Skin Rashes That Involve Palms and Soles: an Internist’S View
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Idiopathic Spiny Keratoderma: a Report of Two Cases and Literature Review
Idiopathic Spiny Keratoderma: A Report of Two Cases and Literature Review Jessica Schweitzer, DO,* Matthew Koehler, DO,** David Horowitz, DO*** *Intern, Largo Medical Center, Largo, FL **Dermatology Resident, Third Year, College Medical Center/Western University, Long Beach, CA ***Dermatology Residency Program Director, College Medical Center/Western University, Long Beach, CA Abstract Spiny keratoderma is a rare and likely underreported condition that presents with punctate hyperkeratotic growths localized to the palms and soles. We present two cases of clinically diagnosed spiny keratoderma. Although the lesions were asymptomatic, patients are at risk of an underlying internal malignancy with this condition, so diagnosis is crucial. Neither men were seeking treatment for the lesions when they were discovered, suggesting that this condition may be much more common than reported. Patients with histories of manual labor, increased UV exposure, and non-melanoma skin cancer (NMSC) may also be at higher risk for developing spiny keratoderma.1 The epidemiology, histopathologic features, differential diagnosis, and current treatments for spiny keratoderma are reviewed. Introduction Case 2 enthusiast for his entire life, spending significant Spiny keratoderma is a rare palmoplantar A 67-year-old Caucasian male presented with a time using his hands to maintain and fire his keratoderma that presents with keratotic, pinpoint one-year history of insidiously growing, pinpoint weapons and many hours outside without sun papules on the palms and soles. There are both hyperkeratotic papules projecting from his palms protection. The patient was referred back to his hereditary and acquired forms. When found, bilaterally (Figures 4-5). He presented to the clinic primary care physician for internal evaluation. -
Infectious Eccrine Hidradenitis Associated with Intense Sun Exposure
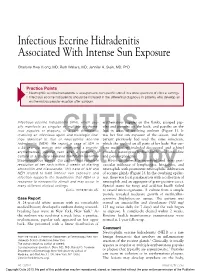
Infectious Eccrine Hidradenitis Associated With Intense Sun Exposure Charlotte Hwa Vuong, MD; Ruth Walters, MD; Jennifer A. Stein, MD, PhD Practice Points Neutrophilic eccrine hidradenitis is a response to nonspecific stimuli in a wide spectrum of clinical settings. Infectious eccrine hidradenitis should be included in the differential diagnosis in patients who develop an erythematous papular eruption after sunburn. Infectious eccrine hidradenitis (IEH), which usu- erythematous papules on the flanks, grouped pap- ally manifests as singular or multiple erythema- ules and pustules on the back, and papules on the tous papules or plaques, is a rare dermatosis legs in areas of resolving sunburn (Figure 1). It involving an infectious agent and histologic find- was her first sun exposure of the season, and the ings identical to that of CUTISneutrophilic eccrine patient previously had used the same sunscreen, hidradenitis (NEH). We report a case of IEH in which she applied on all parts of her body. Her cur- a 24-year-old woman who developed a pruritic, rent medications included desogestrel and ethinyl erythematous, papular rash after a sunburn. A estradiol, naratriptan hydrochloride, and loratadine culture of a pustule revealed methicillin-sensitive and pseudoephedrine. Staphylococcus aureus. Our patient had complete Histology showed a superficial and deep peri- resolution of her rash within 2 weeks of starting vascular infiltrate of lymphocytes, histiocytes, and amoxicillinDo and clavulanate. ThisNot case of IEH and neutrophils Copy with prominent neutrophilic infiltration NEH related to both intense sun exposure and of eccrine glands (Figure 2). In the overlying epider- infection supports the hypothesis that NEH is a mis, there was focal parakeratosis with a collection of response to nonspecific stimuli and may occur in neutrophils and an aggregate of gram-positive cocci. -

