Respiratory Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

OM-85) on Frequency of Upper Respiratory Tract Infections and Size of Adenoid Tissue in Preschool Children with Adenoid Hypertrophy
STUDY PROTOCOL Effect of Vaxoral® (OM-85) on frequency of upper respiratory tract infections and size of adenoid tissue in preschool children with adenoid hypertrophy Study Product(s) Vaxoral® (OM-85) Indication Recurrent RTIs, adenoid hypertrophy Sponsor Dr Sami Ulus Maternity and Children Research and Training Hospital, Department of Pediatric Allergy and Immunology, Ankara, TURKEY Anticipated Turkey Countries Introduction OM-85 significantly reduces RTIs in children. This effect was proved by many clinical studies and meta-analyses1. A Cochrane meta-analysis first published in 2006 and updated recently (Del- Rio-Navarro 2012) showed that immunostimulants (IS) could reduce acute RTIs (ARTIs) by almost 39% when compared to placebo. Among the different IS, OM-85 showed the most robust evidence with 4 trials of “A quality” according to the Cochrane grading criteria. Pooling six OM-85 studies, the Cochrane review reported a mean number of ARTIs reduction by -1.20 [95% CI: - 1.75, -0.66] and a percentage difference in ARTIs by -35.9% [95% CI: -49.46, -22.35] compared to placebo1. Adenoid hypertrophy (AH) is one of the most important respiratory disease in preschool children2. In normal conditions adenoid tissue enlarges up to 5 years and become smaller afterwards. But in some children who have recurrent URTIs, it keeps growing and this can be associated with complications2. AH may cause recurrent respiratory infections and each infection contributes to enlargement of adenoid tissue thus promoting a vicious cycle. Additionally enlarged adenoids are known to be reservoir for microbes and cause of recurrent or long lasting RTIs3. AH is associated with chronic cough, recurrent and chronic sinusitis, recurrent tonsillitis, recurrent otitis media with effusion, recurrent other respiratory problems such as, nasal obstruction and sleep disturbances, sleep apneas2-3. -

Pleural Effusion and Ventilation/Perfusion Scan Interpretation for Acute Pulmonary Embolus
ventricular function by radionuclide angiography during exercise in normal subjects 33. Verani MS. Myocardial perfusion imaging versus two-dimensional echocardiography: and patients with chronic coronary heart disease. J Am Coll Cardiol 1983;1:1518- comparative value in the diagnosis of coronary artery disease. J NucÃCardiol 1529. 1994;1:399-414. 29. Adam WE. Tarkowska A, Bitter F, Stauch M, Geffers H. Equilibrium (gated) 34. Foster T, McNeill AJ, Salustri A, et al. Simultaneous dobutamine stress echocardiog radionuclide ventriculography. Cardiovasc Radial 1979;2:161-173. raphy and technetium-99m SPECT in patients with suspected coronary artery disease. 30. Hurwitz RA, TrêvesS, Kuroc A. Right ventricular and left ventricular ejection fraction J Am Coll Cardiol I993;21:1591-I596. in pediatrie patients with normal hearts: first pass radionuclide angiography. Am 35. Marwick TH, D'Hondt AM, Mairesse GH, Baudhuin T, Wijins W, Detry JM, Meiin Heart J 1984;107:726-732. 31. Freeman ML, Palac R, Mason J, et al. A comparison of dobutamine infusion and JA. Comparative ability of dobutamine and exercise stress in inducing myocardial ischemia in active patients. Br Heart J 1994:72:31-38. supine bicycle exercise for radionuclide cardiac stress testing. Clin NucÃMed 1984:9:251-255. 36. Senior R, Sridhara BS, Anagnostou E, Handler C, Raftery EB, Lahiri A. Synergistic 32. Cohen JL, Greene TO, Ottenweller J, Binebaum SZ, Wilchfort SD, Kim CS. value of simultaneous stress dobutamine sestamibi single-photon-emission computer Dobutamine digital echocardiography for detecting coronary artery disease. Am J ized tomography and echocardiography in the detection of coronary artery disease. -

