Custom Sandal and Clog Program 2016
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Viimeinen Päivitys 8
Versio 20.10.2012 (222 siv.). HÖYRY-, TEOLLISUUS- JA LIIKENNEHISTORIAA MAAILMALLA. INDUSTRIAL AND TRANSPORTATION HERITAGE IN THE WORLD. (http://www.steamengine.fi/) Suomen Höyrykoneyhdistys ry. The Steam Engine Society of Finland. © Erkki Härö [email protected] Sisältöryhmitys: Index: 1.A. Höyry-yhdistykset, verkostot. Societies, Associations, Networks related to the Steam Heritage. 1.B. Höyrymuseot. Steam Museums. 2. Teollisuusperinneyhdistykset ja verkostot. Industrial Heritage Associations and Networks. 3. Laajat teollisuusmuseot, tiedekeskukset. Main Industrial Museums, Science Centres. 4. Energiantuotanto, voimalat. Energy, Power Stations. 5.A. Paperi ja pahvi. Yhdistykset ja verkostot. Paper and Cardboard History. Associations and Networks. 5.B. Paperi ja pahvi. Museot. Paper and Cardboard. Museums. 6. Puusepänteollisuus, sahat ja uitto jne. Sawmills, Timber Floating, Woodworking, Carpentry etc. 7.A. Metalliruukit, metalliteollisuus. Yhdistykset ja verkostot. Ironworks, Metallurgy. Associations and Networks. 7.B. Ruukki- ja metalliteollisuusmuseot. Ironworks, Metallurgy. Museums. 1 8. Konepajateollisuus, koneet. Yhdistykset ja museot. Mechanical Works, Machinery. Associations and Museums. 9.A. Kaivokset ja louhokset (metallit, savi, kivi, kalkki). Yhdistykset ja verkostot. Mining, Quarrying, Peat etc. Associations and Networks. 9.B. Kaivosmuseot. Mining Museums. 10. Tiiliteollisuus. Brick Industry. 11. Lasiteollisuus, keramiikka. Glass, Clayware etc. 12.A. Tekstiiliteollisuus, nahka. Verkostot. Textile Industry, Leather. Networks. -

Gandy – an Old Established Shoemaking Family
Gandy – an old established shoemaking family Throughout the 19 th century, census, church and other records for the Warrington area contain a wealth of evidence for the Gandy’s involvement in the shoe-making trade and other trades with links to footwear, such as hosiery. For example John Gandy was a hosier in The Market Place and Golden Square in Warrington in the 1820`s while Mrs Mary Gandy served the nobility, gentry and clergy in Church Street and Horsemarket Street. (Information provided by Sue Kinsella from trade directories). The connection between the Gandy family and shoes is even older. I have found Gandys who were shoemakers in the 18 th century, such as William Gandy of Prescot, who married Sarah Lingham in 1767 and John Gandy, also shoemaker of Prescot, who married Jane Whittle in 1768. Thomas Gandy, cloger, married Mary Houghton in 1826. James Gandy shoemaker married Ann Smethurst in 1761. Thos Gandy shoemaker married Ann Mason in 1768. Joseph Gandy shoemaker married Betty Wright in 1769. James Gandy shoemaker and wife Ann – christened son James in 1779 and daughter Lydia in 1782. Joseph Gandy, John Gandy, Thomas, James shoemakers carried on 1785, 1787, 1788, 1790,1795, 1796, - 1808. Warrington volunteers raised in 1798 to help meet the threat of invasion from Napoleonic France. 539 men serving in 1807, including James Gandey, Warrington, shoemaker. Another speciality of the Gandy cobblers was clogs: “When you talk of clogs in Warrington, people immediately think of the Gandy’s. And when you mention that name to-day you are referring to 70-year-old Mr. -

