Drugs, Sleep, and the Addicted Brain
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ventrolateral Preoptic Nucleus (VLPO) Role in Turning the Ascending Arousal System Off During Sleep
Progressing Aspects in Pediatrics and Neonatology DOI: 10.32474/PAPN.2020.02.000146 ISSN: 2637-4722 Mini Review Ventrolateral Preoptic Nucleus (VLPO) Role in Turning the Ascending Arousal System Off During Sleep Behzad Saberi* Medical Research, Esfahan, Iran *Corresponding author: Behzad Saberi, Medical Research, Esfahan, Iran Received: June 02, 2020 Published: July 24, 2020 Mini Review References Coordinated manner of action of the projections from monoaminergic cell groups, cholinergic and orexin neurons, 1. Saper, Clifford B, Scammell, Thomas E Lu (2005) Hypothalamic regulation of sleep and circadian rhythms. Nature 437 (7063): 1257- produces arousal. Turning this arousal system off would result in 1263. producing sleep. There is an important role for the Ventrolateral 2. Chou Thomas C, Scammell Thomas E, Gooley Joshua J, Gaus Stephanie, Preoptic Nucleus (VLPO) to inhibit the arousal circuits during sleep. Saper Clifford B Lu (2003) “Critical Role of Dorsomedial Hypothalamic VLPO neurons are sleep active neurons [1-3]. Also, these neurons Nucleus in a Wide Range of Behavioral Circadian Rhythms”. The Journal of Neuroscience 23 (33): 10691-10702. contain GABA and Galanin as inhibitory neurotransmitters. Such 3. Phillips AJK, Robinson PA (2007) A Quantitative Model of Sleep-Wake neurons receive afferents from monoaminergic systems. VLPO Dynamics Based on the Physiology of the Brainstem Ascending Arousal lesions would cause fragmented sleep and insomnia. System. Journal of Biological Rhythms 22(2): 167-179. VLPO has two groups of neurons: One group located in the 4. Brown RE, McKenna JT (2015) Turning a Negative into a Positive: Ascending GABAergic Control of Cortical Activation and Arousal. Front. core of the VLPO and its neurons project to the tuberomammillary Neurol 6: pp.135. -

Estradiol Action at the Median Preoptic Nucleus Is Necessary And
bioRxiv preprint doi: https://doi.org/10.1101/2020.07.29.223669; this version posted July 29, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Estradiol Action at the Median Preoptic Nucleus is Necessary and Sufficient for Sleep Suppression in Female rats Smith PC, Cusmano DM, Phillips DJ, Viechweg SS, Schwartz MD, Mong JA Support: This work was supported by Grant 1F30HL145901 (to P.C.S.), Grant F31AG043329 (to D.M.C.) and Grant R01HL85037 (to J.A.M.). The authors are responsible for this work; it does not necessarily represent the official views of the NIA, NHLBI, or NIH. Disclosure: The authors have nothing to disclose Conflicts of Interest: The authors have no conflicts of interest. Abstract To further our understanding of how gonadal steroids impact sleep biology, we sought to address the mechanism by which proestrus levels of cycling ovarian steroids, particularly estradiol (E2), suppress sleep in female rats. We showed that steroid replacement of proestrus levels of E2 to ovariectomized female rats, suppressed sleep to similar levels as those reported by endogenous ovarian hormones. We further showed that this suppression is due to the high levels of E2 alone, and that progesterone did not have a significant impact on sleep behavior. We found that E2 action within the Median Preoptic Nucleus (MnPN), which contains estrogen receptors (ERs), is necessary for this effect; antagonism of ERs in the MnPN attenuated the E2-mediated suppression of both non- Rapid Eye Movement (NREM) and Rapid Eye Movement (REM) sleep. -