Diagnosing Pulmonary Embolism M Riedel
309 Postgrad Med J: first published as 10.1136/pgmj.2003.007955 on 10 June 2004. Downloaded from REVIEW Diagnosing pulmonary embolism M Riedel ............................................................................................................................... Postgrad Med J 2004;80:309–319. doi: 10.1136/pgmj.2003.007955 Objective testing for pulmonary embolism is necessary, embolism have a low long term risk of subse- quent VTE.2 5–7 because clinical assessment alone is unreliable and the consequences of misdiagnosis are serious. No single test RISK FACTORS AND RISK has ideal properties (100% sensitivity and specificity, no STRATIFICATION risk, low cost). Pulmonary angiography is regarded as the The factors predisposing to VTE broadly fit Virchow’s triad of venous stasis, injury to the final arbiter but is ill suited for diagnosing a disease vein wall, and enhanced coagulability of the present in only a third of patients in whom it is suspected. blood (box 1). The identification of risk factors Some tests are good for confirmation and some for aids clinical diagnosis of VTE and guides decisions about repeat testing in borderline exclusion of embolism; others are able to do both but are cases. Primary ‘‘thrombophilic’’ abnormalities often non-diagnostic. For optimal efficiency, choice of the need to interact with acquired risk factors before initial test should be guided by clinical assessment of the thrombosis occurs; they are usually discovered after the thromboembolic event. Therefore, the likelihood of embolism and by patient characteristics that risk of VTE is best assessed by recognising the may influence test accuracy. Standardised clinical presence of known ‘‘clinical’’ risk factors. estimates can be used to give a pre-test probability to However, investigations for thrombophilic dis- orders at follow up should be considered in those assess, after appropriate objective testing, the post-test without another apparent explanation. -
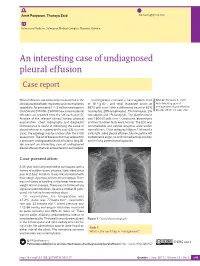
An Interesting Case of Undiagnosed Pleural Effusion Case Report
Amit Panjwani, Thuraya Zaid [email protected] Pulmonary Medicine, Salmaniya Medical Complex, Manama, Bahrain. An interesting case of undiagnosed pleural effusion Case report Pleural effusions are commonly encountered in the Investigations revealed a haemoglobin level Cite as: Panjwani A, Zaid T. clinical practise of both respiratory and nonrespiratory of 16.4 g⋅dL−1, and total leukocyte count of An interesting case of specialists. An estimated 1–1.5 million new cases in 8870 cells⋅mm−3 with a differential count of 62% undiagnosed pleural effusion. the USA and 200 000–250 000 new cases of pleural neutrophils, 28% lymphocytes, 7% monocytes, 2% Breathe 2017; 13: e46–e52. effusions are reported from the UK each year [1]. eosinophils and 1% basophils. The platelet count Analysis of the relevant clinical history, physical was 160 000 cells⋅mm−3. Creatinine, electrolytes examination, chest radiography and diagnostic and liver function tests were normal. The ECG was thoracentesis is useful in identifying the cause of unremarkable and cardiac enzymes were within pleural effusion in majority of the cases [2]. In a few normal limits. Chest radiograph (figure 1) showed a cases, the aetiology may be unclear after the initial mild, right-sided pleural effusion, blunting of the left assessment. The list of diseases that may account for costophrenic angle, no shift of mediastinal position a persistent undiagnosed pleural effusion is long [3]. and no lung parenchymal opacities. We present an interesting case of undiagnosed pleural effusion that was encountered in our hospital. R Case presentation A 33-year-old male presented to our hospital with a history of sudden-onset, pleuritic, right-sided chest pain of 2 days’ duration. -

Diagnosis of Chronic Thromboembolic Pulmonary Hypertension After Acute Pulmonary Embolism
Early View Review Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism Fredrikus A. Klok, Francis Couturaud, Marion Delcroix, Marc Humbert Please cite this article as: Klok FA, Couturaud F, Delcroix M, et al. Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism. Eur Respir J 2020; in press (https://doi.org/10.1183/13993003.00189-2020). This manuscript has recently been accepted for publication in the European Respiratory Journal. It is published here in its accepted form prior to copyediting and typesetting by our production team. After these production processes are complete and the authors have approved the resulting proofs, the article will move to the latest issue of the ERJ online. Copyright ©ERS 2020 Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism Fredrikus A. Klok, Francis Couturaud F2, Marion Delcroix M3, Marc Humbert4-6 1 Department of Thrombosis and Hemostasis, Leiden University Medical Center, Leiden, The Netherlands 2 Département de Médecine Interne et Pneumologie, Centre Hospitalo-Universitaire de Brest, Univ Brest, EA 3878, CIC INSERM1412, Brest, France 3 Department of Respiratory Diseases, University Hospitals and Respiratory Division, Department of Chronic Diseases, Metabolism & Aging, KU Leuven – University of Leuven, Leuven, Belgium 4 Université Paris-Saclay, Faculté de Médecine, Le Kremlin-Bicêtre, France 5 Service de Pneumologie et Soins Intensifs Respiratoires, Hôpital Bicêtre, AP-HP, Le Kremlin-Bicêtre, France 6 INSERM UMR S 999, Hôpital Marie Lannelongue, Le Plessis Robinson, France Corresponding author: Frederikus A. Klok, MD, FESC; Department of Thrombosis and Hemostasis, Leiden University Medical Center, Leiden, the Netherlands; Albinusdreef 2, 2300RC, Leiden, the Netherlands; Phone: +31- 715269111; E-mail: [email protected] Abstract Chronic thromboembolic pulmonary hypertension (CTEPH) is the most severe long-term complication of acute pulmonary embolism (PE). -

