Coughing, Fatigue, Shortness of Breath—If You Have These Symptoms Over
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Slipping Rib Syndrome
Slipping Rib Syndrome Jackie Dozier, BS Edited by Lisa E McMahon, MD FACS FAAP David M Notrica, MD FACS FAAP Case Presentation AA is a 12 year old female who presented with a 7 month history of right-sided chest/rib pain. She states that the pain was not preceded by trauma and she had never experienced pain like this before. She has been seen in the past by her pediatrician, chiropractor, and sports medicine physician for her pain. In May 2012, she was seen in the ER after having manipulations done on her ribs by a sports medicine physician. Pain at that time was constant throughout the day and kept her from sleeping. However, it was relieved with hydrocodone/acetaminophen in the ER. Case Presentation Over the following months, the pain became progressively worse and then constant. She also developed shortness of breath. She is a swimmer and says she has had difficulty practicing due to the pain and SOB. AA was seen by a pediatric surgeon and scheduled for an interventional pain management service consult for a test injection. Following good temporary relief by local injection, she was scheduled costal cartilage removal to treat her pain. What is Slipping Rib Syndrome? •Slipping Rib Syndrome (SRS) is caused by hypermobility of the anterior ends of the false rib costal cartilages, which leads to slipping of the affected rib under the superior adjacent rib. •SRS an lead to irritation of the intercostal nerve or strain of the muscles surrounding the rib. •SRS is often misdiagnosed and can lead to months or years of unresolved abdominal and/or thoracic pain. -

Signs and Symptoms of COPD
American Thoracic Society PATIENT EDUCATION | INFORMATION SERIES Signs and Symptoms of COPD Chronic obstructive pulmonary disease (COPD) can cause shortness of breath, tiredness, Short ness of Breath production of mucus, and cough. Many people with COPD develop most if not all, of these signs Avo iding Activities and symptoms. Sho rtness wit of Breath h Man s Why is shortness of breath a symptom of COPD? y Activitie Shortness of breath (or breathlessness) is a common Avoiding symptom of COPD because the obstruction in the A breathing tubes makes it difficult to move air in and ny Activity out of your lungs. This produces a feeling of difficulty breathing (See ATS Patient Information Series fact sheet Shor f B tness o on Breathlessness). Unfortunately, people try to avoid this reath Sitting feeling by becoming less and less active. This plan may or Standing work at first, but in time it leads to a downward spiral of: avoiding activities which leads to getting out of shape or becoming deconditioned, and this can result in even more Is tiredness a symptom of COPD? shortness of breath with activity (see diagram). Tiredness (or fatigue) is a common symptom in COPD. What can I do to treat shortness of breath? Tiredness may discourage you from keeping active, which leads to greater loss of energy, which then leads to more If your shortness of breath is from COPD, you can do several tiredness. When this cycle begins it is sometimes hard to things to control it: break. CLIP AND COPY AND CLIP ■■ Take your medications regularly. -