Parinaud's Oculoglandular Syndrome
Tropical Medicine and Infectious Disease Case Report Parinaud’s Oculoglandular Syndrome: A Case in an Adult with Flea-Borne Typhus and a Review M. Kevin Dixon 1, Christopher L. Dayton 2 and Gregory M. Anstead 3,4,* 1 Baylor Scott & White Clinic, 800 Scott & White Drive, College Station, TX 77845, USA; [email protected] 2 Division of Critical Care, Department of Medicine, University of Texas Health, San Antonio, 7703 Floyd Curl Drive, San Antonio, TX 78229, USA; [email protected] 3 Medical Service, South Texas Veterans Health Care System, San Antonio, TX 78229, USA 4 Division of Infectious Diseases, Department of Medicine, University of Texas Health, San Antonio, 7703 Floyd Curl Drive, San Antonio, TX 78229, USA * Correspondence: [email protected]; Tel.: +1-210-567-4666; Fax: +1-210-567-4670 Received: 7 June 2020; Accepted: 24 July 2020; Published: 29 July 2020 Abstract: Parinaud’s oculoglandular syndrome (POGS) is defined as unilateral granulomatous conjunctivitis and facial lymphadenopathy. The aims of the current study are to describe a case of POGS with uveitis due to flea-borne typhus (FBT) and to present a diagnostic and therapeutic approach to POGS. The patient, a 38-year old man, presented with persistent unilateral eye pain, fever, rash, preauricular and submandibular lymphadenopathy, and laboratory findings of FBT: hyponatremia, elevated transaminase and lactate dehydrogenase levels, thrombocytopenia, and hypoalbuminemia. His condition rapidly improved after starting doxycycline. Soon after hospitalization, he was diagnosed with uveitis, which responded to topical prednisolone. To derive a diagnostic and empiric therapeutic approach to POGS, we reviewed the cases of POGS from its various causes since 1976 to discern epidemiologic clues and determine successful diagnostic techniques and therapies; we found multiple cases due to cat scratch disease (CSD; due to Bartonella henselae) (twelve), tularemia (ten), sporotrichosis (three), Rickettsia conorii (three), R. -

Living with Mast Cell Activation Syndrome
Anne Maitland, MD, PhD Living with Medical Director, Comprehensive Allergy Mast Cell & Asthma Care Activation Asst Professor, Dept of Medicine – Clinical Immunology Syndrome Icahn School of Medicine at Mt Sinai, New York Got MCAS? Mast Cell mediated disorders are common u 1 out of 2 of us are coping with some chronic immune mediated disorder. o ‘allergies’(rhinitis), sinus infections, hives (urticaria),food allergy/intolerance, skin swelling (angioedema), Anaphylaxis Signs and Symptoms eczema (atopic dermatitis and contact dermatitis), asthma issues, and the prototype of immediate hypersensitivity syndromes, anaphylaxis Why the rise in hypersensitivity disorders? Our genes in this environment! The human race has come to dominate its environment so completely that any analysis of the increase or appearance of a disease has to take changes in our lifestyle into account. In the case of allergic disease [hypersensitivity disorders] changes in our environment, diet, water quality, and personal behavior over the last 150 years have played a dominant role in the specificity of these diseases, as well as in prevalence and severity… it is clear that the consequences of hygiene, indoor entertainment, and changes in diet or physical activity have never been predicted. Thomas A. E. Platts-Mills, MD, PhD, FRS, The allergy epidemics: 1870-2010; J Allergy Clin Immunol 2015;136:3-13. Why? Trauma Stress Infection Connective Tissue Chemical Disorder exposure PIDD -manufactured Autoimmune Dz. -mold, Mastocytosis mycotoxins Hypertryptasemia (naturally Atopic Disorders occuring) Mast cell activation syndrome is easily treated, if it's But most patients with recognized MCAD suffer for Patients with mast cell activation syndrome (MCAS) frequently go for years without an accurate diagnosis… Harding, Reuters Health-New York, 2011 years… It is very common for one hypersensitivity condition to progress/morph into another, be provoked by more triggers. -

Neonatal Dermatology Review
NEONATAL Advanced Desert DERMATOLOGY Dermatology Jennifer Peterson Kevin Svancara Jonathan Bellew DISCLOSURES No relevant financial relationships to disclose Off-label use of acitretin in ichthyoses will be discussed PHYSIOLOGIC Vernix caseosa . Creamy biofilm . Present at birth . Opsonizing, antibacterial, antifungal, antiparasitic activity Cutis marmorata . Reticular, blanchable vascular mottling on extremities > trunk/face . Response to cold . Disappears on re-warming . Associations (if persistent) . Down syndrome . Trisomy 18 . Cornelia de Lange syndrome PHYSIOLOGIC Milia . Hard palate – Bohn’s nodules . Oral mucosa – Epstein pearls . Associations . Bazex-Dupre-Christol syndrome (XLD) . BCCs, follicular atrophoderma, hypohidrosis, hypotrichosis . Rombo syndrome . BCCs, vermiculate atrophoderma, trichoepitheliomas . Oro-facial-digital syndrome (type 1, XLD) . Basal cell nevus (Gorlin) syndrome . Brooke-Spiegler syndrome . Pachyonychia congenita type II (Jackson-Lawler) . Atrichia with papular lesions . Down syndrome . Secondary . Porphyria cutanea tarda . Epidermolysis bullosa TRANSIENT, NON-INFECTIOUS Transient neonatal pustular melanosis . Birth . Pustules hyperpigmented macules with collarette of scale . Resolve within 4 weeks . Neutrophils Erythema toxicum neonatorum . Full term . 24-48 hours . Erythematous macules, papules, pustules, wheals . Eosinophils Neonatal acne (neonatal cephalic pustulosis) . First 30 days . Malassezia globosa & sympoidalis overgrowth TRANSIENT, NON-INFECTIOUS Miliaria . First weeks . Eccrine -