The Substantia Nigra the Tuberomammillary Nucleus
Neurotransmitter Receptors in the Substantia Nigra & the Tuberomammillary Nucleus Coronal Section Coronal Section Coronal Section Substantia Nigra From Pedunculopontine Nucleus Pars Compacta From Dorsal Raphe From Striatum (Caudate/Putamen) Substantia Nigra Hypothalamus Hypothalamus Substantia Nigra From Striatum (Caudate/Putamen) 5-HT R The Substantia Nigra 1B M Muscarinic AChR The substantia nigra (SN) is an area of deeply pigmented cells in the 5 ACh+ midbrain that regulates movement and coordination. Neurons of the nAChR α4α5α6β2 SN are divided into the substantia nigra pars compacta (SNc) and the substantia nigra pars reticulata (SNr). Neurons of the SNc produce Dopamine, which stimulates movement. In contrast, GABAergic neurons of the SNr can stimulate or inhibit movement depending on GABA+ GABAergic Neuron the input signal. GluR6:KA2 D2R mGluR5 mGluR3 From Subthalamic Nucleus GABA-A-R The SN controls movement by functioning as part of the basal ganglia, α3γ2 5-HT1BR Adenosine A1R CB1R a network of neurons that is critical for motion and memory. Along with GABA-B-R1 α GABA+ 4 Astrocyte GABA-B-R2 the SN, the basal ganglia consists of the putamen, the subthalamic EAAT1/GLAST-1 D R + + nAChR α3γ2 1 Neurokinin A /GABA nucleus, the caudate, and the globus pallidus, which is further divided GABA-A-R mGluR7 NK3R NK3R GABA-B-R1 µ-Opioid receptor into the globus pallidus interna (GPi) and the globus pallidus externa EAAT3 GABA-A-R α3γ3/γ2 GABA-B-R2 (GPe). Excluding the caudate, which is thought to be involved in EAAT4 D R learning and memory, the nuclei of the basal ganglia receive signals 2 D R α α β from the cerebral cortex when there is intent to coordinate movement. -

Reidun Ursin Changing Concepts on the Role of Serotonin in the Regulation of Sleep and Waking
Reidun Ursin Changing concepts on the role of serotonin in the regulation of sleep and waking The story of serotonin and sleep has been developing for more than 50 years, from the discovery in the 1950s that it had a role in brain function and in EEG synchronization. In parallel, the areas of sleep research and neurochemistry have seen enormous developments. The concept of serotonin as a sleep neurotransmitter was based on the effects of lesions of the brainstem raphe nuclei and the effects of serotonin depleting drugs in cats. The description of the firing pattern of the dorsal raphe nuclei changed this concept, initially to the entirely opposite view of serotonin as a waking transmitter. More recently, there has emerged a more complex view on the role of serotonin as a modulator of both waking and sleep. The effects of serotonin on sleep and waking may depend on which neurons are firing, their projection site, which postsynaptic receptors are present at this site, and, not the least, on the functional state of the system and the organism at a particular moment. Christopher A. Lowry, Andrew K. Evans, Paul J. Gasser, Matthew W. Hale, Daniel R. Staub and Anantha Shekhar Topographic organization and chemoarchitecture of the dorsal raphe nucleus and the median raphe nucleus The role of serotonergic systems in regulation of behavioral arousal and sleep-wake cycles is complex and may depend on both the receptor subtype and brain region involved. Increasing evidence points toward the existence of multiple topographically organized subpopulations of serotonergic neurons that receive unique afferent connections, give rise to unique patterns of projections to forebrain systems, and have unique functional properties. -

