (A. P) (State University). 2. Acharya N.G. Ranga Agricultural University, Hderabad-500 030. (State University) 3. Acharya Nagarjuna University, Nagarjuna Nagar, Guntur-522 510. (State University) 4. Adikavi Nannaya University, Jaya Krishnapuram, Rajahmundry – 533 105, Andhra Pradesh. (State University) 5. Andhra Pradesh University of Health Sciences, Vijayawada-520 008. (State University) 6. Andhra University, Visakhapatnam-530 003. (State University) 7. Dr. B.R. Ambedkar Open University, Jubilee Hills, Hyderabad-500 033. (State University) 8. Dr. B.R. Ambedkar University, Etcherla – 532 410 Srikakulam, Andhra Pradesh (State University) 9. Dravidian University, Kuppam-517 425. (State University) 10. Dr. Y.S.R. Horticultural University, PO Box No. 7, Venkataramannagudem, West Godavari District – 536 101, Andhra Pradesh. (State University) 11. Gandhi Institute of Technology and Management (GITAM), Gandhi Nagar Campus, Rushikonda, Visakhapatman – 530 045.(Deemed University) 12. ICFAI Foundation for Higher Education, Hyderabad, Andhra Pradesh. (Deemed University) 13. International Institute of Information Technology, Hyderabad-500 019. (Deemed University) 14. Jawaharlal Nehru Architecture and Fine Arts University, Mahaveer Marg, Masab Tank, Hyderabad – 500 028 (State University) 15. Jawaharlal Nehru Technological University, Anantpur-515 002, Andhra Pradesh (State University) 16. Jawaharlal Nehru Technological University, Hyderabad-500 072. (State University) 17. Jawaharlal Nehru Technological University, Kakinada-533003, Andhra Pradesh.(State University) 18. Kakatiya University, Warangal-506 009. (State University) 19. Koneru Lakshmaiah Education Foundation, Greenfields, Kunchanapalli Post, Vaddeswaram, Guntur District, Andhra Pradesh (Deemed University) 20. -

University Grants Commission
UNIVERSITY GRANTS COMMISSION Total No. of Universities in the Country as on 22.02.2017 Universities Total No. State Universities 359 Deemed to be Universities 123 Central Universities 47 Private Universities 260 Total 789 1 S.No ANDHRA PRADESH Date/Year of Notification/ Establishment 1. Acharya Nagarjuna University, Nagarjuna Nagar-522510, Dt. Guntur, Andhra 1976 Pradesh. (State University) 2. Adikavi Nannaya University, 25-7-9/1, Jayakrishnapuram, Rajahmundry – 533 2006 105, East Godavari District, Andhra Pradesh. (State University) 3. Andhra University, Waltair, Visakhapatnam-530 003, Andhra Pradesh. (State 1926 University) 4. Damodaram Sanjivayya National Law University, Plot No. 116, Sector 11 MVP 2008 Colony, Visakhapatnam – 530 017, Andhra Pradesh. (State University) 5. Dr. B.R. Ambedkar University, Etcherla, Dt. Srikakulam-532410, Andhra 2008 Pradesh. (State University) 6. Dravidian University, Srinivasanam, -517 425, Chittoor District, Andhra 1997 Pradesh. (State University) 7. Dr. Y.S.R. Horticultural University, PO Box No. 7, Venkataramannagudem, 2011 West Godavari District – 536 101, Andhra Pradesh. (State University) 8. Dr. N.T.R. University of Health Sciences (Formerly Andhra Pradesh University 1986 of Health Sciences), Vijayawada-520 008, Andhra Pradesh. (State University) 9. Gandhi Institute of Technology and Management (GITAM), Gandhi Nagar 13.08.2007 Campus, Rushikonda, Visakhapatman – 530 045, Andhra Pradesh.(Deemed University) 10. Jawaharlal Nehru Technological University, Anantpur-515 002, Andhra 2008 Pradesh (State University) 11. Jawaharlal Nehru Technological University, Pithapuram Road, Kakinada- 2008 533003, East Godvari District, Andhra Pradesh.(State University) 12. Koneru Lakshmaiah Education Foundation, Greenfields, Kunchanapalli Post, 20.02.2009 Vaddeswaram, Guntur District-522002, Andhra Pradesh. (Deemed University) 13. Krishna University, Andhra Jateeya Kalasala, Campus, Rajupeta, 2008 Machllipatanam – 521 001, Krishna District, Andhra Pradesh. -

