Utilization of Out—Patient Clinics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mural Initiative Brochure Page1
mural initiative 2018 lebanon unrwa UNRWA Ein el Assal school compound, Rashidieh Palestine refugee camp, Tyre Each year since 2013, the UNRWA Operations Support Office Between October 2017 and November 2018, Palestine refugee team (OSO) in Lebanon has taken the lead on initiatives to paint children painted the walls of 14 UNRWA installations including 9 colourful murals on the walls of UNRWA installations in schools, 2 camp services office, 2 health clinic and 1 water tank Palestine refugee camps across Lebanon. Through these and sanitation office across 6 Palestine refugee camps in murals, the initiative aims to promote creativity in portraying Lebanon; Ein el Hilweh camp, Rashidieh camp, Beddawi camp, positive messages, to increase community engagement in Burj el Barajneh camp, Mar Elias camp and Wavel camp. relation to the camp environment, and in addition preserving the neutrality of UNRWA installations in the camps and gatherings. This document enlists the 2018 mural initiatives completed in the four areas of operation in Lebanon (North Lebanon, Central The mural painting included positive messaging related to water, Lebanon, Tyre and Saida) to address neutrality issues in the sanitation and hygiene, sports, inclusion of all communities, following installations: four UNRWA Schools (Sammou, Bissan, friendship and peace. Artists from the community were selected Safad and Naqoura) in Ein el Hilweh Palestine refugee camp, by UNRWA OSO teams to design mural paintings, with the involve- Saida; UNRWA health clinic in Rashidieh Palestine refugee ment of Palestine refugees in Lebanon (PRL) and Palestinian camp, Tyre; UNRWA Ein el Assal school in Rashidieh Palestine refugees from Syria (PRS) children to decide on the themes and refugee camp, Tyre; UNRWA Majeddo and Mazar schools in designs. -

Survey of Palestinian Refugees and Internally Displaced Persons 2010 - 2012 Volume VII
BADIL Resource Center for Palestinian Residency and Refugee Rights is an independent, community-based non- This edition of the Survey of Palestinian Survey of Palestinian Refugees and profit organization mandated to defend Refugees and Internally Displaced Persons BADIL Internally Displaced Persons 2010-2012 and promote the rights of Palestinian (Volume VII) focuses on Palestinian Vol VII 2010-2012 refugees and Internally Displaced Persons Survey of refugees and IDPs. Our vision, mission, 124 Pages, 30 c.m. (IDPs) in the period between 2010 and ISSN: 1728-1679 programs and relationships are defined 2012. Statistical data and estimates of the by our Palestinian identity and the size of this population have been updated Palestinian Refugees principles of international law, in in accordance with figures as of the end Editor: Nidal al-Azza particular international human rights of 2011. This edition includes for the first law. We seek to advance the individual time an opinion poll surveying Palestinian Editorial Team: Amjad Alqasis, Simon and collective rights of the Palestinian refugees regarding specific humanitarian and Randles, Manar Makhoul, Thayer Hastings, services they receive in the refugee Noura Erakat people on this basis. camps. Demographic Statistics: Mustafa Khawaja BADIL Resource Center was established The need to overview and contextualize in January 1998. BADIL is registered Palestinian refugees and (IDPs) - 64 Internally Displaced Persons Layout & Design: Atallah Salem with the Palestinan Authority and years since the Palestinian Nakba Printing: Al-Ayyam Printing, Press, (Catastrophe) and 45 years since Israel’s legally owned by the refugee community Publishing and Distribution Conmpany represented by a General Assembly belligerent occupation of the West Bank, including eastern Jerusalem, and the 2010 - 2012 composed of activists in Palestinian Gaza Strip - is derived from the necessity national institutions and refugee to set the foundations for a human rights- community organizations. -