The Paraventricular Nucleus of the Thalamus Is Recruited by Both
REVIEW ARTICLE published: 03 April 2014 BEHAVIORAL NEUROSCIENCE doi: 10.3389/fnbeh.2014.00117 The paraventricular nucleus of the thalamus is recruited by both natural rewards and drugs of abuse: recent evidence of a pivotal role for orexin/hypocretin signaling in this thalamic nucleus in drug-seeking behavior Alessandra Matzeu*, Eva R. Zamora-Martinez and Rémi Martin-Fardon Molecular and Cellular Neuroscience Department, The Scripps Research Institute, La Jolla, CA, USA Edited by: A major challenge for the successful treatment of drug addiction is the long-lasting Christopher V. Dayas, University of susceptibility to relapse and multiple processes that have been implicated in the Newcastle, Australia compulsion to resume drug intake during abstinence. Recently, the orexin/hypocretin Reviewed by: (Orx/Hcrt) system has been shown to play a role in drug-seeking behavior. The Orx/Hcrt Andrew Lawrence, Florey Neuroscience Institutes, Australia system regulates a wide range of physiological processes, including feeding, energy Robyn Mary Brown, Florey metabolism, and arousal. It has also been shown to be recruited by drugs of abuse. Neuroscience Institutes, Australia Orx/Hcrt neurons are predominantly located in the lateral hypothalamus that projects to *Correspondence: the paraventricular nucleus of the thalamus (PVT), a region that has been identified as a Alessandra Matzeu, Molecular and “way-station” that processes information and then modulates the mesolimbic reward and Cellular Neuroscience Department, The Scripps Research Institute, 10550 extrahypothalamic stress systems. Although not thought to be part of the “drug addiction North Torrey Pines Road, SP30-2120, circuitry”,recent evidence indicates that the PVT is involved in the modulation of reward La Jolla, CA 92037, USA function in general and drug-directed behavior in particular. -
Distribution of Dopamine D3 Receptor Expressing Neurons in the Human Forebrain: Comparison with D2 Receptor Expressing Neurons Eugenia V
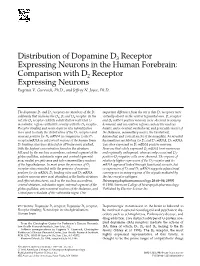
Distribution of Dopamine D3 Receptor Expressing Neurons in the Human Forebrain: Comparison with D2 Receptor Expressing Neurons Eugenia V. Gurevich, Ph.D., and Jeffrey N. Joyce, Ph.D. The dopamine D2 and D3 receptors are members of the D2 important difference from the rat is that D3 receptors were subfamily that includes the D2, D3 and D4 receptor. In the virtually absent in the ventral tegmental area. D3 receptor rat, the D3 receptor exhibits a distribution restricted to and D3 mRNA positive neurons were observed in sensory, mesolimbic regions with little overlap with the D2 receptor. hormonal, and association regions such as the nucleus Receptor binding and nonisotopic in situ hybridization basalis, anteroventral, mediodorsal, and geniculate nuclei of were used to study the distribution of the D3 receptors and the thalamus, mammillary nuclei, the basolateral, neurons positive for D3 mRNA in comparison to the D2 basomedial, and cortical nuclei of the amygdala. As revealed receptor/mRNA in subcortical regions of the human brain. by simultaneous labeling for D3 and D2 mRNA, D3 mRNA D2 binding sites were detected in all brain areas studied, was often expressed in D2 mRNA positive neurons. with the highest concentration found in the striatum Neurons that solely expressed D2 mRNA were numerous followed by the nucleus accumbens, external segment of the and regionally widespread, whereas only occasional D3- globus pallidus, substantia nigra and ventral tegmental positive-D2-negative cells were observed. The regions of area, medial preoptic area and tuberomammillary nucleus relatively higher expression of the D3 receptor and its of the hypothalamus. In most areas the presence of D2 mRNA appeared linked through functional circuits, but receptor sites coincided with the presence of neurons co-expression of D2 and D3 mRNA suggests a functional positive for its mRNA. -

General Anesthesia and Ascending Arousal Pathways
Anesthesiology 2009; 111:695–6 Copyright © 2009, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. General Anesthesia and Ascending Arousal Pathways THE ability to produce a reversible loss of consciousness on cortical (and hippocampal) recordings from anesthe- is the defining characteristic of general anesthetics. It is tized rats, using power spectral analysis and the burst also the most fascinating and elusive. Although the mo- suppression ratio to quantify the electroencephalogra- lecular targets of many anesthetics have been identified, phy under isoflurane anesthesia. they are widely distributed in the central nervous sys- In the first part of the study, histamine was locally tem. Therefore, identifying the locus of action of these infused into the nucleus basalis magnocellularis (NBM) drugs in the brain represents a major challenge. The of the basal forebrain during burst suppression caused neuronal mechanisms of sleep, a physiologic state that by isoflurane (at 1.4%). The electroencephalography involves a loss of consciousness, provide one obvious shows a pronounced shift to increased delta and theta Downloaded from http://pubs.asahq.org/anesthesiology/article-pdf/111/4/695/248373/0000542-200910000-00005.pdf by guest on 02 October 2021 avenue of enquiry.1 Brain imaging and electroencepha- power, equivalent to the pattern recorded at lower con- lographic studies give a broad characterization of the centrations of isoflurane. The respiratory rate was also anesthetic state and show clear similarities with the increased, which the authors cite as a measure of behav- sleeping brain. However, natural sleep and wakefulness ioral arousal. Behavioral arousal itself was not observed, are controlled by multiple arousal pathways, as well as but this was presumably because of the high concentra- by the intimate connectivity between the thalamus and tions of isoflurane used. -

