Instrumentation for Minimally Invasive Surgery in Pediatric Urology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

STILLE Surgical Instruments Kirurgisk Perfektion I Närmare 180 År Surgical Perfection for Almost 180 Years
STILLE Surgical Instruments Kirurgisk perfektion i närmare 180 år Surgical Perfection for almost 180 years I närmare 180 år har vi utvecklat och tillverkat de bästa kirurgiska For almost 180 years, we have developed and manufactured the best instrumenten till världens mest krävande kirurger. Vi vill rikta ett stort surgical instruments for the world’s most demanding surgeons. tack till alla våra trogna kunder och samtidigt välkomna våra nya kunder. We would like to extend a heartfelt thank you to all our loyal I den här katalogen presenterar vi vårt kompletta sortiment av customers and a warm welcome to our new customers. In this catalog STILLEs original instrument. we present our complete range of STILLE original surgical instruments. Precision, hållbarhet och känsla är typiska egenskaper för alla Precision, durability and feel are characteristic qualities of all STILLE STILLE-instrument. Den stora majoriteten är handgjorda av våra instruments. The vast majority are handcrafted by our highly skilled skickliga instrumentmakare Eskilstuna. Instrumentets resa från rundstål instrument makers in Eskilstuna, west of Stockholm, Sweden. The instru- till ett färdigt instrument är lång, och består av många tillverkningssteg. ments’ journey from a rod of stainless steel to a finished instrument is a STILLEs unika tillverkningsmetod och användning av enbart det bästa long one, involving multiple stages. STILLE’s unique method of crafting its materialet ger våra instrument deras unika känsla och hållbarhet. instrument materials, and its usage of only the very highest-grade steels, give our instruments their unique feel and durability. I det första kapitlet hittar du våra saxar, allt från vanliga operationssaxar till våra unika SuperCut och Diamond SuperCut-saxar. -

The Basic Surgery Kit
GLOBAL EXCLUSIVE > SURGERY > PEER REVIEWED The Basic Surgery Kit Jan Janovec, MVDr, MRCVS VRCC Veterinary Referrals Laurent Findji, DMV, MS, MRCVS, DECVS Fitzpatrick Referrals Considering the virtually limitless range of surgical instruments, it can be difficult to assemble a cost-effective basic surgery kit. Some instruments may misleadingly appear multipurpose, but their misuse may damage them, leading to unnecessary replacement costs or, worse, intraoperative accidents putting the patient’s safety at risk. Many instru- ments are available in different qualities and materials (eg, tungsten carbide instruments— more expensive but much more resistant to wear and corrosion than stainless steel) and Minimal Basic Surgery Kit varied sizes to match the purpose of their use as well as the size of the surgeon’s hand. n 1 instrument case Cutting Instruments n 1 scalpel handle Scalpel n 1 pair Mayo scissors The scalpel is an indispensible item in a surgical kit designed to make sharp incisions. Scalpel incision is the least traumatic way of dissection, but provides no hemostasis. n 1 pair Metzenbaum scissors Scalpel handles come in various sizes, each accommodating a range of disposable n 1 pair suture scissors blades (Figure 1). Entirely disposable scalpels are also available. n 1 pair Mayo-Hegar needle holder Scissors n 1 pair Brown-Adson tissue forceps Scissors are used for cutting, albeit with some crushing effect, and for blunt dissection. n 1 pair DeBakey tissue forceps Fine scissors, such as Metzenbaum scissors (Figure 2), should be reserved for cutting n 4 pairs mosquito hemostatic forceps and dissecting delicate tissues. Sturdier scissors, such as Mayo or suture scissors, are designed for use on denser tissues (eg, fascia) or inanimate objects (eg, sutures, drapes). -