Israeli Human Rights Violations and Hamas Support Ii Preface
IIssrraaeellii HHuummaann RRiigghhttss VViioollaattiioonnss aanndd HHaammaass SSuuppppoorrtt RReesseeaarrcchhiiinngg PPeerrcceeppttiiioonnss ooff PPaallleessttiiinniiiaann rreeffuuggeeeess iiinn JJoorrddaann Lidwien Wijchers IIssrraaeellii HHuummaann RRiigghhttss VViioollaattiioonnss aanndd HHaammaass SSuuppppoorrtt RReesseeaarrcchhiiinngg PPeerrcceeppttiiioonnss ooff PPaallleessttiiinniiiaann rreeffuuggeeeess iiinn JJoorrddaann Cover photo Lidwien Wijchers Banner in Irbid refugee camp, Jordan: “The Palestinian case and Jerusalem are always in the heart and consciousness of his Majesty the King” Lidwien Wijchers s0801240 Master Thesis Human Geography Center for International Conflict Analysis and Management Radboud University Nijmegen Supervisor: Dr. S. Vukovic Second Reader: Dr. J. Wagemakers July 2013 Israeli Human Rights Violations and Hamas Support ii Preface This thesis is submitted as part of the Human Geography Master specialization Conflicts, Identities, and Territories at the Center of International Conflict Analysis and Management associated with the Radboud University Nijmegen. It is the result of fieldwork conducted in Jordan from August 2012 until March 2013. Throughout the process of writing this thesis, many people have been of help to me. Not in the least the respondents of my questionnaire, and experts with whom I conducted interviews. I hereby express my appreciation to all of them. Furthermore, I would like to extend gratitude to Dr. Siniša Vukovic who supervised me through the writing stages of the thesis, and to my second reader Dr. Joas Wagemakers. Acknowledgment must also be given to Dr. Gearoid Millar, for his guidance in the initial stages of the project. Four other individuals deserve recognition. Lauren Salathiel and Mohamed el Atfy; thank you for your willingness to be sounding boards. Hashim Taani and Rakan Odeh, I am much indebted to you both for the amount of time and help you have selflessly given. -

People's Perceptions from Jabal El-Hussein to Zarqa Camps. An
Centre for Middle Eastern Studies People’s perceptions from Jabal el-Hussein to Zarqa camps. An analysis of access to water and inequalities in two Palestinian refugee camps of the Hashemite Kingdom of Jordan Thesis submitted in partial fulfillment of the requirements of the degree of Master of Arts in Middle Eastern Studies Author: Giorgia Gusciglio Advisor: Lina Eklund Examiner: Date: Spring 2018 1 Acknowledgments The accomplishment and realization of this thesis was possible thanks to the support of a variety of people who believed in me, not only during this last step towards finishing my studies, but throughout all my life. First and foremost, my parents and my sister Michela who have been accepting all the crazy choices I made, although with a bit of concern. I am deeply grateful for the sacrifices my parents did and their valuable guidance. I am deeply thankful for my grandparents, two of them left us last year, but the teachings and love they gave me will stay with me forever. To my big family goes all my love. To my best friends, Aurora and Mariavittoria, whose constant love, support and acceptance of who I am, despite time changed us, make me believe in true friendship. To Beatrice, Francesca and Marta, thank you for three beautiful years in Trento and for your friendship, contact and care since then, despite distance and Italian trains connections. This achievement was also possible thanks to those people I met since I started the Master at the Center for Middle Eastern Studies at Lund University. The same interest and struggles we faced has brought us together, but what we built, I hope, is a long-lasting friendship. -
University of Cincinnati
U UNIVERSITY OF CINCINNATI Date: 05-20-2009 I, Shadi Y. Saleh , hereby submit this original work as part of the requirements for the degree of: Master in Architecture It is entitled: Designing by Community Participation: Meeting the Challenges of the Palestinian Refugee Camps Shadi Saleh Student Signature: This work and its defense approved by: Committee Chair: Elizabeth Riorden Thomas Bible Approval of the electronic document: I have reviewed the Thesis/Dissertation in its final electronic format and certify that it is an accurate copy of the document reviewed and approved by the committee. Committee Chair signature: Elizabeth Riorden Designing by Community Participation: Meeting the Challenges of the Palestinian Refugee Camps A thesis submitted to the Division of Research and Advance Studies of the University of Cincinnati in partial fulfillment of the requirements of the degree of Master of Architecture In the school of Architecture and Interior design Of the College of Design, Architecture, Art and Planning 2009 By Shadi Y. Saleh Committee chair Elizabeth Riorden Thomas Bible ABSTRACT Palestinian refugee camps in the West Bank, Gaza Strip, Jordan, Lebanon and Syria are the result of the sudden population displacements of 1948 and 1967. After 60 years, unorganized urban growth compounds the situation. The absence of state support pushed the refugees to take matters into their own hands. Currently the camps have problems stemming from both the social situation and the degradation of the built environment. Keeping the refugee camps in order to “represent” a nation in exile does not mean to me that there should be no development. The thesis seeks to make a contribution in solving the social and environmental problems in a way that emphasizes the Right of Return. -

