Epidemiology of Japanese Encephalitis Cases in Dhemaji District of Assam, India
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

LIST of ACCEPTED CANDIDATES APPLIED for the POST of GD. IV of AMALGAMATED ESTABLISHMENT of DEPUTY COMMISSIONER's, LAKHIMPUR
LIST OF ACCEPTED CANDIDATES APPLIED FOR THE POST OF GD. IV OF AMALGAMATED ESTABLISHMENT OF DEPUTY COMMISSIONER's, LAKHIMPUR Date of form Sl Post Registration No Candidate Name Father's Name Present Address Mobile No Date of Birth Submission 1 Grade IV 101321 RATUL BORAH NAREN BORAH VILL:-BORPATHAR NO-1,NARAYANPUR,GOSAIBARI,LAKHIMPUR,Assam,787033 6000682491 30-09-1978 18-11-2020 2 Grade IV 101739 YASHMINA HUSSAIN MUZIBUL HUSSAIN WARD NO-14, TOWN BANTOW,NORTH LAKHIMPUR,KHELMATI,LAKHIMPUR,ASSAM,787031 6002014868 08-07-1997 01-12-2020 3 Grade IV 102050 RAHUL LAMA BIKASH LAMA 191,VILL NO 2 DOLABARI,KALIABHOMORA,SONITPUR,ASSAM,784001 9678122171 01-10-1999 26-11-2020 4 Grade IV 102187 NIRUPAM NATH NIDHU BHUSAN NATH 98,MONTALI,MAHISHASAN,KARIMGANJ,ASSAM,788781 9854532604 03-01-2000 29-11-2020 5 Grade IV 102253 LAKHYA JYOTI HAZARIKA JATIN HAZARIKA NH-15,BRAHMAJAN,BRAHMAJAN,BISWANATH,ASSAM,784172 8638045134 26-10-1991 06-12-2020 6 Grade IV 102458 NABAJIT SAIKIA LATE CENIRAM SAIKIA PANIGAON,PANIGAON,PANIGAON,LAKHIMPUR,ASSAM,787052 9127451770 31-12-1994 07-12-2020 7 Grade IV 102516 BABY MISSONG TANKESWAR MISSONG KAITONG,KAITONG ,KAITONG,DHEMAJI,ASSAM,787058 6001247428 04-10-2001 05-12-2020 8 Grade IV 103091 MADHYA MONI SAIKIA BOLURAM SAIKIA Near Gosaipukhuri Namghor,Gosaipukhuri,Adi alengi,Lakhimpur,Assam,787054 8011440485 01-01-1987 07-12-2020 9 Grade IV 103220 JAHAN IDRISH AHMED MUKSHED ALI HAZARIKA K B ROAD,KHUTAKATIA,JAPISAJIA,LAKHIMPUR,ASSAM,787031 7002409259 01-01-1988 01-12-2020 10 Grade IV 103270 NIHARIKA KALITA ARABINDA KALITA 006,GUWAHATI,KAHILIPARA,KAMRUP -