STILLE Surgical Instruments
Selected Models STILLE Surgical Instruments Quality tools behind the talent Surgical Perfection ”The world’s best instruments, for the world’s best surgeons” STILLE Surgical Instruments For over 175 years, we have developed and manufactured the best surgical In this catalogue you will find a wide selection of instruments, Including the instruments for the world’s most demanding surgeons. We would like to original supercut scissor developed in 1984 and our new Diamond supercut extend a sincere thank you to all our current customers and welcome our design. Quality goes into our STILLE forceps, needle holders, clamps, rongeurs, future customers to experience the STILLE difference. In this catalog we curettes and retractors, as well as, a fine selection of stainless and titanium present a selection of STILLE original surgical instruments. micro instruments. Common to all of our instruments is that they are smooth and consistently perform to your expectations. Our outstanding balance, Precision, durability and feel are characteristic qualities of all STILLE solid design and ergonomics provides the surgeon with a reliable instrument instruments. The majority are handcrafted by our highly skilled artisans in throughout long and complex procedures. Eskilstuna, Sweden. Our instrument manufacturing process from melting steel rods to finished product is a long one, involving multiple stages of We at STILLE are proud to have developed the world’s first double-action development. Our method of crafting STILLE instruments involves only bone ronguer. We also developed the world’s first osteotome with the classic the highest-grade steel, which provides a unique feel and reliability to the 8-sided handle. -
Fine Surgical Instruments for Research™ Hsin-Yi Road, Sec
INTERNATIONAL Scissors, Bone Instruments Fine Science Tools Inc. & Scalpels 202-277 Mountain Highway pages 3–61 North Vancouver, British Columbia Canada V7J 3T6 Telephone 800-665-5355 / 604-980-2481 Fax 800-665-4544 / 604-987-3299 E-Mail [email protected] Web finescience.ca Fine Science Tools (USA) Inc. 373-G Vintage Park Drive F Forceps & Hemostats Foster City, California 94404-1139 I pages 63–97 Telephone 800-521-2109 / 650-349-1636 N Fax 800-523-2109 / 650-349-3729 E E-Mail [email protected] Web finescience.com S C I E Fine Science Tools GmbH N Vangerowstraße 14 C 69115 Heidelberg Germany E Telephone +49 (0) 62 21 - 90 50 50 Fax +49 (0) 62 21 - 90 50 590 T Probes, Needle Holders, O E-Mail [email protected] Thread, Retractors & Clamps Web finescience.de O pages 99–133 L S InterFocus Ltd. Pentagon Business Park Cambridge Road Linton, Cambridge CB21 4NN C United Kingdom A Telephone +44 (0)1223 894833 T Fax +44 (0)1223 894235 A Surgical & Laboratory E-Mail [email protected] L Accessories Web surgicaltools.co.uk O pages 135–161 G 2 Muromachi Kikai Co., Ltd. 0 4-2-12, Nihonbashi-Muromachi 1 Chuo-ku 4 Tokyo 103-0022 Japan Telephone (03) 3241-2444 Fax (03) 3241-2940 E-Mail [email protected] Student Quality Instruments Web muromachi.com pages 163–167 Proserv Instruments Co., Ltd. 7F-2, No. 413 Fine Surgical Instruments for Research™ Hsin-Yi Road, Sec. 4 Taipei, Taiwan R.O.C. Telephone (02) 27230455 Fax (02) 27230799 2014 E-Mail [email protected] Web proserv.com.tw TABLE OF CONTENTS | CATALOG 2014 Scissors 3 – 37 Spring 3 – 14 WE PROUDLY STOCK Fine 15 – 30 Surgical 31 – 37 Bone Instruments 38 – 51 DUMONT® Rongeurs 38 – 41 A selection of over 50 of the most popular Cutters 42 – 49 Other Bone Instruments 50 Dumont forceps are offered in this catalog. -