Berufsschuh-Katalog GB__7.16.Pdf
U2 SIEHE UMSCHLAG i Dear business partner, dear customer, the basis of a high quality shoe is besides the techni- cal expertise and know-how the passion for shoes. Understanding and respect for the person and his needs in everyday worklife are ABEBAs major motivation for the developement of safety and occu- pational shoes. By living this philosophy we create the difference: Perfect protection, a healthy foot climate and best wearing comfort for an every day use. Our demand is to exceed your demands! Our main focus is to offer the best quality products therefore we make the highest demands on the materials used and the most accurate way of manufacturing. ABEBA is one of the largest and most modern shoe manufacturers in Europe with customers in more than 30 countries worldwide. With our German warehouse, our French subsidiary and our production facilities in several European countries we are always ready to meet your demands. Since 1st of June 2007 ABEBA is part of the traditio- nal Polish shoe manufacturer Protektor. The Protektor S.A. is listed at the Warsaw stock exchange. ABEBA safety and occupational shoes are exclusi- vely available at specialized dealers and distributors in worldwide more than 2.000 outlets with specially trained personnel. Together with our European sales team we are happy to answer your questions about ABEBA and our products. We can assure you that we will find the best solution customized to your particular needs. Thank you for the trust in our company! Your team OCCUPATIONALSHOES | 3 CONTENT 16 THE ORIGINAL The clog that convinces OCCUPATIONAL SHOES 26 HIGH ORIGINAL The classic with wedge heel 28 THE ORIGINAL PLUS Comfortable and washable Imprint Editor: 30 DYNAMIC ABEBA Spezialschuh-Ausstatter GmbH Athletic design with lifestyle Schlackenbergstrasse 5 D-66386 St. -

Catalogus Wock's Beroepsschoen
feetsIt yourindividuality OPTIMALE PRESTATIES. Voor professionals die in de meest veeleisende omgevingen werken, is de CLOG het ideale schoeisel. De antistatische CLOG is gemaakt van Steri-Tech™, een hoogwaardig polymeer dat in de autoclaaf kan worden gesteriliseerd, hetgeen garant staat voor optimale hygiëne. In combinatie met het comfort dat het schokdempingsysteem biedt, haal je het einde van de dag in perfecte conditie. Bovendien is de klomp in 12 verschillende kleuren verkrijgbaar die volledig aansluiten bij jouw stijl. !"'.//"0 #$%&'()*(+(*%,-("# Ideaal voor: Ziekenhuizen en andere zorginstellingen Bedrijven gespecialiseerd in cosmetica/verzorgingsproducten Farmaceutische industrie Schoonmaakbedrijven Voedingsindustrie Cateraars Specifcaties: Steriliseerbaar: de CLOG is ontwikkeld! voor professionals die werkzaam zijn in omgevingen waarin de hoogste eisen worden gesteld aan hygiÎ ne. De klomp is * gemaakt van Steri- Tech?, een hoogwaardig polymeer dat ervoor zorgt dat de klomp en de inlegzool in de autoclaaf kunnen worden gesteriliseerd tot een temperatuur van 134 C. Schokdemping: De inlegzool is ontwikkeld om de meest veeleisende professionals optimaal comfort te bieden. De innovatieve geometrische vormgeving van de inlegzool zorgt ervoor dat schokken worden geabsorbeerd, minuscuul letsel van pezen, botten en gewrichten wordt voorkomen en het gevoel van vermoeide benen afneemt. ** * MN,)')(/"'()'*/',%"$9-,,.'5$&*/)'4/0"/&(-(0//&*'/)'6,)',--//)'()'*/'5,03,98()/'5$&*/)'4/5,00/)'"$"'OPQR:''''''''MMS/-*"',--//)'+$$&'RJFS''K<;: STERILISEERBAAR De Clog en de inlegzool zijn gemaakt van Steri-Tech- TM, een hoogwaardig polymeer, zodat de klomp in een autoclaaf tot 134ºC kan worden gesteriliseerd. BESCHERMING BOVENVOET Voorkomt dat vocht in de klomp loopt. SCHOKDEMPING Vermindert minuscule afwijkingen in pezen, botten en gewrichten, waardoor het gevoel van vermoeide benen afneemt. VENTILEREND ANTISTATISCH Regelt de temperatuur en vochtigheid van de voet. -