Basic Information on the Status of Ado & Vlew
BASIC INFORMATION ON THE STATUS OF ADO & VLEW 1. N A M E O F D I S T R I C T : N A L B A R I Sl. Name of Agri Sub- Name of SDAO Name of ADO Name of the ADO Name of VLEW Name of the VLEW with contact Name of G.P No Development Division with contact no. circle with contact no. Eleka no. Block 1 2 3 4 5 6 7 8 9 1. Barbhag Nalbari Jogeswar Kamarkuchi Ghanashyam Das – Ranakuchi Kandarpa Kalita – 9864167392 47(1) Barbhag- Ranakuchi Rajmedhi – 9859926507 Sonkani (Vacant) i/c Kandarpa Kalita 47(1) Barbhag 9435323218 Kalag Vacant) i/c Kandarpa Kalita 48 (2) Pandula Barbhag, 52 (6) Barkuriha Porakuchi Hemanta Bezbarua-9957691157 51(5) Barbhag, 52(6) Barkuriha Arangmou (Vacant) i/c Hemanta Bezbarua 49(3) Kamarkuchi Pandula (Vacant) i/c Hemanta Bezbarua 48(2) Pandula, 53(7) Senekuchi Kamarkuchi (vancant)i/c Fazlur Rahman - 49(3) Kamarkuchi ph.- 9706018390 Arikuchi Fazlur Rahman - 9706018390 50(4) Karia, 51(5) Marowa Karia Krishna Bezbarua-9859291164 50(4) Karia Bezkuchi (vacant) i/c Krishna Bezbarua- 50(4) Karia, 51(5) Marowa Marowa Dharani Talukdar-9859476756 51(5) Marowa, 52(6)Barkuriha 2. Pachim Nalbari Nalbari Jogeswar Chamata Nilamani Medhi Bihampur Vacant ,i/c Bhabesh Bhatta- 26no. Bangaon (Part) Rajmedhi – Ph. 9435513843 Barnarddi Bhabesh Bhatta- 9577044463 28 no. Barnarddi 9435323218 Simaliya Mahammad Ali-9435646568 25 no.Rupiabathan & 26 no Bangaon Niz Pakowa Vacant- Pramod Sarma- 27 no. Panigaon 9707424580 Madhupur Nalbari Jogeswar Chamata Nilamani Medhi Gamarimuri Vacant i/c Mukul Sarma 35 no. -
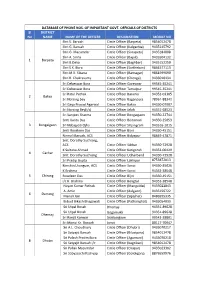
DATABASE of PHONE NOS. of IMPORTANT GOVT. OFFICIALS of DISTRICTS Sl DISTRICT No NAME NAME of the OFFICER DESIGNATION MOBILE NO Shri S
DATABASE OF PHONE NOS. OF IMPORTANT GOVT. OFFICIALS OF DISTRICTS Sl DISTRICT No NAME NAME OF THE OFFICER DESIGNATION MOBILE NO Shri S. Baruah Circle Officer (Barpeta) 9854012478 Shri G. Baruah Circle Officer (Kalgachia) 9435145792 Shri G. Mazumdar Circle Officer (Sarupeta) 9435184008 Shri A. Sinha Circle Officer (Bajali) 9435504132 1 Barpeta Shri B.Deka Circle Officer (Baghbar) 9435152250 Shri S.K. Bora Circle Officer (Sarthebari) 9864577113 Shri M.K. Sikaria Circle Officer (Barnagar) 9864599690 Shri R. Chakravarty Circle Officer (Chenga) 9435010434 Sri Debeswar Bora Circle Officer Goreswar 99545‐35241 Sri Debeswar Bora Circle Officer Tamulpur 99545‐35241 Sri Ratul Pathak Circle Officer Barama 94352‐03305 2 Baksa Sri Norsing bey Circle Officer Baganpara 78961‐88342 Sri Gaya Prasad Agarwal Circle Officer Baksa 94350‐07907 Sri Norsing Bey(i/c) Circle Officer Jalah 94351‐68523 Sri Sanjeev Sharma Circle Officer Bongaigaon 94350‐22744 Smti Kanta Das Circle Officer Boitamari 94350‐25053 3 Bongaigaon Sri Nabajyoti Ojha Circle Officer Srijangram 943516‐1015 Smti Roseleen Das Circle Officer Bijni 94350‐45151 Nirmali Baruah, ACS Circle Officer Bidyapur 98649‐47871 Smt. Dorothy Suchiang, ACS Circle Officer Silchar 94350‐72928 K.Sultana Ahmed Circle Officer Katigorah 94352‐00429 4 Cachar Smt. Dorothy Suchiang Circle Officer Udharband 94350‐72928 Sri Pradip Gupta Circle Officer Lakhipur 8753872013 Kimchin Lhangum, ACS Circle Officer Sonai 94350‐35026 K.Brahma Circle Officer Sonai 94353‐38548 5 Chirang Roseleen Das Circle Officer Bijni 94350‐45151 i/c K. Brahma Circle Officer Bengtal 94353‐38548 Nayan Kumar Pathak Circle Officer (Mangaldai) 9435022843 A. Amin Circle Officer (dalgaon) 9435156722 6 Darrang Manali Jain Circle Officer (Sipajhar) 8486595335 Bidyut Bikash Bhagawati Circle Officer (Patharighat) 9435054033 Sri Utpal Borah Dhemaji 94351‐89628 Sri Utpal Borah Gogamukh 94351‐89628 Dhemaji Sri Ranjit Konwar Sissiborgaon 99542‐28801 Sri Monui Kr. -

