Zambia Country Operational Plan (COP) 2017 Strategic Direction Summary March 16, 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Zambia 30 September 2017
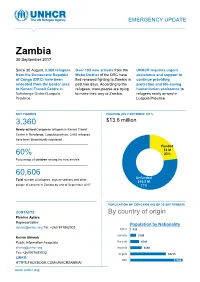
EMERGENCY UPDATE Zambia 30 September 2017 Since 30 August, 3,360 refugees Over 100 new arrivals from the UNHCR requires urgent from the Democratic Republic Moba District of the DRC have assistance and support to of Congo (DRC) have been fled renewed fighting to Zambia in continue providing relocated from the border area past two days. According to the protection and life-saving to Kenani Transit Centre in refugees, more people are trying humanitarian assistance to Nchelenge District/Luapula to make their way to Zambia. refugees newly arrived in Province. Luapula Province. KEY FIGURES FUNDING (AS 2 OCTOBER 2017) 3,360 $13.6 million requested for Zambia operation Newly-arrived Congolese refugees in Kenani Transit Centre in Nchelenge, Luapula province. 2,063 refugees have been biometrically registered Funded $3 M 60% 23% Percentage of children among the new arrivals Unfunded XX% 60,606 [Figure] M Unfunded Total number of refugees, asylum-seekers and other $10.5 M people of concern in Zambia by end of September 2017 77% POPULATION OF CONCERN (AS OF 30 SEPTEMBER) CONTACTS By country of origin Pierrine Aylara Representative Population by Nationality [email protected] Tel: +260 977862002 Other 415 Somalia 3199 Kelvin Shimoh Public Information Associate Burundi 4749 [email protected] Rwanda 6130 Tel: +260979585832 Angola 18715 LINKS: DRC 27398 HTTPS:FACEBOOK.COM/UNHCRZAMBIA/ www.unhcr.org 1 EMERGENCY UPDATE > Zambia / 30 September 2017 Emergency Response Luapula province, northern Zambia Since 30 August, over 3,000 asylum-seekers from the Democratic Republic of Congo (DRC) have crossed into northern Zambia. New arrivals are reportedly fleeing insecurity and clashes between Congolese security forces FARDC and a local militia groups in towns of Pweto, Manono, Mitwaba (Haut Katanga Province) as well as in Moba and Kalemie (Tanganyika Province). -

Zambia Country Operational Plan (COP) 2016 Strategic Direction Summary
Zambia Country Operational Plan (COP) 2016 Strategic Direction Summary June 14, 2016 Table of Contents Goal Statement 1.0 Epidemic, Response, and Program Context 1.1 Summary statistics, disease burden and epidemic profile 1.2 Investment profile 1.3 Sustainability profile 1.4 Alignment of PEPFAR investments geographically to burden of disease 1.5 Stakeholder engagement 2.0 Core, near-core and non-core activities for operating cycle 3.0 Geographic and population prioritization 4.0 Program Activities for Epidemic Control in Scale-up Locations and Populations 4.1 Targets for scale-up locations and populations 4.2 Priority population prevention 4.3 Voluntary medical male circumcision (VMMC) 4.4 Preventing mother-to-child transmission (PMTCT) 4.5 HIV testing and counseling (HTS) 4.6 Facility and community-based care and support 4.7 TB/HIV 4.8 Adult treatment 4.9 Pediatric treatment 4.10 Orphans and vulnerable children (OVC) 5.0 Program Activities in Sustained Support Locations and Populations 5.1 Package of services and expected volume in sustained support locations and populations 5.2 Transition plans for redirecting PEPFAR support to scale-up locations and populations 6.0 Program Support Necessary to Achieve Sustained Epidemic Control 6.1 Critical systems investments for achieving key programmatic gaps 6.2 Critical systems investments for achieving priority policies 6.3 Proposed system investments outside of programmatic gaps and priority policies 7.0 USG Management, Operations and Staffing Plan to Achieve Stated Goals Appendix A- Core, Near-core, Non-core Matrix Appendix B- Budget Profile and Resource Projections 2 Goal Statement Along with the Government of the Republic of Zambia (GRZ), the U.S. -

RAPID FLOOD IMPACT ASSESSMENT REPORT March 2007
RAPID FLOOD IMPACT ASSESSMENT REPORT March 2007 VAC ZAMBIA Vulnerability Assessment Committee BY THE ZAMBIA VULNERABILITY ASSESSMENT COMMITTEE (ZVAC) LUSAKA Table of Contents Acknowledgements...........................................................................................................................4 Acronyms .........................................................................................................................................5 EXECUTIVE SUMMARY...............................................................................................................6 1.0 INTRODUCTION.................................................................................................................8 1.1. Background .......................................................................................................................8 1.2 Overall Objective ..............................................................................................................8 1.2.1. Specific ...........................................................................................................................8 1.3. Background on the Progression of the 2006/07 Rain Season..............................................8 1.4. Limitations to the Assessment ...........................................................................................9 2.0 METHODOLOGY................................................................................................................9 3.0 FINDINGS......................................................................................................................... -