Dermatologic Manifestations and Complications of COVID-19
American Journal of Emergency Medicine 38 (2020) 1715–1721 Contents lists available at ScienceDirect American Journal of Emergency Medicine journal homepage: www.elsevier.com/locate/ajem Dermatologic manifestations and complications of COVID-19 Michael Gottlieb, MD a,⁎,BritLong,MDb a Department of Emergency Medicine, Rush University Medical Center, United States of America b Department of Emergency Medicine, Brooke Army Medical Center, United States of America article info abstract Article history: The novel coronavirus disease of 2019 (COVID-19) is associated with significant morbidity and mortality. While Received 9 May 2020 much of the focus has been on the cardiac and pulmonary complications, there are several important dermato- Accepted 3 June 2020 logic components that clinicians must be aware of. Available online xxxx Objective: This brief report summarizes the dermatologic manifestations and complications associated with COVID-19 with an emphasis on Emergency Medicine clinicians. Keywords: COVID-19 Discussion: Dermatologic manifestations of COVID-19 are increasingly recognized within the literature. The pri- fi SARS-CoV-2 mary etiologies include vasculitis versus direct viral involvement. There are several types of skin ndings de- Coronavirus scribed in association with COVID-19. These include maculopapular rashes, urticaria, vesicles, petechiae, Dermatology purpura, chilblains, livedo racemosa, and distal limb ischemia. While most of these dermatologic findings are Skin self-resolving, they can help increase one's suspicion for COVID-19. Emergency medicine Conclusion: It is important to be aware of the dermatologic manifestations and complications of COVID-19. Knowledge of the components is important to help identify potential COVID-19 patients and properly treat complications. © 2020 Elsevier Inc. -

(Scrub Typhus). Incubation Period 1 to 3
TYPHUS Causative Agents TYPHUS Rickettsia typhi (murine typhus) and Orientia tsutsugamushi (scrub typhus). Causative Agents IncubationRickettsia typhi Period (murine typhus) and Orientia tsutsugamushi (scrub typhus). 1 to 3 weeks Incubation Period Infectious1 to 3 weeks Period Zoonoses with no human-to-human transmission. Infectious Period TransmissionZoonoses with no human-to-human transmission. Scrub typhus: Bite of grass mites (larval trombiculid mites) MurineTransmission typhus: Bite of rat fleas (also cat and mice fleas) RodentsScrub typhus: are the Bite preferred of grass and mites normal (larval hosts. trombiculid mites) Murine typhus: Bite of rat fleas (also cat and mice fleas) EpidemiologyRodents are the preferred and normal hosts. Distributed throughout the Asia-Pacific rim and is a common cause of pyrexia of unknownEpidemiology origin throughout SE Asia. Occupational contact with rats (e.g. construDistributedction throughout workers inthe makeAsia-Pshiftacific container rim and isfacilities, a common shop cause owners, of pyrexia granary of workers,unknown andorigin garbage throughout collectors) SE orAsia. exposure Occupational to mite habitat contacts in lonwithg grassrats (e.g. hikersconstru andction so ldiers)workers are inrisk make factors.-shift container facilities, shop owners, granary workers, and garbage collectors) or exposure to mite habitats in long grass (e.g. Inhikers Singapore, and soldiers) a total are ofrisk 13 factors. laboratory confirmed cases of murine typhus were r eported in 2008. The majority of cases were foreign workers. In Singapore, a total of 13 laboratory confirmed cases of murine typhus were Clinicalreported Featuresin 2008. The majority of cases were foreign workers. Fever Clinical Headache Features (prominent) MyalgiaFever ConjunctiHeadache val(prominent) suffusion MaculopapularMyalgia rash Conjunctival suffusion Scrub Maculopapular typhus may alsorash have: relative bradycardia, eschar (80%), painful regional adenopathy, hepatosplenomegaly, meningoencephalitis and renal failure. -