1 Acharya Nagarjuna University 2 Adikavi Nannaya University 3
1 Acharya Nagarjuna University 2 Adikavi Nannaya University 3 Andhra University Centurion University of Technology and Management, Andhra 4 Pradesh 5 Damodaram Sanjivayya National Law University 6 Dr. Abdul Haq Urdu University, Kurnool- 518001, Andhra Pradesh 7 Dr. B.R. Ambedkar University 8 Dravidian University 9 Dr. Y.S.R. Horticultural University Dr. N.T.R. University of Health Sciences (Formerly Andhra Pradesh 10 University of Health Sciences) Gandhi Institute of Technology and Management (GITAM), Gandhi 11 Nagar 12 Jawaharlal Nehru Technological University, Anantpur-515 002 Jawaharlal Nehru Technological University, Pithapuram Road, 13 Kakinada 14 Koneru Lakshmaiah Education Foundation KREA University, 5655, Central, Expressway, Sri City-517646, 15 Andhra 16 Krishna University 17 Rashtriya Sanskrit Vidyapeeth 18 Rayalaseema University 19 Saveetha Amaravati University 20 Sri Krishnadevaraya University 21 Sri Padmavati Mahila Vishwavidyalayam Sri Sathya Sai Institute of Higher Learning, Prasanthinilayam, 22 Anantapur-515 23 Sri Venkateswara University 24 Sri Venkateswara Vedic University 25 Sri Venkateswara Veterinary University 26 Sri Venkateswara Institute of Medical Sciences 27 SRM University, Andhra Pradesh Vignan's Foundation for Science, Technology and Research, 28 Vadlamudi, 29 Vikrama Simhapuri University, Kakutur 30 VIT-AP University, Amravati 31 Yogi Vemana University 32 Apex Professional University 33. Arunachal University of Studies 34 Arunodaya University 35 Himalayan University 36 North East Frontier Technical University -

Sumandeep Nursing College
SUMANDEEP NURSING COLLEGE Piparia, Waghodia, Vadodara – 391760 STATE LEVEL CONFERENCE"MIDWIVES, MOTHERS AND FAMILIES: PARTNERS FOR LIFE!" Date / time : 13th DECEMBER, 2017, 8:30 am to 5.00 pm. Organizing Chairperson : Dr. Ravindra H.N. Organizing Secretary : Mrs. Vrutipatel Organizers : Faculty of Nursing Venue :Auditorium, SBKS MI & RC Beneficiaries :Nurse Educators, Nurse Administrators, Diploma, PG & UG Nursing Students, Staff Nurses, Alumni from SNC Gujarat Nursing Council awarded “5” credit points for state level Conference 2017. Registration Details: 563 Delegates from different nursing colleges of different districts participated in the state level Conference. Total30 colleges/institutes/hospitals participated in the state level conference. Nursing professionals, faculties, Postgraduate students and Ph.D scholars from different district had attended the state level conference. OBJECTIVES: Enhance nurses’ knowledge regarding early identification and management of risk pregnancies. Light on the current vital statistics and understand the measures to prevent maternal mortality. Find the opportunities for counseling on psychological and social aspect of pregnancy, childbirth and early parenting. Understand the recent advancement in midwifery practice with evidence based approach. With the advancement of midwifery education, enhance nurses' knowledge regarding advances in the care and treatment of pregnant women. Provides best opportunity to reach the largest assemblage of participants from the Nursing community. Provides opportunity to view midwifery as an independent profession. Acknowledge/discuss/ opine the midwifery nursing profession for the welfare of self and human society. CHIEF GUEST: Smt. JashubenPatidar, Ex- Registrar, Gujarat nursing council GUEST OF HONORS: Dr. Manoj Sattigeri, Registrar, Sumandeep Vidyapeeth KEY NOTE ADDRESS SPEAKER: Lt. Col. Shobha Naidu Director, Symbiosis College of Nursing, Symbiosis International University Pune, Maharashtra. -

Smt. NHL Municipal Medical College, Ahmedabad Regional Centre in Medical Education Technologies First Basic Course Workshop
Smt. NHL Municipal Medical College, Ahmedabad Regional Centre in Medical Education Technologies First Basic Course Workshop Date of Workshop: July 1- 3, 2009 Name of Observer: Nil List of Participants Sr. Name of Designation and Official Contact E-mail ID No. Participant Department Address Details (Tel./ Fax/Mobile) 1. Dr. Kiran Assistant Professor, S.B.K.S. Medical 9427320782 [email protected] Tripathi Department of Institute & Microbiology Research Centre, Pipariya 2. Dr. Dimple Assistant Professor, S.B.K.S. Medical 0265 - [email protected] Darad Department of Institute & 2322858 Pathology Research Centre, 9825288185 Pipariya 3. Dr. U.I. Sr. Tutor, S.B.K.S. Medical 904840340 NA Bhatt Department of Institute & Physiology Research Centre, Pipariya 4. Dr. Jitendra Assistant Professor, S.B.K.S. Medical 9426759749 [email protected] Zaveri Department of Institute & Pharmacology Research Centre, Pipariya 5. Dr. Niraj Associate Professor, S.B.K.S. Medical 9825371135 [email protected] Pandit Department of Institute & Community Research Centre, Medicine Pipariya 6. Dr. Hetal Associate Professor, S.B.K.S. Medical 9998055159 [email protected] Pandya Department of Institute & Medicine Research Centre, Pipariya 7. Dr. Chaitri Assistant Professor, S.B.K.S. Medical 9924110147 [email protected] Shah Department of Institute & Medicine Research Centre, Pipariya 8. Dr. Lakhan Assistant Professor, S.B.K.S. Medical 9426334561 [email protected] Kataria Department of Institute & Psychiatry Research Centre, Pipaliy 9. Dr. Vijoy Professor, S.B.K.S. Medical 02668 - [email protected] Singh Department of Institute & 245028 Surgery Research Centre, 9974005726 Pipariya 10. Dr. -