A Novel Right Ventricular Volume and Pressure Loaded Piglet Heart Model for the Study of Tricuspid Valve Function
Materials List for A Novel Right Ventricular Volume and Pressure Loaded Piglet Heart Model for the Study of Tricuspid Valve Function. Lily Q. Lin1, Sanaz Hatami2, James Yashu Coe1, Timothy M. Colen1, Consolato Sergi3, Richard Thompson4, Elena S. Di Martino5, Walter Herzog6, Ziad Abu Sara6, Darren H. Freed2, Nee Scze Khoo1 1Division of Pediatric Cardiology, Department of Pediatrics, University of Alberta 2Department of Surgery, University of Alberta 3Department of Laboratory Medicine and Pathology, University of Alberta 4Department of Biomedical Engineering, University of Alberta 5Department of Civil Engineering, University of Calgary 6Faculty of Kinesiology, University of Calgary Corresponding Author Citation Lily Q. Lin Lin, L.Q., Hatami, S., Coe, J.Y., Colen, T.M., Sergi, C., Thompson, R., Di Martino, E.S., [email protected] Herzog, W., Abu Sara, Z., Freed, D.H., Khoo, N.S. A Novel Right Ventricular Volume and Pressure Loaded Piglet Heart Model for the Study of Tricuspid Valve Function.. J. Vis. Exp. (), e61251, doi:10.3791/61251 (2020). Date Published DOI URL July 28, 2020 10.3791/61251 jove.com/video/61251 Materials Name Company Catalog Number Comments Drugs 1% lidocaine spray WDDC 103365 Lidodan 30 mL atropine sodium injection WDDC/Rafter 8 Products 0.5 mg/mL bupivacaine WDDC/Sterimax 5 mg/mL buprenorphine HCl slow release Chiron Compounding Pharmacy 1 mg/mL injection buprenorphine regular WDDC/Champion Alstoe 121378 Vetergesic 0.3 mg/mL cefazolin WDDC/Fresenius Kabi 102016 1 g/vial cephalexin capsule WDDC/Novopharm Novo-Lexin -

Care and Maintenance of Tissue and Dressing Forceps
Instrument Whisperer by Rick Schultz Care and Maintenance of Tissue and Dressing Forceps LTHOUGH TISSUE AND Q: What are atraumatic forceps? INSPECTING FORCEPS dressing forceps have a A: Atraumatic forceps are designed to Forcep inspection begins at the proximal relatively basic design, they minimize damage and trauma to the end, where the forcep is held. Inspect the require careful inspection to tissue. The most common styles are base of the forcep where the two halves Aensure surgeon satisfaction and patient Cooley and Debakey. are joined. Cracks commonly occur at safety. It is important to first understand the rivet and move to the edge. Inspect the answers to the following frequently the handle and tips for blood and tissue. asked questions. Dressing forceps must be inspected in the serrations, while the teeth of tissue forceps Q: What is the difference between tissue must be closely examined for bioburden. forceps and dressing forceps? Finally, inspect the distal tips to ensure A: Tissue forceps have teeth (e.g., 1x2, Q: The Operating Room (OR) places they meet evenly and don’t overlap. If 2x3, 3x4) that are designed to grasp forceps on the side of the tray. Is this the tips are out of alignment, remove the and manipulate tissue. Dressing forceps acceptable? forcep from the tray and send it out for have serrations instead of teeth, and A: Yes. However, placing forceps on the repair. are designed to grasp and hold gauze side of the tray is a practice occasionally Tissue Forcep Dressing Forcep and dressing during a surgical procedure. used in the OR to organize and quickly pass the forcep to the sterile field. -