Palmoplantar Keratoderma with Progressive Gingivitis and Recurrent Pyodermas
Palmoplantar Keratoderma With Progressive Gingivitis and Recurrent Pyodermas Tyler A. Moss, DO; Anne P. Spillane, MD; Sam F. Almquist, MD; Patrick E. McCleskey, MD; Oliver J. Wisco, DO Practice Points Papillon-Lefèvre syndrome (PLS) is an autosomal-recessive inherited transgredient palmoplantar kerato- derma (PPK) that is associated with gingivitis and recurrent pyodermas. The symptoms associated with PLS are thought to be due to cathepsin C gene, CTSC, mutations. CTSC is expressed in epithelial regions commonly affected by PLS and also plays a role in the activation of immune and inflammatory responses. Papillon-Lefèvre syndrome must be differentiated from other conditions causing PPK, such as Haim-Munk syndrome, Greither syndrome, mal de Meleda, Clouston syndrome, Vohwinkel syndrome, and Olmsted syndrome. Treatment of PLS includesCUTIS keratolytics such as urea and/or salicylic acid comb ined with oral retinoids. Active gingivitis may be treated with combined use of amoxicillin and metronidazole. Papillon-Lefèvre syndrome (PLS) is a rare inher- Case Report ited palmoplantar keratoderma (PPK) that is asso- A 30-year-old woman presented to the dermatology ciated with progressive gingivitis and recurrent clinic with erythematous hyperkeratotic plaques on pyodermas.Do We present a caseNot exhibiting classic the palmsCopy and soles. The plaques extended onto features of this autosomal-recessive condition the dorsal aspects of the fingers, toes, hands, and and review the current understanding of its patho- feet (Figures 1 and 2). The patient had psoriasiform physiology, diagnosis, and treatment. Addition- plaques on the extensor surfaces of the knees and ally, a review of pertinent transgredient PPKs is elbows (Figure 3) along with a history of slow- undertaken, with key and distinguishing features progressing gingivitis and periodontal disease that of each syndrome highlighted. -

HIV and the SKIN • Sudden Acute Exacerbations • Treatment Failure DR
2018/08/13 KEY FEATURES • Atypical presentation of common disorders • Severe or exaggerated presentations HIV AND THE SKIN • Sudden acute exacerbations • Treatment failure DR. FREDAH MALEKA DERMATOLOGY UNIVERSITY OF PRETORIA:KALAFONG VIRAL INFECTIONS EXANTHEM OF PRIMARY HIV INFECTION • Exanthem of primary HIV infection • Acute retroviral syndrome • Herpes simplex virus (HSV) • Morbilliform rash (exanthem) : 2-4 weeks after HIV exposure • Varicella Zoster virus (VZV) • Typically generalised • Molluscum contagiosum (Poxvirus) • Pronounced on face and trunk, sparing distal extremities • Human papillomavirus (HPV) • Associated : fever, lymphadenopathy, pharyngitis • Epstein Barr virus (EBV) • DDX: drug reaction • Cytomegalovirus (CMV) • other viral infections – EBV, Enteroviruses, Hepatitis B virus 1 2018/08/13 HERPES SIMPLEX VIRUS(HSV) • Vesicular eruption due to HSV 1&2 • Primary lesion: painful, grouped vesicles on an erythematous base • HIV: attacks are more frequent and severe • : chronic, non-healing, deep ulcers, with scarring and tissue destruction • CLUE: severe pain and recurrences • DDX: syphilis, chancroid, lymphogranuloma venereum • Tzanck smear, Histology, Viral culture HSV • Treatment: Acyclovir 400mg tds 7-10 days • Alternatives: Valacyclovir and Famciclovir • In setting of treatment failure, viral isolates tested for resistance against acyclovir • Alternative drugs: Foscarnet, Cidofovir • Chronic suppressive therapy ( >8 attacks per year) 2 2018/08/13 VARICELLA • Chickenpox • Presents with erythematous papules and umbilicated -