Personnel, Planning & Policy Committee Meeting
NOTICE OF MEETING Inhabitants of the Town of Amherst: You are hereby notified that there will be a meeting of: Public Body: The Jones Library, Inc. Personnel, Planning and Policy Committee Date: Thursday, August 12, 2021 Time: 4-5pm Location: Zoom Webinar ADVISORY TO THE PUBLIC: This special Jones Library Personnel, Planning and Policy Committee meeting will occur virtually via ZOOM and will be streamed live here: You are invited to a Zoom webinar. When: Aug 12, 2021 04:00 PM Eastern Time (US and Canada) Topic: The Jones Library, Inc. Personnel, Planning, and Policy Committee Please click the link below to join the webinar: https://amherstma.zoom.us/j/81703664637 Or One tap mobile : US: +13017158592,,81703664637# or +13126266799,,81703664637# Or Telephone: Dial(for higher quality, dial a number based on your current location): US: +1 301 715 8592 or +1 312 626 6799 or +1 646 876 9923 or +1 669 900 6833 or +1 253 215 8782 or +1 346 248 7799 or +1 408 638 0968 Webinar ID: 817 0366 4637 International numbers available: https://amherstma.zoom.us/u/kc8f97qdL Meeting Agenda I. Call to Order II. Minutes * III. Proposed Deaccessions * IV. Jones Library Plan for Phased Resumption of Services to the Public o Masks Required o Open Hours Schedule * o 50% Meeting Room Occupancies (Woodbury 62; Amherst 12; Goodwin 25) V. Director Annual Evaluation Forms * VI. Adjournment ** Please note that the list of topics in this notice was comprehensive at the time of posting, however the public body may consider and take action on unforeseen matters not specifically named in this notice. -

Create Your Clog Table of Contents
CREATE YOUR CLOG TABLE OF CONTENTS Pick a Base – There are three base colors to choose from Black, 1 Brown (stained), and White (natural). Materials & Colors –Clogs & Sandals are available in the following 2 colors and leather types Patents Materials & Colors Flat Leather – same as patent Nubuc Leathers - same as patent Suede - same as patent Optional Design Features – Clogs & Sandals are available with 3 optional design features such as straps, braids, or mowhawks. Mix & Match Samples Please contact us at [email protected] to arrange for samples CLOG FEATURES Not only are our clogs custom fit, they are custom made for you. You chose the color of the leather, wooden base color, and which style you like. You can even mix and match different colors or different types of leathers on your pair of clogs. Your clogs will be as unique as you are. Ultra Durability Wood will never wear to your incorrect walking or standing pattern, so you are always in alignment. Water Resistant Our flat and patent leathers have a coating that make them water resistant. The light weight wood base with a molded polyurethane sole is skid resistant. Super Comfort The full benefit of CLOGS can only be accomplished if the top fits your foot properly. We feel that when it does, you can walk all day without gripping with your toes to keep the CLOGS on, making this a very therapeutically correct and comfortable shoe. PICK A BASE Pick a Base – There are three base colors to choose from 1 Black, Brown (stained), and White (natural). -
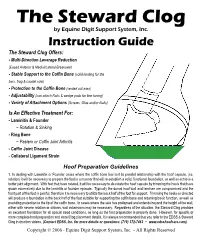
The Steward Clog by Equine Digit Support System, Inc
The Steward Clog by Equine Digit Support System, Inc. Instruction Guide The Steward Clog Offers: - Multi-Direction Leverage Reduction (Eased Anterior & Medial/Lateral Breakover) - Stable Support to the Coffin Bone(solid landing for the bars, frog & caudal sole) - Protection to the Coffin Bone (seated out area) - Adjustability (can attach Rails & wedge pads for fine tuning) - Variety of Attachment Options (Screws, Glue and/or Nails) Is An Effective Treatment For: - Laminitis & Founder ~ Rotation & Sinking - Ring Bone ~ Pastern or Coffin Joint Arthritis - Coffin Joint Disease - Collateral Ligament Strain Hoof Preparation Guidelines 1. In dealing with Laminitis or Founder cases where the coffin bone has lost its parallel relationship with the hoof capsule, (i.e. rotation) it will be necessary to prepare the foot in a manner that will re-establish a solid, functional foundation, as well as achieve a better joint alignment. With feet that have rotated, it will be necessary to de-rotate the hoof capsule by trimming the heels that have grown excessively due to the laminitis or founder episode. Typically the dorsal hoof wall and laminae are compromised and the front part of the foot is painful, therefore it is necessary to utilize the back half of the foot for support. Trimming the heels as directed will produce a foundation in the back half of the foot suitable for supporting the coffin bone and returning basic function, as well as providing protection to the tip of the coffin bone. In cases where the sole has prolapsed and extends beyond the height of the wall, either with severe rotation or sinkers, wall extensions may be necessary. -