Chest Pain and Non-Respiratory Symptoms in Acute Asthma
Postgrad Med J 2000;76:413–414 413 Chest pain and non-respiratory symptoms in Postgrad Med J: first published as 10.1136/pmj.76.897.413 on 1 July 2000. Downloaded from acute asthma W M Edmondstone Abstract textbooks. Occasionally the combination of The frequency and characteristics of chest dyspnoea and chest pain results in diagnostic pain and non-respiratory symptoms were confusion. This study was prompted by the investigated in patients admitted with observation that a number of patients admitted acute asthma. One hundred patients with with asthmatic chest pain had been suspected a mean admission peak flow rate of 38% of having cardiac ischaemia, pleurisy, pericardi- normal or predicted were interviewed tis, or pulmonary embolism. It had also been using a questionnaire. Chest pain oc- observed that many patients admitted with curred in 76% and was characteristically a asthma complained of a range of non- dull ache or sharp, stabbing pain in the respiratory symptoms, something which has sternal/parasternal or subcostal areas, been noted previously in children1 and in adult worsened by coughing, deep inspiration, asthmatics in outpatients.2 The aim of this or movement and improved by sitting study was to examine the frequency and char- upright. It was rated at or greater than acteristics of chest pain and other symptoms in 5/10 in severity by 67% of the patients. A patients admitted with acute asthma. wide variety of upper respiratory and sys- temic symptoms were described both Patients and methods before and during the attack. One hundred patients (66 females, mean (SD) Non-respiratory symptoms occur com- age 45.0 (19.7) years) admitted with acute monly in the prodrome before asthma asthma were studied. -
Sputum Collection Instructions Step 1 Step 2 Step 3
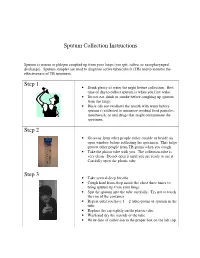
Sputum Collection Instructions Sputum is mucus or phlegm coughed up from your lungs (not spit, saliva, or nasopharyngeal discharge). Sputum samples are used to diagnose active tuberculosis (TB) and to monitor the effectiveness of TB treatment. Step 1 • Drink plenty of water the night before collection. Best time of day to collect sputum is when you first wake. • Do not eat, drink or smoke before coughing up sputum from the lungs. • Rinse (do not swallow) the mouth with water before sputum is collected to minimize residual food particles, mouthwash, or oral drugs that might contaminate the specimen. Step 2 • Go away from other people either outside or beside an open window before collecting the specimen. This helps protect other people from TB germs when you cough. • Take the plastic tube with you. The collection tube is very clean. Do not open it until you are ready to use it. Carefully open the plastic tube. Step 3 • Take several deep breaths. • Cough hard from deep inside the chest three times to bring sputum up from your lungs. • Spit the sputum into the tube carefully. Try not to touch the rim of the container. • Repeat until you have 1 – 2 tablespoons of sputum in the tube. • Replace the cap tightly on the plastic tube. • Wash and dry the outside of the tube. • Write date of collection in the proper box on the lab slip. Step 4 • Place the primary specimen container (usually a conical centrifuge tube) in the clear plastic baggie that has the biohazard symbol imprint. • Place the white absorbent sheet in the plastic baggie. -

Perinatal/Neonatal Case Presentation
Perinatal/Neonatal Case Presentation &&&&&&&&&&&&&& Urinary Tract Infection With Trichomonas vaginalis in a Premature Newborn Infant and the Development of Chronic Lung Disease David J. Hoffman, MD vaginal bleeding with suspected abruption resulted in delivery of Gerard D. Brown, DO the infant by Cesarean section. The Apgar scores were 1, 5, and 9 Frederick H. Wirth, MD at 1, 5, and 10 minutes of life, respectively. Betsy S. Gebert, CRNP After delivery, the infant was managed with mechanical Cathy L. Bailey, MS, CRNP ventilation with pressure support and volume guarantee for Endla K. Anday, MD respiratory distress syndrome. She received exogenous surfactant We report a case of a low-birth-weight infant with an infection of the urinary tract with Trichomonas vaginalis, who later developed cystic chronic lung disease suggestive of Wilson-Mikity syndrome. Although she had mild respiratory distress syndrome at birth, the extent of the chronic lung disease was out of proportion to the initial illness. We speculate that maternal infection with this organism may have resulted in an inflammatory response that led to its development. Journal of Perinatology (2003) 23, 59 – 61 doi:10.1038/sj.jp.7210819 CASE PRESENTATION A 956-g, appropriate-for-gestational-age, African–American female was delivered by Cesarean section following 27 5/7 weeks of gestation in breech presentation after a period of advanced cervical dilatation and uterine contractions. Her mother was a 20-year-old gravida 5, para 2022 woman whose prenatal laboratory data were significant for vaginal colonization with Streptococcus agalactiae, treatment for Chlamydia trachomatis, and a history of cocaine and marijuana usage confirmed by urine toxicology. -