List-Of-Universities-In-Gujarat-PDF
# Name Location Established Specialization Contact Number 1 Central University Of Gujarat Gandhinagar 2009 General 079 2326 0092 2 Gujarat Vidyapith Ahmadabad 1920 General 079 2754 0746 National Rail and Transportation 3 Vadodara 2018 Railway and Transport +91 8880922331 Institute 4 Sumandeep Vidyapeeth Piparia,��Waghodia,��Vadodara 2007 Dental, Medical, Management 02668 245 262 5 Ahmedabad University Ahmedabad 2009 General 079 6191 1200 Management, hospitality, law, IT, 6 Auro University Surat 2011 0261 408 8100 fashion, interior, mass communication teaching, research in Arts, Commerce, Science, Engineering, Medicine, 7 Bhavnagar University Bhavnagar 1978 02697 265 011 Management, Rural Studies and Law Faculties Charotar University of Science and 8 Anand 2009 Science, technology 02697 265 011 Technology 9 Dharamsinh Desai University Nadiad 1968 Technology 0268 252 0502 Dhirubhai Ambani Institute of 10 Information and Communication Gandhinagar 2001 Technology 079 6826 1700 Technology 11 Ganpat University Mehsana 2005 General 02762 286 080 12 Indus University Ahmedabad 2006 Technology 090999 44242 13 Kadi Sarva Vishwavidyalaya Gandhinagar 2007 General 079 2324 4690 Engineering, Arts, Commerce, Science, 14 Marwadi University, Rajkot Rajkot 2016 281-7123456 Management, Law Faculties 15 MICA Ahmedabad 1992 Communication 02717 308 250 Nirma University of Science and 16 Ahmedabad 1998 Technology 079 7165 2000 Technology School of Engineering, School of Science, School of physiotherapy, 17 P P Savani University Surat 2016 School of Nursing, School -

Curriculum Vitae of Urmi Nanda Biswas
Curriculum Vitae of Urmi Nanda Biswas Dr. Urmi Nanda Biswas, Professor, Department of Psychology, Faculty of Education and Psychology, The M. S. University of Baroda, Vadodara. Contact: Mobile- 0091-9737422624 e-mail: [email protected] [email protected] Gender: Female; Nationality: Indian Present Position: Professor, Department of Psychology, The M. S. University of Baroda, Vadodara. Education 1995-Post Doctoral Research with fellowship from UGC, S.P. University, Vallabh Vidyanagar,, Gujarat. 1993 - Doctor of Philosophy (Ph. D) in Psychology with UGC NET( JRF and SRF), Allahabad University, Allahabad, UP. 1986 - Master of Arts (Psychology), Utkal University, Bhubaneswar, OdIsha. 1984 -Bachelor of Arts (Psychology Honors and Statistics), Utkal University, Bhubaneswar, Odisha. Additional Diploma/Certificates 2004 - PG Diploma in Clinical and Applied Hypnotherapy. The M. S. University of Baroda, Gujarat. 2004 - Certified Trainer for Counselors of Voluntary Centre for Testing and Counseling (VCTC), National AIDS Control Organization (NACO), India. Fellowships/ Scholarships/ Awards • 2014 (April) Awarded Guest Professor Grant from FORTE (Swedish Research Council for Health, Working Life and Welfare) for three months to visit Department of Sociology and Work Science, Gothenberg University, Sweden. • 2014 (January). Awarded Planning Grant from Gothenberg Centre for Global Development, Gothenberg,Sweden. 1 • 2008-Collaborative Delivery Award for short term course development under UKIERI scheme of British Council. • 2006-Awarded Commonwealth Academic Staff Fellowship (CASF) of British Council and Commonwealth Secretariat, UK in 2006 and was engaged as a visiting faculty at the University of Roehampton, UK. • 2003-Recipient of the best research paper award in the International Seminar of Indian Association of Applied Psychology held in Jodhpur during October 11-13, 2003.