GOVERNMENT GAZETTE Price: K10.00 Net Annual Subscription: Within Lusaka—K3Q0.Q0 Published by Authority Outside Lusaka—K350.ÕÕ
REPUBLIC OF ZAMBIA GOVERNMENT GAZETTE Price: K10.00 net Annual Subscription: Within Lusaka—K3Q0.Q0 Published by Authority Outside Lusaka—K350.ÕÕ No. 6S45] Lusaka, Friday, 21§t February, 2020 [Vol LVI, No. 14 TABLE OF CONTENTS Gazette Notice No. 134 of 2019 [9181243 Gazette Notices No. Page Marriage Act—Appointment of Person to Solemnise The Companies Act Marriages 133 101 (Act No. 10 of 2017) Companies Act: Notice Under Section 318 134 101 Notice Linder Section 318 Notice Under Section 318 135 lOi Notice is hereby given that at the expiration of a period of three Notice Under Section 318 136 10! months after the publication of this notice, Zamcapitol Enterprises Notice Under Section 318 137 102 Limited, Company Registration No. 119700005694, incorporated in Notice Under Section 318 138 102 Zambia on 11 th day of May, 1970 and having its place of business at Notice Under Section 318 139 102 Notice Under Section 318 140! 02 P.O. Box 30278 will be struck-off the register of Companies pursuance Notice Under Section 318 141 102 to Section 318 of the Companies Act No. 10 of 2017 of the Laws of Notice Under Section 318 142 102 Zambia unless due cause is shown to the contrary. Notice Under Section 318 143 102 S. Zimba, Corporate Insolvency Act—Notice Under Section 5 144 102 P.O. Box 32020 Assistant Registrar, Commissioner for Oaths Act—Appointment of Lusaka for /Registrar, Commissioner for Oaths 145 103 14th February, 2020 Patents and Companies Lands and Deeds Registry Act: Registration Agency Notice of Intention to Issue Duplicate Document 146 103 Notice of Intention to Issue Duplicate Document 147 103 Gazette Notice No. -

The Impact of Cassava Growing in Luapula Valley, a Historical
THE IMPACT OF CASSAVA GROWING IN LUAPULA VALLEY, A HISTORICAL STUDY, 1900-1980 BY CHAMA KALUBA JICKSON A dissertation submitted to the University of Zambia in partial fulfilment of the requirements of the Degree of Master of Arts in History. THE UNIVERSITY OF ZAMBIA LUSAKA © 2016 DECLARATION I, Chama Kaluba Jickson, do hereby declare that this dissertation represents my own work; it has not been previously submitted for any degree at this or any other university; and does not incorporate any published work or material from another dissertation without citation. Signed: ............................................................. Date: ................................................................ i COPYRIGHT All rights reserved. No part of this dissertation may be reproduced or stored in any form or by any means without prior permission in writing from the author or the University of Zambia. ii APPROVAL This dissertation of CHAMA KALUBA JICKSON is approved as fulfilling the partial requirements for the award of the degree of Master of Arts in History by the University of Zambia. Signed: Date: ......................................................... ................................................ .......................................................... ................................................. .......................................................... ................................................. .......................................................... ................................................. iii ABSTRACT This -