Experience with Molluscum Contagiosum and Associated Inflammatory Reactions in a Pediatric Dermatology Practice the Bump That Rashes
STUDY ONLINE FIRST Experience With Molluscum Contagiosum and Associated Inflammatory Reactions in a Pediatric Dermatology Practice The Bump That Rashes Emily M. Berger, MD; Seth J. Orlow, MD, PhD; Rishi R. Patel, MD; Julie V. Schaffer, MD Objective: To investigate the frequency, epidemiol- (50.6% vs 31.8%; PϽ.001). In patients with molluscum ogy, clinical features, and prognostic significance of in- dermatitis, numbers of MC lesions increased during the flamed molluscum contagiosum (MC) lesions, mollus- next 3 months in 23.4% of those treated with a topical cum dermatitis, reactive papular eruptions resembling corticosteroid and 33.3% of those not treated with a topi- Gianotti-Crosti syndrome, and atopic dermatitis in pa- cal corticosteroid, compared with 16.8% of patients with- tients with MC. out dermatitis. Patients with inflamed MC lesions were less likely to have an increased number of MC lesions Design: Retrospective medical chart review. over the next 3 months than patients without inflamed MC lesions or dermatitis (5.2% vs 18.4%; PϽ.03). The Setting: University-based pediatric dermatology practice. GCLRs were associated with inflamed MC lesion (PϽ.001), favored the elbows and knees, tended to be Patients: A total of 696 patients (mean age, 5.5 years) pruritic, and often heralded resolution of MC. Two pa- with molluscum. tients developed unilateral laterothoracic exanthem– like eruptions. Main Outcome Measures: Frequencies, characteris- tics, and associated features of inflammatory reactions Conclusions: Inflammatory reactions to MC, including to MC in patients with and without atopic dermatitis. the previously underrecognized GCLR, are common. Treat- ment of molluscum dermatitis can reduce spread of MC Results: Molluscum dermatitis, inflamed MC lesions, and via autoinoculation from scratching, whereas inflamed MC Gianotti-Crosti syndrome–like reactions (GCLRs) oc- lesions and GCLRs reflect cell-mediated immune re- curred in 270 (38.8%), 155 (22.3%), and 34 (4.9%) of sponses that may lead to viral clearance. -

Back to Basics: Understanding Hidradenitis Suppurativa
PRACTICE DEVELOPMENT Back to basics: understanding hidradenitis suppurativa KEY WORDS Hidradenitis Suppurativa (HS) is a chronic recurrent debilitating skin disease of the Dermatology hair follicle. It is a condition that has been overlooked in wound care publications, Fistulae with most articles found in dermatological journals. However, the condition affects Hidradenitis Suppurativa 1% of the population in Europe and produces painful nodules in one or more of Scarring Sinus tracts the apocrine-gland bearing aspects of the skin that can ulcerate and produce pain and a foul odour and can multiply and eventually develop sinus tracts and fistulae. HS is often misdiagnosed as alternative skin ulcerating conditions, leaving the individuals with many years of suffering from the physical symptoms and their psychological consequences. The disease often begins in puberty and burns out by middle age, leaving the individual with unsightly scarring. This article examines the pathophysiology, clinical presentations and comorbidities associated with the disease. The treatment options focus on controlling the comorbidities, moderating life-style behaviours and arresting the disease. The medical and surgical options are discussed along with their limitations. idrarenitis Suppurativa (HS) was first selection bias, however is thought to be 1% in described by the French surgeon Velpeau Europe (Gulliver et al, 2016; WUWHS, 2016). in 1839. The origin of the term HS comes Prevalence is rare in children and when HS does Hfrom the Greek hidros meaning sweat and aden occur in this population it is often associated with denoting glands (Ather et al, 2006). Initially it was hormonal disorders such as metabolic syndrome, thought to be due to infection of the sweat glands precocious puberty, adrenal hyperplasia and however it is now recognized as an acneform premature adrenarche (Vivar and Kruse, 2017). -

WO 2014/134709 Al 12 September 2014 (12.09.2014) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2014/134709 Al 12 September 2014 (12.09.2014) P O P C T (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every A61K 31/05 (2006.01) A61P 31/02 (2006.01) kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, (21) International Application Number: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, PCT/CA20 14/000 174 DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (22) International Filing Date: HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, 4 March 2014 (04.03.2014) KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, (25) Filing Language: English OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, (26) Publication Language: English SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, (30) Priority Data: ZW. 13/790,91 1 8 March 2013 (08.03.2013) US (84) Designated States (unless otherwise indicated, for every (71) Applicant: LABORATOIRE M2 [CA/CA]; 4005-A, rue kind of regional protection available): ARIPO (BW, GH, de la Garlock, Sherbrooke, Quebec J1L 1W9 (CA). GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, SZ, TZ, UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, (72) Inventors: LEMIRE, Gaetan; 6505, rue de la fougere, TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, DK, Sherbrooke, Quebec JIN 3W3 (CA).