Full-Scale Laboratory Testing of a Toe Drain with a Geotextile Sock DSO-99-14
Full-Scale Laboratory Testing of a Toe Drain with a Geotextile Sock DSO-99-14 Materials Engineering and Research Laboratory April 1999 Full-Scale Laboratory Testing of a Toe Drain with a Geotextile Sock DSO-99-14 by Jay Swihart U.S. Department of Interior Bureau of Reclamation Dam Safety Office April 1999 UNITED STATES DEPARTMENT OF THE INTERIOR BUREAU OF RECLAMATION Full-Scale Laboratory Testing of a Toe Drain with a Geotextile Sock Executive Summary This report describes the full-scale laboratory testing (pipe box testing) of a 15-inch-diameter, corrugated, polyethylene toe drain with a knitted geotextile sock, backfilled with a sand envelope material. The test results are compared with previous small-scale and full-scale tests using perforated pipe with 1/8-inch and 1/4-inch perforations, but no geotextile. Use of the geotextile optimized toe drain performance both with respect to flow and with respect to loss of the sand envelope. The long-term flow rate was 21 gpm per linear foot of pipe, which was significantly higher (by a factor of 3 to 12) than the earlier tests without geotextile. The total loss of sand envelope was only 50 grams per linear foot of pipe, which was significantly lower (by a factor of 4 to 17) than the earlier tests without geotextile. The test with geotextile was run for 31 days at a constant head of 2½ feet above the pipe invert with no indication of clogging. The results from this test with geotextile along with the two previous tests without geotextile are summarized below: Test Configuration Flow Rate Envelope Loss Test Duration and (gpm / lin ft) (grams / lin ft) Comments 1/8-inch slots 1.74 Not Stable 200 Stable 8 Days - Not Stable 1/4-inch holes 6.3 Not Stable 850 Not Stable 24 Days - Not Stable Geotextile Sock 21.3 Stable 50 Stable 31 Days - Stable Improvements with 3 to 12 4 to 17 Geotextile (factor) Based on these results, use of geotextile sock in conjunction with a sand envelope is recommended for all future toe drain installations in areas with fine native soils. -

The Crocs Comeback
The Crocs Comeback Crocs #FindYourFun Campaign 2015 The Crocs Comeback 1 Summary Crocs was a brand that used to be great. For years they dominated the casual-shoe corner of the market. But eventually the fad wore out…and Crocs became irrelevant. The planning team faced a difficult task: We needed to breathe life back into a brand that few cared about anymore. As we dove into research, we uncovered a simple but important truth: Crocs are fun. They’re bright and colorful, but more than that, they’re the shoes you wear when you want to be comfortable and be yourself. This concept of self-expression came up over and over again. People all around the world are hungry for it. Why? Because “being you” is fun. It was clear that we needed to turn Crocs into the brand that stands for fun. But how? We took another look at the polarizing clog. Where others saw weakness, we saw opportunity. The clog was more than just a shoe, it was a globally recognized symbol of the brand. Rather than ignore it, we needed to do the exact opposite. We needed to turn it into a global icon of fun. The campaign came to life through the #FindYourFun creative platform — it was simple, straightforward and universal. The message encouraged everyone around the world to celebrate fun in the everyday. The Crocs Comeback 2 Remember when Crocs were a thing? Back in 2002, when Ja Rule was topping the charts and cellphones still flipped, the But, after a decade of climbing, Crocs first Crocs shoe was introduced at the began to lose momentum. -