Clinical Study Microbiological Profile of Adenoid Hypertrophy Correlates to Clinical Diagnosis in Children
Hindawi Publishing Corporation BioMed Research International Volume 2013, Article ID 629607, 10 pages http://dx.doi.org/10.1155/2013/629607 Clinical Study Microbiological Profile of Adenoid Hypertrophy Correlates to Clinical Diagnosis in Children Anita Szalmás,1 Zoltán Papp,2 Péter Csomor,2 József Kónya,1 István Sziklai,2 Zoltán Szekanecz,3 and Tamás Karosi2 1 Department of Medical Microbiology, Medical and Health Science Center, University of Debrecen, Nagyerdei Krt. 98, Debrecen 4032, Hungary 2 Department of Otolaryngology and Head and Neck Surgery, Medical and Health Science Center, University of Debrecen, Nagyerdei Krt. 98, Debrecen 4032, Hungary 3 Department of Rheumatology, Medical and Health Science Center, University of Debrecen, Nagyerdei Krt. 98, Debrecen 4032, Hungary Correspondence should be addressed to Tamas´ Karosi; [email protected] Received 24 April 2013; Accepted 23 August 2013 Academic Editor: Ralph Mosges¨ Copyright © 2013 Anita Szalmas´ et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Objective. Adenoid hypertrophy is a common condition in childhood, which may be associated with recurring acute otitis media (RAOM), otitis media with effusion (OME), and obstructive sleeppnea a syndrome (OSAS). These different clinical characteristics have some clinical overlap; however, they might be explained by distinct immunologic and infectious profiles and result in various histopathologic findings of adenoid specimens. Methods. A total of 59 children with adenoid hypertrophy undergoing adenoidectomy were studied. Three series of identical adenoid specimens were processed to hematoxylin-eosin (H.E.) and Gram staining and to respiratory virus specific real-time PCR, respectively. -

Acute Pulmonary Embolism in Patients with and Without COVID-19
Journal of Clinical Medicine Article Acute Pulmonary Embolism in Patients with and without COVID-19 Antonin Trimaille 1,2 , Anaïs Curtiaud 1, Kensuke Matsushita 1,2 , Benjamin Marchandot 1 , Jean-Jacques Von Hunolstein 1 , Chisato Sato 1,2, Ian Leonard-Lorant 3, Laurent Sattler 4 , Lelia Grunebaum 4, Mickaël Ohana 3 , Patrick Ohlmann 1 , Laurence Jesel 1,2 and Olivier Morel 1,2,* 1 Division of Cardiovascular Medicine, Nouvel Hôpital Civil, Strasbourg University Hospital, 67000 Strasbourg, France; [email protected] (A.T.); [email protected] (A.C.); [email protected] (K.M.); [email protected] (B.M.); [email protected] (J.-J.V.H.); [email protected] (C.S.); [email protected] (P.O.); [email protected] (L.J.) 2 INSERM (French National Institute of Health and Medical Research), UMR 1260, Regenerative Nanomedicine, FMTS, 67000 Strasbourg, France 3 Radiology Department, Nouvel Hôpital Civil, Strasbourg University Hospital, 67000 Strasbourg, France; [email protected] (I.L.-L.); [email protected] (M.O.) 4 Haematology and Haemostasis Laboratory, Centre for Thrombosis and Haemostasis, Nouvel Hôpital Civil, Strasbourg University Hospital, 67000 Strasbourg, France; [email protected] (L.S.); [email protected] (L.G.) * Correspondence: [email protected] Abstract: Introduction. Acute pulmonary embolism (APE) is a frequent condition in patients with Citation: Trimaille, A.; Curtiaud, A.; COVID-19 and is associated with worse outcomes. Previous studies suggested an immunothrombosis Matsushita, K.; Marchandot, B.; instead of a thrombus embolism, but the precise mechanisms remain unknown. -