Histamine Modulation of the Basal Ganglia Circuitry in the Development of Pathological Grooming
Histamine modulation of the basal ganglia circuitry in the development of pathological grooming Maximiliano Rapanellia,1,2, Luciana Fricka,1,3, Haruhiko Bitob, and Christopher Pittengera,c,4 aDepartment of Psychiatry, Yale University hool of Medicine, New Haven, CT 06510; bDepartment of Neurochemistry, Graduate School of Medicine, University of Tokyo, Tokyo 113-0033, Japan; and cDepartment of Psychology, Child Study Center, and Interdepartmental Neuroscience Program, Yale University, New Haven, CT 06519 Edited by Solomon H. Snyder, The Johns Hopkins University School of Medicine, Baltimore, MD, and approved May 11, 2017 (received for review March 19, 2017) Aberrant histaminergic function has been proposed as a cause of Elevated grooming has garnered increasing interest in recent years tic disorders. A rare mutation in the enzyme that produces as a potential behavioral model for compulsive behavior (21). It is histamine (HA), histidine decarboxylase (HDC), has been identified seen in proposed mouse models of OCD (22–24), autism (25, 26), in patients with Tourette syndrome (TS). Hdc knockout mice ex- Rett syndrome (27), and trichotillomania (28). Repetitive stimu- hibit repetitive behavioral pathology and neurochemical charac- lation of projections from the orbitofrontal cortex to the striatum, teristics of TS, establishing them as a plausible model of tic thought to be hyperactive in OCD, can produce elevated groom- pathophysiology. Where, when, and how HA deficiency produces ing (29). these effects has remained unclear: whether the contribution of TS and OCD are associated with abnormalities in the basal HA deficiency to pathogenesis is acute or developmental, and ganglia circuitry (30–32). HA receptors are particularly dense in where in the brain the relevant consequences of HA deficiency the basal ganglia (1), and HDC protein is present at exception- occur. -

Regulate Serotonin Neurons in the Dorsal Raphe Nucleus by Excitatory Direct and Inhibitory Indirect Actions
The Journal of Neuroscience, November 1, 2002, 22(21):9453–9464 Hypocretins (Orexins) Regulate Serotonin Neurons in the Dorsal Raphe Nucleus by Excitatory Direct and Inhibitory Indirect Actions Rong-Jian Liu,1 Anthony N. van den Pol,3 and George K. Aghajanian1,2 Departments of 1Psychiatry, 2Pharmacology, and 3Neurosurgery, Yale School of Medicine, New Haven, Connecticut 06508 ϳ The hypocretins (hcrt1 and hcrt2) are expressed by a discrete taneous postsynaptic currents in 5-HT neurons (EC50 , 450– population of hypothalamic neurons projecting to many regions 600 nM), which were TTX-sensitive and mostly blocked by the of the CNS, including the dorsal raphe nucleus (DRN), where GABAA antagonist bicuculline, indicating increased impulse serotonin (5-HT) neurons are concentrated. In this study, we flow in local GABA interneurons. Accordingly, hcrts were found investigated responses to hcrts in 216 physiologically identified to increase the basal firing of presumptive GABA interneurons. 5-HT and non-5-HT neurons of the DRN using intracellular and Immunolabeling showed that hcrt fibers projected to both 5-HT whole-cell recording in rat brain slices. Hcrt1 and hcrt2 induced and GABA neurons in the DRN. We conclude that hcrts act similar amplitude and dose-dependent inward currents in most directly to excite 5-HT neurons primarily via a TTX-insensitive, ϳ ϩ ϩ 5-HT neurons tested (EC50 , 250 nM). This inward current was Na /K nonselective cation current, and indirectly to activate not blocked by the fast Na ϩ channel blocker TTX or in a local inhibitory GABA inputs to 5-HT cells. The greater potency Ca 2ϩ-free solution, indicating a direct postsynaptic action. -
Physiology of Consciousness Consciousness
Physiology of Consciousness consciousness • Is the brain state in which a person is being aware of the self and surroundings • It is a product of electrical activity of the brain • (flat EEG = unconscious) 4 levels of consciousness 1- Normal consciousness 2- Clouded consciousness 3- Sleep 4- Coma Level of consciousness • (1) Normal Consciousness • (state of normal arousal , being fully awake and aware of the self and surroundings ) • (2) Clouded consciousness : • person conscious but mentally confused • e.g., in cases of drug or alcohol intoxication , High fever associated (malaria or septicemia , dementia , etc ) . • (3) Sleep : • person unconscious ( in relation to the external world & surroundings) • but is arousable ( can be aroused ) . • (4) Coma : person unconscious and not arousable Brain Structures involved in the conscious state: • Brain stem Reticular formation • Thalamus • Hypothalamus • Ascending projection pathways • Wide spread area in the cerebral cortex Reticular formation Set of interconnected nuclei that are located throughout the brainstem (Pons, Midbrain, Upper medulla), and the thalamus Role in behavioral arousal Role in consciousness (sleep/awake cycle) Connect the brain stem to the CC consists of 3 parts: Lateral Reticular Formation Para median Reticular Formation Raphe nuclei (Median RF) Lateral Reticular Formation Has small neurones Receives information from ascending tracts for touch and pain. Receives vestibular information from median vestibular nerve. Receives auditory information from superior olivary nucleus. Visual information from superior colliculus. Olfactory information via medial forebrain bundle Paramedian Reticular Formation Has large cells. -Receives signals from lateral reticular formation -Nucleus ceruleus contains noradrenergic neurones and projects onto the cerebral cortex. -Ventral tegmental nucleus contains dopaminergic neurones that project directly onto the cortex. -