Paper No. 1 UNITED STATES PATENT and TRADEMARK OFFICE
Paper No. 1 UNITED STATES PATENT AND TRADEMARK OFFICE _______________ BEFORE THE PATENT TRIAL AND APPEAL BOARD _____________ AURIS HEALTH, INC. Petitioner, v. INTUITIVE SURGICAL OPERATIONS, INC. Patent Owner. Patent No. 6,491,701 _______________ Inter Partes Review No. IPR2019-01532 ____________________________________________________________ Petition for Inter Partes Review of U.S. Patent No. 6,491,701 IPR2019-01532 TABLE OF CONTENTS I. INTRODUCTION ............................................................................................1 II. REGULATORY INFORMATION ................................................................ 2 A. CERTIFICATION PETITIONER MAY CONTEST THE ’701 PATENT (§ 42.104(A)) 2 B. IDENTIFICATION OF CHALLENGED CLAIMS (§ 42.104(B)) ............................... 3 C. FEE FOR INTER PARTES REVIEW (§ 42.15(A)) .................................................. 3 III. BACKGROUND ..........................................................................................3 A. BACKGROUND TECHNOLOGY ..........................................................................3 B. SUMMARY OF THE ’701 PATENT ......................................................................5 C. SUMMARY OF THE ’701 PATENT’S PROSECUTION HISTORY ............................ 8 D. PERSON OF ORDINARY SKILL IN THE ART ....................................................... 9 IV. CLAIM CONSTRUCTION ......................................................................10 A. “END EFFECTOR” (ALL CHALLENGED CLAIMS) .............................................11 -
Instrument Measuring: Why Precise Descriptions Are Necessary When Completing Count Sheets
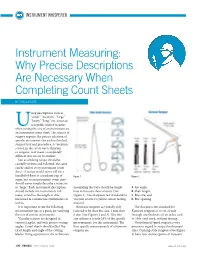
INSTRUMENT WHISPERER Instrument Measuring: Why Precise Descriptions Are Necessary When Completing Count Sheets BY RICK SCHULTZ sing descriptions such as “small,” “medium,” “large,” “heavy,” “long,” etc. is not an acceptable unit of measure Uwhen noting the size of an instrument on an instrument count sheet. The science of surgery requires the precise selection of specific instruments for each individual, surgical tray and procedure. A “medium” scissor, in the eye of one technician or surgeon, may mean a completely different size scissor to another. Just as a baking recipe should be carefully written and followed, the same can be said of every instrument count sheet. A recipe would never call for a handful of flour or a medium cup of Figure 1 Figure 2 sugar, just as an instrument count sheet should never simply describe a retractor as “large.” Each instrument description assembling the trays should be taught A. Jaw angle; should include the instrument’s full how to measure these scissors (See B. Shaft length; name, as well as the length or size, Figure 1). The sharpness test standard for C. Bite size; and measured in centimeteres/millimeters or vascular scissors is yellow scissor testing D. Bite opening inches. material. It is important to use the following Kerrison rongeurs are usually only The sharpness test standard for measurement tips as a guide for verifying referred to by their bite size, 1 mm thru Kerrison rongeurs is to cut cleanly the size of certain instruments. 6 mm (See Figures 2 and 3). This bite through one thickness of an index card Vascular scissors are designed in size reference is only 25% of the specific or 100# card stock, without tearing. -