Vera Bradley and Crocs Create New Limited-Edition Footwear Collection
Vera Bradley and Crocs Create New Limited-Edition Footwear Collection August 25, 2020 New collection to debut on August 25, Vera Bradley + Crocs Collection followed by a special edition Crocs At Work™ collection and first-ever children’s collection on September 8 FORT WAYNE, Ind. and NIWOT, Colo., Aug. 25, 2020 (GLOBE NEWSWIRE) -- Vera Bradley, Inc. (Nasdaq: VRA), the iconic women’s fashion and lifestyle brand, and Crocs, Inc. (Nasdaq: CROX), a global leader in innovative casual footwear, announced a new limited-edition footwear collection debuting today. The two iconic brands partnered for the second time to expand the Vera Bradley + Crocs exclusive footwear collection, combining Vera Bradley’s signature bright florals and paisley designs with Crocs’ world-renowned comfort. The brands’ first highly successful collaboration Vera Bradley + Crocs Collection launched in July 2019. The Vera Bradley + Crocs footwear collection is available in Crocs’ most popular silhouettes: the Vera Bradley + Crocs Collection iconic Classic Clog and the Classic Slide. This one-of-a-kind collaboration features two colorful patterns – Floating Garden and Sunny Garden – and is designed to make every day feel more bright, fun and cheerful. Of course, no collection would be complete without the ability to personalize! As part of this launch, new Vera Bradley + Crocs Jibbitz™ Charms 3-packs will be available to add even more playfulness and cheer to every step. Rob Wallstrom, Chief Executive Officer of Vera Bradley, noted, “The success of our first Vera Bradley + Crocs footwear collection that debuted last summer proved that both of our fans love fashion, function, and fun, making our collaboration the perfect pairing. -

Download (PDF)
COLLECTION 2019/2020 WORK FOOTWEAR FOR HOTELS, RESTAURANTS, CANTEENS, CATERING 2 Some people just go a little further for others. From the hardworking chef in the kitchen to the busy server in the restaurant or café. This requires footwear that is not only approved for work but that also feels right. Even after a long shift. At Sika Footwear we have a wide range of work footwear for hotels, restaurants, canteens and catering. Our products are developed in close collaboration with users, and are designed to provide maximum comfort and safety in the workplace. In this catalogue you will find exactly the right work footwear for your industry and your job. Happy reading. CONTENTS 4 Footwear made for work 6 Work shoes and sandals 26 Work clogs 30 Accessories FIND THE ENTIRE ASSORTMENT AT WWW.SIKAFOOTWEAR.EU Footwear made for work At Sika Footwear we develop, manufacture and supply footwear for working people. From the restaurant server with the long shift to the contractor who builds roads and bridges. Needs vary, but one thing remains the same: Footwear should fit, both to the feet and to the work that needs doing! Sika Footwear is a Danish company which took its first steps back in 1870. Not that longevity is synonymous with quality, but it is difficult to argue against nearly 150 years of insight and refinement. Today we use the knowledge to develop our own products from scratch, as well as selecting and marketing the very best brands on the market. Yes, we know a lot about footwear at Sika Footwear. -

Stepping Into History at the Bata Shoe Museum Zapatos Y Sociedad: Caminando Por La Historia En El Bata Shoe Museum
CORE Metadata, citation and similar papers at core.ac.uk Provided by Revistes Catalanes amb Accés Obert Shoes and Society: Stepping into History at the Bata Shoe Museum Zapatos y sociedad: caminando por la historia en el Bata Shoe Museum Elizabeth Semmelhack Senior Curator of the Bata Shoe Museum The Bata Shoe Museum 327, Bloor Street West Toronto (ON), Canadá M5S 1W7 [email protected] Recepción del artículo 19-07-2010. Aceptación de su publicación 17-08-2010 resumen. El Bata Shoe Museum de Toronto (Ca- abstract. The Bata Shoe Museum in Toronto, nadá) es el museo de zapatos más grande de Nor- Canada is the largest shoe museum in North teamérica y alberga una colección de casi trece mil America and houses a collection of nearly 13,000 objetos que abarcan cuatro mil quinientos años de artifacts spanning 4,500 years of history. It is a cen- historia. Es, además, un centro internacional de in- tre for international academic research with a man- vestigación cuyo objetivo es el estudio, la exposi- date to study, exhibit, and publish on the cultural, ción y la publicación de trabajos académicos y cien- historical and sociological significance of footwear. tíficos sobre el significado cultural, histórico y -so The museum opened its doors to the public on ciológico del calzado. El museo abrió sus puertas May 6, 1995 and was established by Mrs. Sonja Bata al público el 6 de mayo de 1995 y fue fundado por as an independent, non-profit institution to house Sonja Bata como una institución independiente y and exhibit her renowned personal collection of sin ánimo de lucro cuya función primordial era al- historic and ethnographic footwear.