Drivers of Malnutrition in Niger: Analysis of Secondary Data Sources
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Niger Country Strategic Plan (2020–2024)
Executive Board Second regular session Rome, 18–21 November 2019 Distribution: General Agenda item 7 Date: 25 October 2019 WFP/EB.2/2019/7-A/6 Original: English Operational matters – Country strategic plans For approval Executive Board documents are available on WFP’s website (https://executiveboard.wfp.org). Niger country strategic plan (2020–2024) Duration 1 January 2020–31 December 2024 Total cost to WFP USD 1,055,624,308 Gender and age marker* 3 * https://gender.manuals.wfp.org/en/gender-toolkit/gender-in-programming/gender-and-age-marker/. Executive summary The Niger is a food-deficit, land-locked least developed country ranked last in the 2018 Human Development Index. High levels of food insecurity and malnutrition are exacerbated by environmental degradation, poor natural resource management, rapid population growth, pervasive gender inequalities and climate shocks. Increasing insecurity and the spill over of conflicts induced by non-state groups from neighbouring countries compound these challenges, resulting in forced population displacements. This country strategic plan focuses on supporting government emergency response while implementing integrated resilience activities to protect livelihoods and foster long-term recovery. WFP also aims to strengthen national capacities in order to ensure the sustainability and ownership of zero hunger solutions, for example through measures to make the national social protection system more shock-adaptive and gender-responsive. The plan contains a multisectoral and integrated nutrition package, through which nutrition treatment and inclusive community-led nutrition-sensitive approaches will be aimed at strengthening local food production, promoting girls’ education and improving health and sanitation. The country strategic plan will be gender-equitable and will incorporate gender-transformative approaches to achieving zero hunger, including through the economic and social empowerment of women. -

NIGER: Carte Administrative NIGER - Carte Administrative
NIGER - Carte Administrative NIGER: Carte administrative Awbari (Ubari) Madrusah Légende DJANET Tajarhi /" Capital Illizi Murzuq L I B Y E !. Chef lieu de région ! Chef lieu de département Frontières Route Principale Adrar Route secondaire A L G É R I E Fleuve Niger Tamanghasset Lit du lac Tchad Régions Agadez Timbuktu Borkou-Ennedi-Tibesti Diffa BARDAI-ZOUGRA(MIL) Dosso Maradi Niamey ZOUAR TESSALIT Tahoua Assamaka Tillabery Zinder IN GUEZZAM Kidal IFEROUANE DIRKOU ARLIT ! BILMA ! Timbuktu KIDAL GOUGARAM FACHI DANNAT TIMIA M A L I 0 100 200 300 kms TABELOT TCHIROZERINE N I G E R ! Map Doc Name: AGADEZ OCHA_SitMap_Niger !. GLIDE Number: 16032013 TASSARA INGALL Creation Date: 31 Août 2013 Projection/Datum: GCS/WGS 84 Gao Web Resources: www.unocha..org/niger GAO Nominal Scale at A3 paper size: 1: 5 000 000 TILLIA TCHINTABARADEN MENAKA ! Map data source(s): Timbuktu TAMAYA RENACOM, ARC, OCHA Niger ADARBISNAT ABALAK Disclaimers: KAOU ! TENIHIYA The designations employed and the presentation of material AKOUBOUNOU N'GOURTI I T C H A D on this map do not imply the expression of any opinion BERMO INATES TAKANAMATAFFALABARMOU TASKER whatsoever on the part of the Secretariat of the United Nations BANIBANGOU AZEY GADABEDJI TANOUT concerning the legal status of any country, territory, city or area ABALA MAIDAGI TAHOUA Mopti ! or of its authorities, or concerning the delimitation of its YATAKALA SANAM TEBARAM !. Kanem WANZERBE AYOROU BAMBAYE KEITA MANGAIZE KALFO!U AZAGORGOULA TAMBAO DOLBEL BAGAROUA TABOTAKI TARKA BANKILARE DESSA DAKORO TAGRISS OLLELEWA -

World Bank Document