Mediastinum and Subcutaneous Emphysema: a Rare Complication of a Common Procedure
Case Report Brunei Int Med J. 2017; 13 (1): 29-32 Post adenotonsillectomy pneumo- mediastinum and subcutaneous emphysema: A rare complication of a common procedure. Farah Wahida ABD MANAB1,2, Nor Shahida ABDUL MUTALLIB1, Hisham ABDUL RAH- MAN1, Hamidah MAMAT1 1Department of otorhinolaryngology-Head and Neck surgery, Hospital Sultan Abdul Halim, Kedah, Malaysia, 2Department of Otorhinolaryngology, Head and Neck Surgery, School of Medical Sciences, Universiti Sains Malaysia, Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia ABSTRACT Cervicofacial and pneumomediastinum subcutaneous emphysema is a very rare complication of adenotonsillectomy procedure. Even though it is a self limiting complication and can be treated conservatively, it can alarming for the patient or patient’s family as well as leading to more seri- ous and fatal consequences occurring from tension pneumomediastinum. We report a case of incidental finding of pneumomediastinum in postadenotonsillectomy patient. He was managed conservatively and made an uneventful recovery. Keywords: tonsillectomy, subcutaneous emphysema, complication INTRODUCTION Case Report Adenotonsillectomy is a common surgical pro- A 12 year old boy was admitted to our Ear, cedure among paediatric age group. It is rela- Nose and Throat (ENT) ward for elective sur- tively a safe procedure with minimal compli- gery of adenotonsillectomy. The indication for cations. Common complications are intraoper- surgery was recurrent attacks of acute tonsil- ative or postoperative haemorrhage, infec- litis. He had underlying Allergic Rhinitis and tion, damaged to soft tissue and surrounding Bronchial Asthma. structure such as teeth, odynophagia and oropharyngeal edema.1 Cervicofacial and Patient was given general anaesthesia with pneumomediastinum subcutaneous emphyse- fentanyl, propofol and cisatracium during in- ma is a very rare complication. -

COVID-19 Associated Pulmonary Embolism in Pediatric Patients
Prepublication Release A N O F F I C I A L J O U R N A L O F T H E A M E R I C A N A C A D E M Y O F P E D I A T R I C S COVID-19 Associated Pulmonary Embolism in Pediatric Patients Melissa Chima, Duane Williams, Neal J. Thomas, Conrad Krawiec DOI: 10.1542/hpeds.2021-005866 Journal: Hospital Pediatrics Article Type: Original Article Citation: Chima M, et al. COVID-19 Associated Pulmonary Embolism in Pediatric Patients. Hosp Pediatr. 2021; doi: 10.1542/hpeds.2021-005866 This is a prepublication version of an article that has undergone peer review and been accepted for publication but is not the final version of record. This paper may be cited using the DOI and date of access. This paper may contain information that has errors in facts, figures, and statements, and will be corrected in the final published version. The journal is providing an early version of this article to expedite access to this information. The American Academy of Pediatrics, the editors, and authors are not responsible for inaccurate information and data described in this version. Downloaded©202 from1 www.aappublications.org/news American Academy byof guest Pediatrics on October 1, 2021 Prepublication Release COVID-19 Associated Pulmonary Embolism in Pediatric Patients Melissa Chima, BS1, Duane Williams, MD2, Neal J. Thomas, MD2,3, Conrad Krawiec, MD2 Authors’ Affiliations and Addresses: 1Penn State College of Medicine, 500 University Drive, P.O. Box 850, Hershey, PA, USA 17033-0850, Tel: (717)-531-5337, Fax: (717)-531-8985. -

Pulmonary Embolism Or Pneumocystis Jiroveci Pneumonia?
breathe case presentations.qxd 26/07/2006 12:03 Page 5 CASE PRESENTATION Pulmonary embolism or Pneumocystis jiroveci pneumonia? Case report Table 1 Vital signs and F. Braiteh1,2 A 33-year-old male presented to the emergency laboratory test results at I. Nash3 department with a 5-day history of exertional dys- presentation pnoea, dry cough, lethargy and an ongoing fever of 38.9°C. He had been previously diagnosed Investigation Result Normal 1Medical Oncology, Division of with left-frontal oligodendroglioma during a range Cancer Medicine, The University work-up following a new-onset seizure 4 months Vital signs of Texas M.D. Anderson Cancer Temperature °C 36.6 earlier. After successful tumour resection and Center, 2University of Texas Respiratory rate cycles·min-1 22 adjuvant radiotherapy, the patient totally recov- Graduate School of Biomedical Heart rate beats·min-1 88 ered without any residual paresis. He was main- Sciences, Houston, TX, and Blood pressure mmHg 126/64 3Dept of Pathology, Hospital of tained on valproic acid and dexamethasone at a O2 saturation % 91 Saint Raphael, Yale School of -1 dose that was tapered down to 2 mg·day . Haematological counts and coagulation Medicine, New Haven, CT, USA. The physical examination was unremarkable. White cells ×109·L -1 6.8 4.0–10.0 The patient was haemodynamically stable but Platelets ×109·L -1 123 150–350 hypoxaemic and anaemic (table 1). Chest radio- Haemoglobin g·dL-1 9.3 12.0–16.0 Correspondence: graphy and computed tomography (CT) were Prothrombine time s 12.8 <13.0 F. -