Precision Surgical Instruments 2016 Catalog
WORLD PRECISION INSTRUMENTS ΖQVWUXPHQWLQJVFLHQWLȴFLGHDV Precision Surgical Instruments 2016 Catalog www.wpiinc.com Let WPI fill all your lab needs: syringe pumps micromanipulators capillary glass blood pressure monitors microinjection laboratory glassware anesthesia analgesia respirators temperature controls You’ll find all this and more in WPI’s 208-page Laboratory Equipment catalog. Call for your copy today — or request one online at www.wpiinc.com Re-stocking your lab glassware? WPI can save you hundreds of dollar$! Request a Top glassware catalog today! Quality Borosilicate Glass Surgical Instruments Scissors Veterinary Instruments Spring Scissors . 2. Dental Instruments . 74 Titanium Spring Scissors . .6 Periodontal Basic Set-up . 77 Ring Scissors . 9. Micro Scissors . 19 Extraction Basic Set-up . 77 Round Handled Spring Scissors . 19 Surgical Packs . 78 Catheters . 81 Forceps & Tweezers WPI Swiss Tweezers . 20 Electrosurgery Dumont Forceps . 22 Ceramic-Tipped, Delrin-Tipped . 27 Disposable Cautery Units . 82 Round Handled Forceps . 34 Thermal Cautery Unit . 83 Towel Clamps . 38 High Frequency Dessicator . 84 Hemostatic . 38 Economy Electrosurgical Unit . 85 Titanium Forceps . 36 OmniDrill35 Micro Drill System . 85 Needle Holders Animal Handling and Support Spring Handles . 41 Ring Handles . 43 Small Animal Anesthesia . 86 Titanium . 45 Animal Temperature Control . 88 Blood Pressure Monitor & Transducer . 89 Sutures and Clamps Syringe Pumps . 90 Surgical Needles . 46 Manual Microsyringe Pumps . 91 Skin Staplers . 47 MiniStar Miniature Peristalic Pump . 91 Clips and Clamps . 48 NanoFil™ Sub-microliter Injection System . 92 UltraMicroPump III . 95 Retractors Spring . 50 Optics Self-Retaining . 51 Binocular Loupes . 96 Knives Precision SurgioScope . 98 Sapphire Knives . 53 Scalpels and Blades . 54 Instrument Care Ear Tags, Biopsy Punches . -
Valve Instrumentation
The Finest Surgical VALVE INSTRUMENTATION CONVENTIONAL • VALVE REPLACEMENT • PLACEMENT OF ANNULOPLASTY RING • ADVANCED VALVE REPAIR Valve Instrumentation Valve Instrumentation SCISSORS We are pleased to introduce the new Scanlan Valve Instrument brochure, a collection of new and existing instrument designs that are frequently used in VALVE REPLACEMENT or conventional approach cardiac valve procedures. PLACEMENT OF ANNULOPLASTY RING ADVANCED REPAIR ACCESSORIES SCISSORS NEEDLE HOLDERS If you need additional instrument design options, the Scanlan catalog or our website (scanlaninternational.com) offers an extensive selection of additional SCISSORS SCISSORS – Fine MEMORY INSTRUMENTS instrument designs. Thompson Valve Scissors. .4 Metzenbaum Scissors - Fine Tip . 14 Mirror Instrument. .24 Metzenbaum Scissors. 5 Lillehei-Potts Scissors. .14 Hook Instrument . .24 Even with our extensive design options, we understand the need to Mayo Harrington Scissors. .5 Metzenbaum Scissors - Tenotomy Tip. 15 Knife Handle. 24 accommodate changing technology and unique surgical procedures. To Stevens Tenotomy Scissors . 15 Garrett Vascular Dilators / Vessel Probes. .25 support this, Scanlan International provides customers with in-house design NEEDLE HOLDERS for 2-0, 3-0, 4-0 suture Knife Blade Attachment / Removal Instrument. 26 NEEDLE HOLDERS FORCEPS and instrument modification services – where our experienced artisans can Stratte Needle Holders. .6 NEEDLE HOLDERS for 5-0 and 6-0 suture – Fine customize each instrument to your specifications. Fell Needle Holders. .7 Micro Needle Holders, Ryder Style. 16-17 SCANLAN CALIPER. 27 Heavy Style Needle Holders. .8 Jacobson Micro Needle Holders. 18-19 Since 1921, our family has dedicated itself to providing the highest quality Mayo-Hegar Needle Holders. 9 LEGACY DeBakey Needle Holders. .19 CLAMPS FORCEPS surgical instrumentation and fast, friendly service to all of our customers. -