The World Bank Report No: ISR12228 Implementation Status & Results Niger Transport Sector Program Support Project (P101434) Operation Name: Transport Sector Program Support Project (P101434) Project Stage: Implementation Seq.No: 11 Status: ARCHIVED Archive Date: 26-Nov-2013 Country: Niger Approval FY: 2008 Public Disclosure Authorized Product Line:IBRD/IDA Region: AFRICA Lending Instrument: Sector Investment and Maintenance Loan Implementing Agency(ies): Key Dates Board Approval Date 29-Apr-2008 Original Closing Date 15-Dec-2012 Planned Mid Term Review Date 14-Feb-2011 Last Archived ISR Date 24-Apr-2013 Public Disclosure Copy Effectiveness Date 10-Sep-2008 Revised Closing Date 15-Dec-2015 Actual Mid Term Review Date 28-Jan-2011 Project Development Objectives Project Development Objective (from Project Appraisal Document) The project development objectives are to (i) improve the physical access of rural population to markets and services on selected unpaved sections of the national road network, and (ii) strengthen the institutional framework, management and implementation of roadmaintenance in Niger. Has the Project Development Objective been changed since Board Approval of the Project? Yes No Public Disclosure Authorized Component(s) Component Name Component Cost 1. Periodic maintenance and spot rehabilitation of unpaved roads; 24.89 2. Institutional support to main transport sector players 2. Institutional support to the main transport sector players 5.11 Overall Ratings Previous Rating Current Rating Progress towards achievement of PDO Satisfactory Moderately Satisfactory Overall Implementation Progress (IP) Satisfactory Moderately Satisfactory Overall Risk Rating Moderate Moderate Public Disclosure Authorized Implementation Status Overview As of October 31, 2013, the Grant amount for the original project has reached a disbursement rate of about 100 percent. -
Caught in the Middle a Human Rights and Peace-Building Approach to Migration Governance in the Sahel
Caught in the middle A human rights and peace-building approach to migration governance in the Sahel Fransje Molenaar CRU Report Jérôme Tubiana Clotilde Warin Caught in the middle A human rights and peace-building approach to migration governance in the Sahel Fransje Molenaar Jérôme Tubiana Clotilde Warin CRU Report December 2018 December 2018 © Netherlands Institute of International Relations ‘Clingendael’. Cover photo: © Jérôme Tubiana. Unauthorized use of any materials violates copyright, trademark and / or other laws. Should a user download material from the website or any other source related to the Netherlands Institute of International Relations ‘Clingendael’, or the Clingendael Institute, for personal or non-commercial use, the user must retain all copyright, trademark or other similar notices contained in the original material or on any copies of this material. Material on the website of the Clingendael Institute may be reproduced or publicly displayed, distributed or used for any public and non-commercial purposes, but only by mentioning the Clingendael Institute as its source. Permission is required to use the logo of the Clingendael Institute. This can be obtained by contacting the Communication desk of the Clingendael Institute ([email protected]). The following web link activities are prohibited by the Clingendael Institute and may present trademark and copyright infringement issues: links that involve unauthorized use of our logo, framing, inline links, or metatags, as well as hyperlinks or a form of link disguising the URL. About the authors Fransje Molenaar is a Senior Research Fellow with Clingendael’s Conflict Research Unit, where she heads the Sahel/Libya research programme. She specializes in the political economy of (post-) conflict countries, organized crime and its effect on politics and stability. -

Download File
NIGER: COVID-19 Situation Report – #09 22 June to 20 July 2020 Situation in Numbers 1,105 COVID-19 confirmed cases 69 deaths 6,25% Lethality rate @UNICEFNiger/J.Haro (Ministère de la Santé Publique, July 20th, Situation Overview and Humanitarian Needs 2020) As of the end of the reporting period, Niger registered 1,105 cases of COVID-19, 1,014 3,800,000 patients healed, 69 deaths, 9,197 followed contacts, with a decreasing trend in cases. Children affected Even if the rate of imported cases is high, local transmission is still active. 4 out of 8 by COVID-19 regions didn’t report any cases for at least 2 weeks. UNICEF works closely with the Government and its partners to respond to the ongoing outbreak in the country, which is school reopening already facing the consequences of multiple crisis (nutrition, conflicts, natural disasters). As part of the national COVID-19 response plan, UNICEF is providing technical support to the government of Niger to scale-up the national safety net program to mitigate the social and economic impacts of the COVID-19 crisis on the most vulnerable population, US$ 25.8 M with a special focus on children and women needs. UNICEF continues to support the back funding required to school activities by providing the Ministry of Education with Education and WASH supplies, technical assistance, key messages about COVID-19 prevention and a monitoring system based on RapidPro. UNICEF assists particularly the Ministry of Health (MoH), in the field of risk communication/community engagement (RCCE), infection prevention and control (IPC), supply and logistics, epidemiological surveillance and healthcare provision and it is co-leading 3 of the 8 sub-committees established by the MoH (RCCE, IPC and logistics) at central and sub-national level. -