Towards a Global Movement: a Framework for Today’S Anti-Apartheid Activism
Grassroots Palestinian Anti-Apartheid Wall Campaign Towards a Global Movement: A framework for today’s anti-apartheid activism June 2007 ii Abstract Building and strengthening a global boycott, divestment and sanctions (BDS) movement has become a core aim for many involved in today’s solidarity work for Palestine. This report assesses the current state of the BDS movements – within the general context of Palestine solidarity work – and makes recommendations for improvement. Developing clarity, cohesion and coordination across the numerous local and national initiatives, campaigns and movements from around the world is crucial if solidarity is to be more effective. Our discussion and framework for action explores the central issues pertaining to any BDS strategy and sets out how global activism can have an important role to play in advancing the Palestinian cause and struggle. Reflections upon previous BDS strategies used to isolate Israel, from within and outside the Middle East, are explored together with a comprehensive study of the campaigns pursued by the anti-apartheid movement against South Africa. An evaluation seeks to learn from past BDS experiences and the implications for Palestine campaign work today. The findings are addressed to solidarity movements, trade unions and social justice organizations around the world, with the intention of creating stronger global networks and alliances with Palestine at a grassroots and civil society level. Moreover, they build upon the Palestinian Call (2005) for BDS as a means of support for -

Draft Chapter 1
UvA-DARE (Digital Academic Repository) Palestine online : cyber Intifada and the construction of a virtual community 2001-2005 Aouragh, M. Publication date 2008 Document Version Final published version Link to publication Citation for published version (APA): Aouragh, M. (2008). Palestine online : cyber Intifada and the construction of a virtual community 2001-2005. General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl) Download date:07 Oct 2021 Palestine Online Dit proefschrift werd mogelijk gemaakt met de financiële steun van: Amsterdam School voor Social Science Research (ASSR) Netherlands Organisation for Scientific Research (NWO) Netherlands Foundation for the Advancement of Tropical Research (WOTRO) Palestine Online Cyber Intifada and the Construction of a Virtual Community 2001-2005 ACADEMISCH PROEFSCHRIFT ter verkrijging van de graad van doctor aan de Universiteit van Amsterdam op gezag van de Rector Magnificus prof. -

Beit Sahour City Profile
Beit Sahour City Profile Prepared by The Applied Research Institute – Jerusalem Funded by Spanish Cooperation Azahar Program 2010 Palestinian Localities Study Bethlehem Governorate Acknowledgments ARIJ hereby expresses its deep gratitude to the Spanish agency for International Cooperation for Development (AECID) for their funding of this project through the Azahar Program. ARIJ is grateful to the Palestinian officials in the ministries, municipalities, joint services councils, village committees and councils, and the Palestinian Central Bureau of Statistics (PCBS) for their assistance and cooperation with the project team members during the data collection process. ARIJ also thanks all the staff who worked throughout the past couple of years towards the accomplishment of this work. 1 Palestinian Localities Study Bethlehem Governorate Background This booklet is part of a series of booklets, which contain compiled information about each city, town, and village in Bethlehem Governorate. These booklets came as a result of a comprehensive study of all localities in Bethlehem Governorate, which aims at depicting the overall living conditions in the governorate and presenting developmental plans to assist in developing the livelihood of the population in the area. It was accomplished through the "Village Profiles and Azahar Needs Assessment;" the project funded by the Spanish Agency for International Cooperation for Development (AECID) and the Azahar Program. The "Village Profiles and Azahar Needs Assessment" was designed to study, investigate, analyze and document the socio-economic conditions and the needed programs and activities to mitigate the impact of the current unsecure political, economic and social conditions in Bethlehem Governorate with particular focus on the Azahar program objectives and activities concerning water, environment, and agriculture. -