Tissue & Artery Forceps
Tissue & Artery Forceps Zepf Tissue Forceps have Zepf Artery Forceps are carefully rounded and uniform points. designed for easy handling in all operating situations, giving surgeons perfect control. The teeth have great durability and The points are carefully rounded and sharpness for ease of grasp and release. uniform. The jaw serrations mesh exactly when instrument is closed and edges are This well-balanced instrument has serrated beveled to protect tissue. Rachets are handles for a firm grip and well adjusted undercut, ensuring safe ease of locking springs for the perfect amount of tension. and unlocking. Page 4 Zepf Tungsten Carbide Forceps 32-5624 SEMKEN DRESSING FORCEPS 5” 13CM 32-5624-15 DRESSING FORCEPS-SEMKEN 1x2 TEETH 6” 15CM 32-5500 ZEPF DRESSING FORCEPS 5” 12.5CM T/C JAWS 32-5631 SEMKEN TISSUE FORCEPS 5” 13CM 1x2 TEETH 32-5504 ZEPF DRESSING FORCEPS 6.25” 16 T/C JAWS 32-5631-15 TISSUE FORCEPS-SEMKEN 1X2 TEETH 6” 15CM 32-5508 ZEPF DRESSING FORCEPS 7” 18CM T/C JAWS 32-5633 LUCAE TISSUE FORCEPS-SEPARATED 5.5” 14CM 32-5512 ZEPF DRESSING FORCEPS 8” 20CM T/C JAWS 32-5635-18 NEVINS TISSUE FORCEPS 7” 18CM 1x2 TEETH 32-5516 ZEPF DRESSING FORCEPS 10” 25CM T/C JAWS 32-5635-23 NEVINS TISSUE FORCEPS 9” 23CM 1x2 TEETH 32-5520 ADSON DRESSING FORCEPS 4.75” 12CM T/C JAWS 32-5640-18 POTTS-NEVINS DRESSING FORCEPS 7” 18CM 32-5524 POTTS-SMITH DRESSING FORCEPS 7” 18CM T/C JAWS 32-5640-23 POTTS-NEVINS DRESSING FORCEPS 9” 23CM 32-5532 GRUENWALD DRESSING FORCEPS 8.5” 21.5CM T/C JAWS 32-5644 GERALD DRESSING FORCEPS 7” 18CM 32-5536 TAYLOR-CUSHING DRESSING -

Teleflex Incorporated
Surgical Instruments Catalog Home // CVT CVT 341503 : LEMOLE-PILLING® VALVE RETRACTOR - Set #3 Fits Ankeney Retractor Provides self-retaining valve retraction. Fits directly onto arms of many types of sternal retractors. The T-Frame cross bar attaches to the sternal retractor by means of a “C” clamp. 8" (20.3 cm) T-Frame cross bar allows... 351814 : DEBAKEY TISSUE FORCEPS Angled, 2mm tip, 9 1/2" (24 cm) 341515 : Lemole Side Arm Extension For Cooley And Chaux Retractors For third point atrial retraction during mitral valve surgery, fits Cooley-style and Chaux Retractors. Related: 341150 Chaux Multipurpose Sternal IMA Retractor 341155 Chaux Sternal/IMA Valve Retractor Set 341194,... 351755 : Blanco Valve Retractor 9mm width x 1/2" (1.0cm) depth blade, 11 1/2" (29.0cm) 342606 : MIXER FORCEPS Strongly Curved, Serrated (3cm) tip length, 10 3/4" (27.5cm) 152827 : MICRO SURGERY NEEDLE HOLDER Curved, Flat handle, With lock, 12.8 x 1.4mm smooth jaw, 6" (14.5cm), TC 342166 : DeBakey-Metzenbaum Scissors Curved, 9 1/8" (23.0cm), TC 353040 : SCHWARTZ CLAMP HOLDING FORCEPS Angled, 7 1/2" (19 cm) 342725 : BABCOCK TISSUE FORCEPS Serrated, 9 1/2" (24 cm) 352295 : Satinsky Scissors Curved, 9 3/4" (25.0cm) 506748 : MEDIASTINAL BLUNT TIPPED DISSECTING FORCEPS Serrated, 16 mm tip, 12" (31 cm), working length 7-1/2" (19 cm) 359048 : GERALD TITANIUM TISSUE FORCEPS Serrated, 6 7/8" (18 cm) 343027 : STRATTE NEEDLE HOLDER Reverse curved, 9" (23cm), TC 354908 : MATCHED SET OF FOUR DEBAKEY NEEDLE HOLDERS Consists of 354900, 354902, 354904, 354906 357675 : Micro Vascular Round Handle Needle Holder Smooth, stainless steel jaws, round handles.