Lake Chad Basin Fact Sheet #3.Pdf
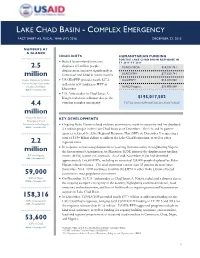
LAKE CHAD BASIN - COMPLEX EMERGENCY FACT SHEET #3, FISCAL YEAR (FY) 2016 DECEMBER 22, 2015 NUMBERS AT A GLANCE HIGHLIGHTS HUMANITARIAN FUNDING FOR THE LAKE CHAD BASIN RESPONSE IN Boko Haram-related insecurity FY 2015–FY 2016 2.5 displaces 2.5 million people; USAID/OFDA1 $30,287,761 displacement increases significantly in million Cameroon and Chad in recent months USAID/FFP2 $77,629,741 People Displaced by Boko USAID/FFP provides nearly $27.2 State/PRM3 $53,300,000 Haram-Related Insecurity million in new funding to WFP in in Lake Chad Basin USAID/Nigeria $33,800,000 OCHA – December 2015 December U.S. Ambassador to Chad James A. Knight redeclares a disaster due to the $195,017,502 4.4 ongoing complex emergency TOTAL USG HUMANITARIAN ASSISTANCE million People in Need of KEY DEVELOPMENTS Emergency Food Assistance in the Region Ongoing Boko Haram-related violence continues to result in insecurity and has displaced OCHA – December 2015 2.5 million people in the Lake Chad Basin as of December. The UN and its partner agencies released the Sahel Regional Response Plan (SRP) on December 9, requesting a total of $1.98 billion dollars to address the Lake Chad Basin crisis, as well as other 2.2 regional crises. In response to increasing displacement resulting from insecurity in neighboring Nigeria, million the International Organization for Migration (IOM) initiated the displacement tracking IDPs in Nigeria matrix (DTM) system in Cameroon. As of mid-November, IOM had identified IOM – November 2015 approximately 158,300 IDPs, including an estimated 124,000 people displaced by Boko Haram-related violence. -

WHO Emergency Health Programme for the Food Crisis in Niger Situation Report # 13 1 to 7 November 2005
Health action in crisis WHO Emergency Health Programme for the Food Crisis in Niger Situation Report # 13 1 to 7 November 2005 I. Highlights • A project for 79 000 Euros, for expansion of the current national communicable diseases surveillance system to include nutritional surveillance through the timely collection of data on malnutrition and analysis for appropriate response in Niger, was submitted to the Humanitarian Aid Department of the European Commission (ECHO) by the WHO Niger Representative. • WHO and partners are scheduling additional training courses for healthcare workers on the treatment of malnutrition from all eight regions of Niger (Agadez, Diffa, Dosso, Maradi, Niamey, Tahoua, Tilla- bery and Zinder) to respond to increased requests. It was planned to provide training for 450 health- care workers by the end 31 December 2005. This has already been exceeded. By 7 November, 503 healthcare workers had received training. Of the 503, 48 participated in the training for healthcare trainers on the treatment of malnutrition and 455 participated in training on the treatment of malnutri- tion. • The WHO collaborating centre, Burlo-Garofolo Regional Paediatric Hospital Institute of Child Health, Trieste, Italy, seconded a paediatric-nurse to WHO Niger for the period of one month from the 4 No- vember 2005. The paediatric-nurse is based at the Tillaberi Hospital and Intensive Nutritional Reha- bilitation Centre and will provide technical support to paramedical personnel in charge of the treat- ment of children under five years suffering from severe malnutrition upon request of the local authorities. • Partners of the interagency group on nutrition provided an update of activities at the weekly coordina- tion meeting held at UNICEF on 4 November 2005. -
Local Governance Opportunities for Sustainable Migration Management in Agadez