Pulmonary Embolism (Pe): Diagnosis
PULMONARY EMBOLISM (PE): DIAGNOSIS OBJECTIVE: To provide a diagnostic approach to patients with suspected acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE), which comprises deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common disease, affecting approximately 1-2 in 1,000 adults per year. The diagnosis of PE has increased significantly since the advent of computed tomography pulmonary angiography (CTPA) with its widespread availability and enhanced sensitivity. The majority of PE originates in the proximal deep veins of the leg, despite the observation that only 25-50% of patients with PE have clinically evident DVT at the time of PE diagnosis. While active malignancy, surgery (especially orthopedic), hospitalization, air travel >8 hours, and hormone use/pregnancy are common transient provoking factors, approximately 50% of first-time PEs appear to be unprovoked. Symptoms of PE may include sudden onset dyspnea, pleuritic chest pain, and syncope. Signs of PE may include tachypnea, tachycardia, hypoxemia, hypotension, and features of right ventricular dysfunction (distended jugular veins). There may be accompanying signs and symptoms of DVT. The ECG may show right ventricular strain (S1Q3T3, right bundle branch block and T-inversion in leads V1- V4). Up to 10% of symptomatic PEs are fatal within the first hour of symptom onset. Independent predictors of mortality within the first few days after diagnosis of PE include hypotension (systolic blood pressure [SBP] <90 mmHg), clinical right heart failure, right ventricular dilatation on CTPA/echocardiography, positive troponin, and elevated brain natriuretic peptide (BNP). Early diagnosis and treatment of PE reduces morbidity and mortality. DIAGNOSIS OF PE: The constellation of symptoms and signs may be suggestive of PE but do not alone have the sensitivity or specificity to rule in or rule out the diagnosis. -

Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE)
How can it be prevented? You can take steps to prevent deep vein thrombosis (DVT) and pulmonary embolism (PE). If you're at risk for these conditions: • See your doctor for regular checkups. • Take all medicines as your doctor prescribes. • Get out of bed and move around as soon as possible after surgery or illness (as your doctor recommends). Moving around lowers your chance of developing a blood clot. References: • Exercise your lower leg muscles during Deep Vein Thrombosis: MedlinePlus. (n.d.). long trips. Walking helps prevent blood Retrieved October 18, 2016, from clots from forming. https://medlineplus.gov/deepveinthrombos is.html If you've had DVT or PE before, you can help prevent future blood clots. Follow the steps What Are the Signs and Symptoms of Deep above and: Vein Thrombosis? - NHLBI, NIH. (n.d.). Retrieved October 18, 2016, from • Take all medicines that your doctor http://www.nhlbi.nih.gov/health/health- prescribes to prevent or treat blood clots topics/topics/dvt/signs • Follow up with your doctor for tests and treatment Who Is at Risk for Deep Vein Thrombosis? - • Use compression stockings as your DEEP NHLBI, NIH. (n.d.). Retrieved October 18, doctor directs to prevent leg swelling 2016, from http://www.nhlbi.nih.gov/health/health- VEIN topics/topics/dvt/atrisk THROMBOSIS How Can Deep Vein Thrombosis Be Prevented? - NHLBI, NIH. (n.d.). Retrieved October 18, 2016, from (DVT) http://www.nhlbi.nih.gov/health/health- topics/topics/dvt/prevention How Is Deep Vein Thrombosis Treated? - NHLBI, NIH. (n.d.). Retrieved October 18, 2016, from http://www.nhlbi.nih.gov/health/health- topics/topics/dvt/treatment Trinity Surgery Center What is deep vein Who is at risk? What are the thrombosis (DVT)? The risk factors for deep vein thrombosis symptoms? (DVT) include: Only about half of the people who have DVT A blood clot that forms in a vein deep in the • A history of DVT.