Nablus City Profile
Nablus City Profile Prepared by The Applied Research Institute – Jerusalem Funded by Spanish Cooperation 4102 Palestinian Localities Study Nablus Governorate Acknowledgments ARIJ hereby expresses its deep gratitude to the Spanish Agency for International Cooperation for Development (AECID) for their funding of this project. ARIJ is grateful to the Palestinian officials in the ministries, municipalities, joint services councils, village committees and councils, and the Palestinian Central Bureau of Statistics (PCBS) for their assistance and cooperation with the project team members during the data collection process. ARIJ also thanks all the staff who worked throughout the past couple of years towards the accomplishment of this work. 1 Palestinian Localities Study Nablus Governorate Background This report is part of a series of booklets which contain compiled information about each city, town, and village in the Nablus Governorate. These booklets came as a result of a comprehensive study of all localities in the Nablus Governorate, and aim to depict the overall living conditions in the governorate and presenting developmental plans to assist in improving the livelihood of the population in the area. It was accomplished through the "Village Profiles and Needs Assessment" project funded by the Spanish Agency for International Cooperation for Development (AECID). The "Village Profiles and Needs Assessment" was designed to study, investigate, analyze and document the socio-economic conditions and the programs and activities needed to mitigate the impact of the current insecure political, economic and social conditions in the Nablus Governorate. The project's objectives are to survey, analyze and document the available natural, human, socioeconomic and environmental resources, and the existing limitations and needs assessment for the development of the rural and marginalized areas in the Nablus Governorate. -

Nablus Salfit Tubas Tulkarem
Iktaba Al 'Attara Siris Jaba' (Jenin) Tulkarem Kafr Rumman Silat adh DhahrAl Fandaqumiya Tubas Kashda 'Izbat Abu Khameis 'Anabta Bizzariya Khirbet Yarza 'Izbat al Khilal Burqa (Nablus) Kafr al Labad Yasid Kafa El Far'a Camp Al Hafasa Beit Imrin Ramin Ras al Far'a 'Izbat Shufa Al Mas'udiya Nisf Jubeil Wadi al Far'a Tammun Sabastiya Shufa Ijnisinya Talluza Khirbet 'Atuf An Naqura Saffarin Beit Lid Al Badhan Deir Sharaf Al 'Aqrabaniya Ar Ras 'Asira ash Shamaliya Kafr Sur Qusin Zawata Khirbet Tall al Ghar An Nassariya Beit Iba Shida wa Hamlan Kur 'Ein Beit el Ma Camp Beit Hasan Beit Wazan Ein Shibli Kafr ZibadKafr 'Abbush Al Juneid 'Azmut Kafr Qaddum Nablus 'Askar Camp Deir al Hatab Jit Sarra Salim Furush Beit Dajan Baqat al HatabHajja Tell 'Iraq Burin Balata Camp 'Izbat Abu Hamada Kafr Qallil Beit Dajan Al Funduq ImmatinFar'ata Rujeib Madama Burin Kafr Laqif Jinsafut Beit Furik 'Azzun 'Asira al Qibliya 'Awarta Yanun Wadi Qana 'Urif Khirbet Tana Kafr Thulth Huwwara Odala 'Einabus Ar Rajman Beita Zeita Jamma'in Ad Dawa Jafa an Nan Deir Istiya Jamma'in Sanniriya Qarawat Bani Hassan Aqraba Za'tara (Nablus) Osarin Kifl Haris Qira Biddya Haris Marda Tall al Khashaba Mas-ha Yasuf Yatma Sarta Dar Abu Basal Iskaka Qabalan Jurish 'Izbat Abu Adam Talfit Qusra Salfit As Sawiya Majdal Bani Fadil Rafat (Salfit) Khirbet Susa Al Lubban ash Sharqiya Bruqin Farkha Qaryut Jalud Kafr ad Dik Khirbet Qeis 'Ammuriya Khirbet Sarra Qarawat Bani Zeid (Bani Zeid al Gharb Duma Kafr 'Ein (Bani Zeid al Gharbi)Mazari' an Nubani (Bani Zeid qsh Shar Khirbet al Marajim 'Arura (Bani Zeid qsh Sharqiya) Bani Zeid 'Abwein (Bani Zeid ash Sharqiya) Sinjil Turmus'ayya. -