Factors Associated with Pleurisy in Pigs: a Case-Control Analysis of Slaughter Pig Data for England and Wales
Aus dem Zentrum für Klinische Tiermedizin der Tierärztlichen Fakultät der Ludwig-Maximilians-Universität München Arbeit angefertigt unter der Leitung von Prof. Dr. Mathias Ritzmann Angefertigt am Cambridge Infectious Diseases Consortium, University of Cambridge, Department of Veterinary Medicine, Cambridge, UK (Dr. A W (Dan) Tucker) Factors associated with pleurisy in pigs: A case-control analysis of slaughter pig data for England and Wales Inaugural-Dissertation zur Erlangung der tiermedizinischen Doktorwürde der Tierärztlichen Fakultät der Ludwig-Maximilians-Universität München Von Henrike Caroline Jäger aus Wiesbaden München 2012 Gedruckt mit der Genehmigung der Tierärztlichen Fakultät der Ludwig-Maximilians-Universität München Dekan: Univ.-Prof. Dr. Joachim Braun Berichterstatter: Univ.-Prof. Dr. Mathias Ritzmann Korreferent: Univ.-Prof. Dr. Dr. habil. Manfred Gareis Tag der Promotion: 9. Februar 2013 Meinem Vater Dr. med Sepp-Dietrich Jäger Table of Contents 4 TABLE OF CONTENTS I. INTRODUCTION ...................................................................................... 7 II. LITERATURE OVERVIEW .................................................................... 8 1. Anatomy and Physiology of the Pleura ....................................................8 2. Pleurisy ........................................................................................................9 2.1. Morphology ..................................................................................................9 2.2. Prevalence ..................................................................................................11 -

Chest Pain in Pediatrics
PEDIATRIC CARDIOLOGY 0031-3955/99 $8.00 + .OO CHEST PAIN IN PEDIATRICS Keith C. Kocis, MD, MS Chest pain is an alarming complaint in children, leading an often frightened and concerned family to a pediatrician or emergency room and commonly to a subsequent referral to a pediatric cardiologist. Because of the well-known associ- ation of chest pain with significant cardiovascular disease and sudden death in adult patients, medical personnel commonly share heightened concerns over pediatric patients presenting with chest pain. Although the differential diagnosis of chest pain is exhaustive, chest pain in children is least likely to be cardiac in origin. Organ systems responsible for causing chest pain in children include*: Idiopathic (12%-85%) Musculoskeletal (15%-31%) Pulmonary (12%-21%) Other (4%-21%) Psychiatric (5%-17%) Gastrointestinal (4'/0-7%) Cardiac (4%4%) Furthermore, chest pain in the pediatric population is rareZy associated with life-threatening disease; however, when present, prompt recognition, diagnostic evaluation, and intervention are necessary to prevent an adverse outcome. This article presents a comprehensive list of differential diagnostic possibilities of chest pain in pediatric patients, discusses the common causes in further detail, and outlines a rational diagnostic evaluation and treatment plan. Chest pain, a common complaint of pediatric patients, is often idiopathic in etiology and commonly chronic in nature. In one study,67 chest pain accounted for 6 in 1000 visits to an urban pediatric emergency room. In addition, chest pain is the second most common reason for referral to pediatric cardiologist^.^, 23, 78 Chest pain is found equally in male and female patients, with an average *References 13, 17, 23, 27, 32, 35, 44, 48, 49, 63-67, 74, and 78. -