Situation Report Last Updated: 9 Dec 2020
ZAMBIA Situation Report Last updated: 9 Dec 2020 HIGHLIGHTS (9 Dec 2020) The Ministry of Health has confirmed 17,916 COVID- 19 cases and 364 deaths as of 7 December. The number of districts reporting COVID-19 infections had increased from 68 in September to 96, as of 30 November. Education partners report that 16 per cent of nearly 39,000 learners in Eastern and Southern provinces have dropped a reading level during COVID-19 school closures.. The food security situation remains of major concern, Community sensitization on COVID-19 in Chawama Market amid a infestation of the African Migratory Locusts in in Lusaka. Photo: ©UNICEF/Mulikita 14 districts across Central, Southern and Western provinces. Nearly 2 million people are facing severe food insecurity between October 2020 and March 2021, despite increased crop production in most areas. KEY FIGURES FUNDING CONTACTS Laura Hastings 10.1M 6.2M $132.9M $66.2M Humanitarian Affairs Officer, Zambia people in need people targeted requested (May-Oct received [email protected] 2020) Guiomar Pau Sole 27 Head of Communications & Information partners operational 51.7% Management, Regional Office for funded Southern & Eastern Africa [email protected] INTERACTIVE (29 Oct 2020) Emergency Appeal Financial Tracking https://reports.unocha.org/en/country/zambia/ Page 1 of 15 Downloaded: 9 Dec 2020 ZAMBIA Situation Report Last updated: 9 Dec 2020 View this interactive graphic: https://bit.ly/ZambiaAppealFunding BACKGROUND (9 Dec 2020) Situation Overview Since the first case of COVID-19 on 18 March 2020, the Ministry of Health (MOH) has confirmed over 17,916 cases with 364 deaths (case fatality rate of 2 per cent) as of 7 December 2020. -
The Iccf Group Brochure Ed
THE ICCF GROUP BROCHURE ED. 2021-2022 INTERNATIONALCONSERVATION.ORG TABLE OF CONTENTS WHO WE ARE AND WHAT WE DO ................................................................ 4 WORKING WITH LEGISLATURES ..................................................................... 8 • Caucuses We Support ................................. 10 • ICCF in the United States ................................ 12 • The ICCF Group in the United Kingdom ......................................................................................................... 31 • The ICCF Group in Latin America & the Caribbean ...................................................................................... 39 • The ICCF Group in Africa ............................ 63 • The ICCF Group in Southeast Asia ................ 93 WORKING WITH MINISTRIES ....................................................................... 103 MISSION THE MOST ADVANCED WE WORK HOW TO ADVANCE SOLUTION IN CONSERVATION CONSERVATION GOVERNANCE GOVERNANCE BY BUILDING 1. WE BUILD POLITICAL WILL POLITICAL WILL, The ICCF Group advances leadership in conservation by building political will among parliamentary PROVIDING and congressional leaders, and by supporting ministries in the management of protected areas. ON-THE-GROUND SOLUTIONS 2. CATALYZING CHANGE WITH KNOWLEDGE & EXPERTISE We support political will to conserve natural resources by catalyzing strategic partnerships and knowledge sharing between policymakers and our extensive network. VISION 3. TO PRESERVE THE WORLD'S MOST CRITICAL LANDSCAPES -

Chililabombwe District Investment Profile
CHILILABOMBWE DISTRICT INVESTMENT PROFILE WELCOME TO CHILILABOMBWE HOME OF THE CROAKING FROG This profile give you an insight of Chililabombwe District. It demonstrates the investment poetical of the District and the comparative advantages with other Districts in the Province. Chililabombwe is predominantly a mining town. However, the District offers a lot of other economic activities that have high potential for growth. Apart from mining, Chililabombwe has a conducive climate and suitable land for agriculture, fish farming, beekeeping and other agricultural related activities. The District also has potential for Tourism, Small-scale Mining, Infrastructure development, Trade and many others. Therefore, investing in Chililabombwe is one of the wisest business decisions you will make due to the high demand for goods and services in Chililabombwe and Congo DR. Phone: +260977316767 E-mail: [email protected] Facebook: Chililabombwe Municipal Council Sincerely, Christabel M. Mulala Chililabombwe Mayor PO Box 210023 President Avenue Chililabombwe Page | 1 Table of Contents WELCOME TO CHILILABOMBWE ................................................................................................... 1 LIST OF TABLES .................................................................................................................................. 4 LIST OF FIGURES ................................................................................................................................ 4 ABBREVIATIONS ............................................................................................................................... -
Report20 Uniting to End Malaria 501(C)3
PHOTO BY PAUL ISHII ANNUAL REPORT20 Uniting to End Malaria 501(c)3. EIN: 46-1380419 No one can foresee the duration or severity of COVID’s human and economic toll. But the malaria global health community agrees it will be disastrous to neglect or underinvest in malaria during this period, and thereby squander a decade of hard won progress. By some estimates, halting malaria intervention efforts could trigger a return to one million malaria deaths per year, a devastating mortality rate unseen since 2004. To that end many of our efforts last year were to strategically advocate for continued global malaria funding, as well as supporting COVID adjustments to ensure malaria projects were not delayed. Last year we supplied Personal Protection Equipment (PPE) to over 700 Rotary-funded community health workers (CHWs) in Uganda and Zambia; altered CHW The training to incorporate appropriate social distancing; conducted several webinars specifically focused on maintaining malaria financial support despite COVID; and we provided $50,000 to the Alliance for Malaria Prevention used for COVID/malaria public education in Africa. Jeff Pritchard Board Chair While our near-term work must accommodate pandemic restrictions, we are still firmly committed to our mission, “to generate a broad international Rotary campaign for the global elimination of malaria.” During the coming twelve months we intend to: • Implement a blueprint developed in 2020 for a large long-term Road malaria program with Rotary, the Bill & Melinda Gates Foundation, and World Vision, in the most underserved regions of Zambia’s Central and Muchinga Provinces, positively impacting nearly 1.4 million residents. -