Urban Planning Analyses of Refugee Camps, Jabalia As Case Study-Gaza Strip, Palestine
International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064 Index Copernicus Value (2013): 6.14 | Impact Factor (2015): 6.391 Urban Planning Analyses of Refugee Camps, Jabalia as Case Study-Gaza Strip, Palestine Dr. Usama Ibrahim Badawy1, Dr Ra’ed A. Salha2, Dr. Muain Qasem Jawabrah3, Amjad Jarada4 Mohammed A. EL Hawajri5 1Former Professor of Architecture, Birzeit University Palestine, works currently at UNRWA 2Assistant Professor, Islamic University of Gaza in Geography and GIS Palestine 3Assistance Professor, Architecture Department, Birzeit University Palestine 4Researcher in Infrastructure Planning and Development works currently at UNRWA, G, 5Researcher Geography subjects, works currently as teacher by the Ministry of Education Abstract: The Gaza Strip is a tight area with more than 1.8 million inhabitants. Since the beginning of the last century, and as other Palestinian areas, Gaza Strip was subject to direct occupation. The occupation tightened laws and regulations and increased obstacles, meanwhile it established settlements in a method that besieges existing Palestinian urban areas and leads them to develop in a way that serves the occupation, particularly the security side. This research begins with background information on Palestinian refugees in Gaza, sees that camp Improvement Strategies should called for adoption of the future urban planning, increasing the accommodation capacity of the built-up area, activating the environmental resources protection laws and played down the issue of the land properties when preparing the comprehensive plans. In this study reviews options for addressing the problems faced by Palestinian refugees in Gaza, Recommendations: After discussing the topic through a analyses of the Current Conditions , Land availability, Population distribution, Land requirements, Overcrowding, Public Spaces problems inside the camps , Sustainability in Gaza Strip, socio-economic situation , Unemployment problem and Population density in Jabalia Camp. -
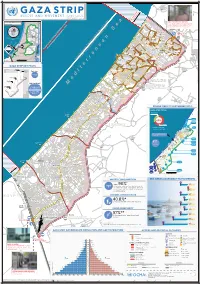
Gaza CRISIS)P H C S Ti P P I U
United Nations Office for the Coordination of Humanitarian Affairs occupied Palestinian territory Zikim e Karmiya s n e o il Z P m A g l in a AGCCESSA ANDZ AMOV EMENTSTRI (GAZA CRISIS)P h c s ti P P i u F a ¥ SEPTEMBER 2014 o nA P N .5 F 1 Yad Mordekhai EREZ CROSSING (BEIT HANOUN) occupied Palestinian territory: ID a As-Siafa OPEN, six days (daytime) a B?week4 for B?3the4 movement d Governorates e e of international workers and limited number of y h s a b R authorized Palestinians including aid workers, medical, P r 2 e A humanitarian cases, businessmen and aid workers. Jenin d 1 e 0 Netiv ha-Asara P c 2 P Tubas r Tulkarm r fo e S P Al Attarta Temporary Wastewater P n b Treatment Lagoons Qalqiliya Nablus Erez Crossing E Ghaboon m Hai Al Amal r Fado's 4 e B? (Beit Hanoun) Salfit t e P P v i Al Qaraya al Badawiya i v P! W e s t R n m (Umm An-Naser) n i o » B a n k a North Gaza º Al Jam'ia ¹¹ M E D I TER RAN EAN Hatabiyya Ramallah da Jericho d L N n r n r KJ S E A ee o Beit Lahia D P o o J g Wastewater Ed t Al Salateen Beit Lahiya h 5 Al Kur'a J a 9 P l D n Treatment Plant D D D D 9 ) D s As Sultan D 1 2 El Khamsa D " Sa D e J D D l i D 0 D s i D D 0 D D d D D m 2 9 Abedl Hamaid D D r D D l D D o s D D a t D D c Jerusalem D D c n P a D D c h D D i t D D s e P! D D A u P 0 D D D e D D D a l m d D D o i t D D l i " D D n .