Thalamic Neuromodulation and Its Implications for Executive Networks
Thalamic neuromodulation and its implications for executive networks The MIT Faculty has made this article openly available. Please share how this access benefits you. Your story matters. Citation Varela, Carmen. “Thalamic Neuromodulation and Its Implications for Executive Networks.” Front. Neural Circuits 8 (June 24, 2014). As Published http://dx.doi.org/10.3389/fncir.2014.00069 Publisher Frontiers Research Foundation Version Final published version Citable link http://hdl.handle.net/1721.1/89204 Terms of Use Creative Commons Attribution Detailed Terms http://creativecommons.org/licenses/by/4.0/ REVIEW ARTICLE published: 24 June 2014 doi: 10.3389/fncir.2014.00069 Thalamic neuromodulation and its implications for executive networks Carmen Varela* Picower Institute for Learning and Memory, Massachusetts Institute of Technology, Cambridge, MA, USA Edited by: The thalamus is a key structure that controls the routing of information in the brain. Guillermo Gonzalez-Burgos, Understanding modulation at the thalamic level is critical to understanding the flow of University of Pittsburgh, USA information to brain regions involved in cognitive functions, such as the neocortex, the Reviewed by: hippocampus, and the basal ganglia. Modulators contribute the majority of synapses Robert P.Vertes, Florida Atlantic University, USA that thalamic cells receive, and the highest fraction of modulator synapses is found in Randy M. Bruno, Columbia University, thalamic nuclei interconnected with higher order cortical regions. In addition, disruption USA of modulators often translates into disabling disorders of executive behavior. However, *Correspondence: modulation in thalamic nuclei such as the midline and intralaminar groups, which are Carmen Varela, Picower Institute for interconnected with forebrain executive regions, has received little attention compared Learning and Memory, Massachusetts Institute of Technology, Building 46, to sensory nuclei. -

Arousal and Sleep Circuits
www.nature.com/npp NEUROPSYCHOPHARMACOLOGY REVIEWS Arousal and sleep circuits Barbara E. Jones1 The principal neurons of the arousal and sleep circuits are comprised by glutamate and GABA neurons, which are distributed within the reticular core of the brain and, through local and distant projections and interactions, regulate cortical activity and behavior across wake-sleep states. These are in turn modulated by the neuromodulatory systems that are comprised by acetylcholine, noradrenaline, dopamine, serotonin, histamine, orexin (hypocretin), and melanin-concentrating hormone (MCH) neurons. Glutamate and GABA neurons are heterogeneous in their profiles of discharge, forming distinct functional cell types by selective or maximal discharge during (1) waking and paradoxical (REM) sleep, (2) during slow wave sleep, (3) during waking, or (4) during paradoxical (REM) sleep. The neuromodulatory systems are each homogeneous in their profile of discharge, the majority discharging maximally during waking and paradoxical sleep or during waking. Only MCH neurons discharge maximally during sleep. They each exert their modulatory influence upon other neurons through excitatory and inhibitory receptors thus effecting a concerted differential change in the functionally different cell groups. Both arousal and sleep circuit neurons are homeostatically regulated as a function of their activity in part through changes in receptors. The major pharmacological agents used for the treatment of wake and sleep disorders act upon GABA and neuromodulatory transmission. Neuropsychopharmacology (2020) 45:6–20; https://doi.org/10.1038/s41386-019-0444-2 INTRODUCTION NEURONS IN THE RETICULAR CORE UTILIZING AMINO ACID Arousal circuits comprise multiple diverse, partially redundant NEUROTRANSMITTERS CONSTITUTE AROUSAL AND SLEEP systems which promote behavioral arousal that is accompanied CIRCUITS by cortical activation.