Provincial Health Literacy Training Report Northern and Muchinga Provinces
Provincial Health Literacy Training Report Northern and Muchinga Provinces AT MANGO GROVE LODGE, MPIKA, ZAMBIA 23-26TH APRIL 2013 Ministry of Health and Lusaka District Health Team, Zambia in association with Training and Research Support Centre (TARSC) Zimbabwe In the Regional Network for Equity in Health in east and southern Africa (EQUINET) With support from CORDAID 1 Table of Contents 1. Background ......................................................................................................................... 3 2. Opening .............................................................................................................................. 4 3. Ministry of Health and LDHMT ............................................................................................ 5 3.1 Background information on MOH ................................................................................. 5 3.2 Background on LDHMT ............................................................................................... 6 4. Using participatory approaches in health ............................................................................ 7 5. The health literacy programme ............................................................................................ 9 5.1 Overview of the Health literacy program ...................................................................... 9 5.2 Using the Zambia HL Manual ......................................................................................10 5.3 Social mapping ...........................................................................................................10 -

Zambia USADF Country Portfolio
Zambia USADF Country Portfolio Overview: Country program established in 1984 and reopened in U.S. African Development Foundation Partner Organization: Keepers Zambia 2004. USADF currently manages a portfolio of 23 projects and one Country Program Coordinator: Guy Kahokola Foundation (KZF) Cooperative Agreement. Total active commitment is $2.9 million. Suite 103 Foxdale Court Office Park Program Manager: Victor Makasa Agricultural investments total $2.6 million. Youth-led enterprise 609 Zambezi Road, Roma Tel: +260 211 293333 investments total $20,000. Lusaka, Zambia Email: [email protected] Email: [email protected] Country Strategy: The program focuses on support to agricultural enterprises, including organic farming as Zambia has been identified as a Feed the Future country. In addition, there are investments in off-grid energy and youth led-enterprises. Enterprise Duration Grant Size Description Mongu Dairy Cooperative Society 2012-2017 $152,381 Sector: Agriculture (Dairy) Limited Town/City: Mongu District in the Western Province 2705-ZMB Summary: The project funds will be used to increase the production and sales of milk through the purchase of improved breed cows, transportation, and storage equipment. Chibusa Home Based Care 2013-2018 $187,789 Sector: Agriculture (Food Processing) Association Town/City: Mungwi District in the Northern Province of Zambia 2925-ZMB Summary: The project funds will be used to provide working capital for purchasing grains, increase milling capacity, build a storage warehouse, and provide funds to improve marketing. Ushaa Area Farmers Association 2013-2018 $94,960 Sector: Agriculture (Rice) Limited Town/City: Mongu District in the Western Province of Zambia 2937-ZMB Summary: The project funds will be used to provide working capital for purchasing rice, build a storage warehouse, and provide funds to improve marketing. -

J:\Sis 2013 Folder 2\S.I. Provincial and District Boundries Act.Pmd
21st June, 2013 Statutory Instruments 397 GOVERNMENT OF ZAMBIA STATUTORY INSTRUMENT NO. 49 OF 2013 The Provincial and District Boundaries Act (Laws, Volume 16, Cap. 286) The Provincial and District Boundaries (Division) (Amendment)Order, 2013 IN EXERCISE of the powers contained in section two of the Provincial and District BoundariesAct, the following Order is hereby made: 1. This Order may be cited as the Provincial and District Boundaries (Division) (Amendment) Order, 2013, and shall be read Title as one with the Provincial and District Boundaries (Division) Order, 1996, in this Order referred to as the principal Order. S. I. No. 106 of 1996 2. The First Schedule to the principal Order is amended — (a) by the insertion, under Central Province, in the second Amendment column, of the following Districts: of First Schedule The Chisamba District; The Chitambo District; and The Luano District; (b) by the insertion, under Luapula Province, in the second column, of the following District: The Chembe District; (c) by the insertion, under Muchinga Province, in the second column, of the following District: The Shiwang’andu District; and (d) by the insertion, under Western Province, in the second column, of the following Districts: The Luampa District; The Mitete District; and The Nkeyema District. 3. The Second Schedule to the principal Order is amended— 398 Statutory Instruments 21st June, 2013 Amendment (a) under Central Province— of Second (i) by the deletion of the boundary descriptions of Schedule Chibombo District, Mkushi District and Serenje