Management of Wheeze and Cough in Infants and Pre-Schoo L Children In
nPersonal opinio lManagement of wheeze and cough in infants and pre-schoo echildren in primary car Pauln Stephenso nIntroductio is, well established in adults 2thoughs there remain somer controversy about its diagnosis in children eve Managementa of wheeze and cough in children is sinceh Spelman's uncontrolled study of children wit commonm problem in primary care. In this paper I ai nchronic cough successfully treated according to a tod provide a few useful management tools with regar .asthma protocol 3gWithout the ability to perform lun toe diagnosis, the role of a trial of treatment, and th functione tests in pre-school children, care must b rationalee for referral. For an in-depth review see th takent to exclude other diagnoses. A persisten article. in this journal two years ago by Bush 1 eproductiv coughc may be due solely to chroni catarrhe with postnasal drip, but early referral may b sPresentation of Symptom needed. A persistent dry cough,n worse at night and o exercise,s and without evidence of other diagnose Ity is always worth asking parents what they mean b warrants. a trial of asthma treatment thed term 'wheeze' or 'cough'. The high-pitche musicaln noise of a wheeze usually on expiratio Thef younger the child, the longer the list o shouldy not be confused with the sound of inspirator differentialo diagnoses and the more one has t sstridor. The sound of airflow through secretions i econsider possibilities other than 'asthma'. Thes ddifferent again, and parents may describe their chil linclude upper airways disease, congenital structura 'vomiting'g when, in fact, the child has been coughin diseasel of the bronchi, bronchial or trachea severely and bringing up phlegm or mucus. -

Breathing Better with a COPD Diagnosis
Difficulty Breathing Chronic Bronchitis Smoker’s Cough Chronic Coughing Wheezing Em- Chronic Obstructive Pulmonary Disease physema Shortness of Breath Feeling of Suffocation Excess Mucus Difficulty Breathing Chronic Bronchitis Smoker’s Cough Chronic Coughing Wheezing Emphysema Shor tness of Breath Feeling of Suffocation Excess Mucus Difficulty Breathing Chronic Bronchitis Smoker’s Cough Chronic Coughing Wheezing Emphysema Shortness of Breath Feeling of Suffocation Excess Mucus Difficulty Breathing Chronic Bronchitis Smoker’s Cough Chron- ic Coughing Wheezing Emphysema Shortness of Breath Feeling of Suffocation Excess Mu- cus DifficultyBreathing Breathing Chronic Bronchitis Better Smoker’s Cough Chronic Coughing Wheezing Emphysema Shortness of Breath Feeling of Suffocation Excess Mucus Difficulty Breathing Chronic Bronchitis Smoker’s Cough Chronic Coughing Wheezing Emphysema Shor tness of Breath Feeling of SuffocationWith Excess a COPDMucus Difficulty Diagnosis Breathing Chronic Bronchitis Smoker’s Cough Chronic Coughing Wheezing Emphysema Shortness of Breath Feeling of did you know? When COPD is severe, shortness of breath and other COPDdid you is the know? 4th leading cause of death in the symptomswhen you can get are in the diagnosed way of doing even the most UnitedCOPD States.is the 4th The leading disease cause kills ofmore death than in 120,000 basicwith tasks, copd such as doing light housework, taking a Americansthe United eachStates year—that’s and causes 1 serious, death every long-term 4 walk,There and are even many bathing things and that getting you can dressed. do to make minutes—anddisability. The causesnumber serious, of people long-term with COPDdisability. is COPDliving withdevelops COPD slowly, easier: and can worsen over time, increasing.The number More of people than 12with million COPD people is increasing. -

What Is Pertussis (Whooping Cough)?
American Thoracic Society PATIENT EDUCATION | INFORMATION SERIES What Is Pertussis (Whooping Cough)? Pertussis is a very contagious respiratory infection commonly known as ‘whooping cough’. It is caused by a bacterium called Bordetella pertussis. The infection became much less common after a successful vaccine was developed and given to children to help prevent infection. However, in recent years, the number of people infected with pertussis has increased and now is at the highest rate seen since the 1950’s. There is concern that this is due mainly to people not taking the pertussis (whooping cough) vaccination and adults who have not had a booster and their immune protection has weakened with age. Whooping cough usually starts as a mild cold-like illness get in the air. If you are close enough, you can breathe in these (upper respiratory infection). The pertussis bacteria enter the droplets or they can land on your mouth, nose, or eye. You lungs and cause swelling and irritation in the airways leading can also get the infection if you kiss the face of a person with to severe coughing fits. At times, people with whooping pertussis or get infected nose or mouth secretions on your cough can have a secondary pneumonia from other bacteria hands and then touch your own face to rub your eyes or nose. while they are ill. Whooping cough can cause very serious A person with pertussis can remain contagious for many weeks illness. It is most dangerous in young babies and can result unless treated with an antibiotic. in death. It spreads very easily and people who have the infection can still spread it to others for weeks after they What are the symptoms of Pertussis infection? become sick. -