Local governance opportunities for sustainable migration management in Agadez Fransje Molenaar CRU Report Anca-Elena Ursu Bachirou Ayouba Tinni Supported by: Local governance opportunities for sustainable migration management in Agadez Fransje Molenaar Anca-Elena Ursu Bachirou Ayouba Tinni CRU Report October 2017 October 2017 © Netherlands Institute of International Relations ‘Clingendael’. Cover photo: Men sitting on a bench at the Agadez Market. © Boris Kester / traveladventures.org Unauthorised use of any materials violates copyright, trademark and / or other laws. Should a user download material from the website or any other source related to the Netherlands Institute of International Relations ‘Clingendael’, or the Clingendael Institute, for personal or non-commercial use, the user must retain all copyright, trademark or other similar notices contained in the original material or on any copies of this material. Material on the website of the Clingendael Institute may be reproduced or publicly displayed, distributed or used for any public and non-commercial purposes, but only by mentioning the Clingendael Institute as its source. Permission is required to use the logo of the Clingendael Institute. This can be obtained by contacting the Communication desk of the Clingendael Institute ([email protected]). The following web link activities are prohibited by the Clingendael Institute and may present trademark and copyright infringement issues: links that involve unauthorized use of our logo, framing, inline links, or metatags, as well as hyperlinks or a form of link disguising the URL. About the authors Fransje Molenaar is a research fellow at the Clingendael Institute’s Conflict Research Unit Anca-Elena Ursu is a research assistant at the Clingendael Institute’s Conflict Research Unit Bachirou Ayouba Tinni is a PhD student at the University of Niamey The Clingendael Institute P.O. -
Assessment of Chronic Food Insecurity in Niger
Assessment of Chronic Food Insecurity in Niger Analysis Coordination March 2019 Assessment of Chronic Food Insecurity in Niger 2019 About FEWS NET Created in response to the 1984 famines in East and West Africa, the Famine Early Warning Systems Network (FEWS NET) provides early warning and integrated, forward-looking analysis of the many factors that contribute to food insecurity. FEWS NET aims to inform decision makers and contribute to their emergency response planning; support partners in conducting early warning analysis and forecasting; and provide technical assistance to partner-led initiatives. To learn more about the FEWS NET project, please visit www.fews.net. Acknowledgements This publication was prepared under the United States Agency for International Development Famine Early Warning Systems Network (FEWS NET) Indefinite Quantity Contract, AID-OAA-I-12-00006. The author’s views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government. Recommended Citation FEWS NET. 2019. Assessment of Chronic Food Insecurity in Niger. Washington, DC: FEWS NET. Famine Early Warning Systems Network ii Assessment of Chronic Food Insecurity in Niger 2019 Table of Contents Executive Summary ..................................................................................................................................................................... 1 Background ............................................................................................................................................................................. -

Ref Agadeza1.Pdf
REGION D'AGADEZ: Carte référentielle Légende L i b y e ± Chef lieu de région Chef lieu de département localité Route principale Route secondaire ou tertiaire Frontière internationale Frontière régionale Cours d'eau MADAMA Région d'Agadez A l g é r i e ☶ Population Djado DJABA DJADO CHIRFA KANARIA I-N-AZAOUA SARA BILMA DAOTIMMI I-N-TADERA ☶ 17 459 TOUARET SEGUEDINE IFEROUANE TAGHAJIT TAMJIT TAZOUROUTETASSOS INTIKIKITENE OURARENE AGALANGAÏ ☶ 32 864 DOUMBA EZAZAW FARAZAKAT ANEY ASSAMAKKA ABARGOT TEZIRZEK LOTEY TCHOUGOY TIRAOUENE TAKARATEMAMANAT ZOURIKA EMI TCHOUMA AZATRAYA AGREROUM ET TCHWOUN ARLIT Gougaram ACHENOUMA IFEROUANE ISSAWANE ARRIGUI Dirkou ACHEGOUR TEMET DIRKOU ☶ 103 369 INIGNAOUEI TILALENE ARAKAW MAGHET TAKRIZA TARHMERT ARLIT AGAMGAM BILMA ANOU OUACHCHERENE TCHIGAYEN TAZOURAT TAGGAFADI Dannet GOUGARAM SIDAOUET ZOMO ASSODE IBOUL TCHILHOURENE ERISMALAN TIESTANE Bilma MAZALALE AJIWA INNALARENE TAZEWET AGHAROUS ESSELEL ZOBABA ANOUZAGHARAN DANNET FAYAYE Timia FACHI TIGUIR AJIR IMOURAREN TIMIA FACHI MARI Fachi TAKARACHE ZIKAT OFENE MALLETAS AKEREBREB ABELAJOUAD TCHINOUGOUWENEARITAOUA IN-ABANGHARIT TAMATEDERITTASSEDET ASSAK HARAU INTAMADE T c h a d EGHARGHAR TILIA OOUOUARI Dabaga ELMEKI BOURNI TIDEKAL SEKIRET ASSESA MERIG AKARI TELOUES EGANDAWEL AOUDERAS EOULEM SOGHO TAGAZA ATKAKI TCHIROZERINE TABELOT EGHOUAK M a l i AZELIK DABLA ABARDOKH TALAT INGAL IMMASSATANE AMAN NTEDENT ELDJIMMA ☶ 241 007 GUERAGUERA TEGUIDDA IN TESSOUM ABAZAGOR Tabelot FAGOSCHIA DABAGA TEGUIDDA IN TAGAIT I-N-OUTESSANE ☶ EKIZENGUI AGALGOU 51 818 TCHIROZERINE INGOUCHIL -