Gas Exchange and Respiratory Function
LWBK330-4183G-c21_p484-516.qxd 23/07/2009 02:09 PM Page 484 Aptara Gas Exchange and 5 Respiratory Function Applying Concepts From NANDA, NIC, • Case Study and NOC A Patient With Impaired Cough Reflex Mrs. Lewis, age 77 years, is admitted to the hospital for left lower lobe pneumonia. Her vital signs are: Temp 100.6°F; HR 90 and regular; B/P: 142/74; Resp. 28. She has a weak cough, diminished breath sounds over the lower left lung field, and coarse rhonchi over the midtracheal area. She can expectorate some sputum, which is thick and grayish green. She has a history of stroke. Secondary to the stroke she has impaired gag and cough reflexes and mild weakness of her left side. She is allowed food and fluids because she can swallow safely if she uses the chin-tuck maneuver. Visit thePoint to view a concept map that illustrates the relationships that exist between the nursing diagnoses, interventions, and outcomes for the patient’s clinical problems. LWBK330-4183G-c21_p484-516.qxd 23/07/2009 02:09 PM Page 485 Aptara Nursing Classifications and Languages NANDA NIC NOC NURSING DIAGNOSES NURSING INTERVENTIONS NURSING OUTCOMES INEFFECTIVE AIRWAY CLEARANCE— RESPIRATORY MONITORING— Return to functional baseline sta- Inability to clear secretions or ob- Collection and analysis of patient tus, stabilization of, or structions from the respiratory data to ensure airway patency improvement in: tract to maintain a clear airway and adequate gas exchange RESPIRATORY STATUS: AIRWAY PATENCY—Extent to which the tracheobronchial passages remain open IMPAIRED GAS -

Rivaroxaban (Xarelto®)
Rivaroxaban (Xarelto®) To reduce your bleeding and clotting risk it is important that you attend follow-up appointments with your provider, and have blood tests done as your provider orders. What is rivaroxaban (Xarelto®)? • Rivaroxaban is also called Xarelto® • Rivaroxaban(Xarelto®) is used to reduce the risk of blood clots and stroke in people with an abnormal heart rhythm known as atrial fibrillation, in people who have had a blood clot, or in people who have undergone orthopedic surgery. o Blood clots can block a blood vessel cutting off blood supply to the area. o Rarely, clots can break into pieces and travel in the blood stream, lodging in the heart (causing a heart attack), the lungs (causing a pulmonary embolus), or in the brain (causing a stroke). • If you were previously on Warfarin/Coumadin® and you are starting Rivaroxaban(Xarelto®), do not continue taking warfarin. Rivaroxaban(Xarelto®) replaces warfarin. Xarelto 10mg tablet Xarelto 15mg tablet Xarelto 20mg tablet How should I take rivaroxaban (Xarelto®)? • Take Rivaroxaban(Xarelto®) exactly as prescribed by your doctor. • Rivaroxaban(Xarelto®) should be taken with food. • Rivaroxaban(Xarelto®) tablets may be crushed and mixed with applesauce to make the tablet easier to swallow. - 1 - • If you missed a dose: o Take it as soon as you remember on the same day. • Do not stop taking rivaroxaban suddenly without telling your doctor. This can put you at risk of having a stroke or a blood clot. • If you take too much rivaroxaban, call your doctor or the anticoagulation service. If you are experiencing any bleeding which you cannot get to stop, go to the nearest emergency room.