Food Insecurity
Emergency appeal n° MDRNE005 Niger: GLIDE n° OT2010000028-NER 29 June 2010 Food Insecurity Appeal target (revised budget): CHF 3,670,607 (USD 3.2 m or EUR 2.2m) <click here to view the attached Revised Emergency Appeal Budget> Appeal coverage: 23% (revised budget); <click here to go directly to the updated donor response report, or here to link to contact details> Appeal history: • This Emergency Appeal was initially launched on 18 March, 2010 for CHF 986,862 for nine months to assist 300,000 beneficiaries. • Disaster Relief Emergency Fund (DREF): CHF 229,046 was initially allocated from the Federation’s DREF on 22 February 2010 to support the Red Cross Society of Niger (NRCS) to start the response operation. • Appeal budget revision and extension: due to new reports of the government and partners (19 May, 2010) which raises the severe food insecurity affected population from 2.7 to 3.3 million, the appeal has been revised to CHF 3.65 million and extended until March 2011. • Some 215 villages are already being reached instead of the 120 initially planned. Special Niger Red Cross volunteer screening children for emphasis will be put on: a) meeting emergency referral to centres for treatment of acute food and household needs through cash malnutrition, Tahoua Region, Niger, April 2010 programming, i) addressing the acute malnutrition in children under five by providing community-based screening and referral of acute malnutrition cases, and support for better infant and young child feeding practices through nutrition education, and ii) supporting early recovery through seeds and tools distribution, and improved harvest, iii) strengthening the capacity of the NRCS to deliver the needed services to 384,998 beneficiaries. -

Tahaoua Abalak Bagaroua Birni Nkonni Bouza Illela Keita Madaoua Malbaza Tahouha Tassara Tchintabaraden Tillia
Niger: Atlas admin1 Agadez Tahaoua Agadez Tahaoua Aderbissinat Abalak Arlit Bagaroua Birma Birni Nkonni Iferouane Bouza Ingall Illela Tcirozerine Keita Madaoua Diffa Malbaza Diffa Tahouha Bosso Tassara Goudou Maria Tchintabaraden Maine Soroa Tillia Ngourti Nguigmi Tillabéri Agadez Tillabéri Dosso Abala Dosso Ayerou Boboye Balleyara Dioundiou Banbangou Dogondoutchi Banikilare Falmey Filingue Gaya Goteheye Loga Kollo Diffa Tibiri Ouallam Tahoua Say Maradi Tera Tillabéri Zinder Maradi Torodi Aguie Maradi Bermo Zinder Niamey Dakoro Zinder Dosso Gazaoua Beledji Guidan Roumdji Ayerou Madarounfa Damagaram Takaya Mayahi Dungass Tessaoua Goure Kantche Niamey Magara Niamey Mirriah Tafeita Tanout Niger: Reference map of Agadez ! Fort Gardel !! Ghat ! ! Al Quatrun Eferi ! Al Wigh LIBYA ! Ami Madema In-Amdjel ! ! Ain az Zan ! Tamanraset !! ALGERIA Bardaa !! Djado Creation date: 02/05/2018 ! TIBESTI Data soures: OCHA, ESRI, UNCS, Zouar DCW, IGNN ! Paper size: A4 Iferouane Bilma Disclaimers The boundaries and names shown and the designations used on these maps do not Garin Malam ! Arlit imply official endorsement CHAD or acceptance by the Iferouane Dirkou ! ! United Nations. Arlit Bilma ! ! KIDAL 0 100 200 Dannet km ! Timia Fachi ! ! Tchirozerine ! Ingall Tabelot BORKOU Tchirozerine ! ^! ! National capital Tassara Ingall ! GAO ! ! Agadez !! Admin1 capital Tillia Aderbissinat ! ! DIFFA Main town ! Tamaya INTERNATIONAL BOUNDARIES TAHOUA !Aderbissinat Abalak ! N'Gourti ADMIN1 BOUNDARIES ZINDER ! Tesker ! KANEM Admin2 boundaries Abala Tahoua ! Tanout ! !! TILLABERI Nokou Main road Bouza ! Filingue ! ! ! Illela N'Guigmi MARADI ! Mao Secondary road Goure LAC !! Malbaza! Mayahi Sofoua ! ! Liwa! Local road !! Zinder Goudoumaria Bosso ! ! ! ! ! ! !! !! !! ! Niger: Reference map of Diffa ! Bilma TIBESTI AGADEZ BORKOU Creation date: 02/05/2018 Data soures: OCHA, ESRI, UNCS, DCW, IGNN Paper size: A4 N'Gourti Disclaimers The boundaries and names shown and the designations used on these maps do not imply official endorsement or acceptance by the CHAD United Nations.