List of Candidates Called for Preliminary Examination for Direct Recruitment of Grade-Iii Officers in Assam Judicial Service
LIST OF CANDIDATES CALLED FOR PRELIMINARY EXAMINATION FOR DIRECT RECRUITMENT OF GRADE-III OFFICERS IN ASSAM JUDICIAL SERVICE. Sl No Name of the Category Roll No Present Address Candidate 1 2 3 4 5 1 A.M. MUKHTAR AHMED General 0001 C/O Imran Hussain (S.I. of Ploice), Convoy Road, Near Radio Station, P.O.- CHOUDHURY Boiragimath, Dist.- Dibrugarh, Pin-786003, Assam 2 AAM MOK KHENLOUNG ST 0002 Tipam Phakey Village, P.O.- Tipam(Joypur), Dist.- Dibrugarh(Assam), Pin- 786614 3 ABBAS ALI DEWAN General 0003 Vill: Dewrikuchi, P.O.:-Sonkuchi, P.S.& Dist.:- Barpeta, Assam, Pin-781314 4 ABDIDAR HUSSAIN OBC 0004 C/O Abdul Motin, Moirabari Sr. Madrassa, Vill, PO & PS-Moirabari, Dist-Morigaon SIDDIQUEE (Assam), Pin-782126 5 ABDUL ASAD REZAUL General 0005 C/O Pradip Sarkar, Debdaru Path, H/No.19, Dispur, Ghy-6. KARIM 6 ABDUL AZIM BARBHUIYA General 0006 Vill-Borbond Part-III, PO-Baliura, PS & Dist-Hailakandi (Assam) 7 ABDUL AZIZ General 0007 Vill. Piradhara Part - I, P.O. Piradhara, Dist. Bongaigaon, Assam, Pin - 783384. 8 ABDUL AZIZ General 0008 ISLAMPUR, RANGIA,WARD NO2, P.O.-RANGIA, DIST.- KAMRUP, PIN-781365 9 ABDUL BARIK General 0009 F. Ali Ahmed Nagar, Panjabari, Road, Sewali Path, Bye Lane - 5, House No.10, Guwahati - 781037. 10 ABDUL BATEN ACONDA General 0010 Vill: Chamaria Pam, P.O. Mahtoli, P.S. Boko, Dist. Kamrup(R), Assam, Pin:-781136 11 ABDUL BATEN ACONDA General 0011 Vill: Pub- Mahachara, P.O. & P.S. -Kachumara, Dist. Barpeta, Assam, Pin. 781127 12 ABDUL BATEN SK. General 0012 Vill-Char-Katdanga Pt-I, PO-Mohurirchar, PS-South Salmara, Dist-Dhubri (Assam) 13 ABDUL GAFFAR General 0013 C/O AKHTAR PARVEZ, ADVOCATE, HOUSE NO. -

Dhemaji State: Assam Annexure:A
DISTRICT DHEMAJI STATE: ASSAM ANNEXURE:A STATEMENT INDICATING THE SCHEMES FOR GENREAL AREAS OF FIRST (1st) INSTALMENTS OF THIRTEENTH FINANCE COMMISSION GRANTS FOR RURAL LOCAL BODIES FOR YEAR 2012-13 (In Rupees) Amount required in ZPs/Aps/GPs Level For For Water Sanitation For Operation Roads & Parks /Play others Others Nos of Population of Maintenanc Creation of Supply each family & Drains grounds/ income Name of Total amount Sl.N AP and the each AP Rural Areas e of Data Base below Maintenance waiting shed generating District and required Remarks o. GPs(LSG as per census, ( In Sq. Km) Accounts poverty Cost etc sources types of PRIs under 13th I) [2001] lines FC [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15] [16] DHEMAJI 1 ZP 1 537565 2585.52 200000.00 200000.00 0.00 0.00 0.00 2781100.07 0.00 0.00 2000000.00 5181100 2 AP 5 75000.00 0.00 0.00 0.00 0.00 4496650.11 0.00 0.00 3200000.00 7771650 3 GP 65 325000.00 0.00 0.00 0.00 0.00 11002750.18 0.00 1625000.00 0.00 12952750 537565 2585.52 600000 200000 0 0 0 18280500.36 0 1625000 5200000 25905500 NB: Schemes may implement as per government procedure. Standing committee must select one income generation schemes for resoruces mobilisation in ZP and AP level as per allocation of fund for income generating resource. Create profile for data base by private agency Schemes may implement through tender procedure. Prepare Plan & Estimate each schemess as per allocation Chief Executive Officer, Dhemaji Zilla Parishad 1 DISTRICT DHEMAJI STATE: ASSAM ANNEXURE:B STATEMENT INDICATING THE SCHEMES FOR GENREAL AREAS OF FIRST (1sT) INSTALMENTS OF THIRTEENTH FINANCE COMMISSION GRANTS FOR RURAL LOCAL BODIES FOR YEAR 2012-13 (In Rupees) Amount required in ZP Level Population of For For Creation Water Sanitation For Roads & Parks others Others Nos of the each AP Rural Areas Total amount Bank Sl.N Name of Nos of AP Maintenance of Data Base Supply each family Operation Drains /Play income Schemes Bank Account GP as per in ZP( In required Bank Type Branch Name of Bank & Addreess o. -

Stratified Random Sampling - Assam (Code -4)
Download The Result Stratified Random Sampling - Assam (Code -4) Species Selected for Stratification = Cattle + Buffalo Number of Villages Having 100 + (Cattle + Buffalo) = 19446 Design Level Prevalence = 0.2041 Cluster Level Prevalence = 0.02 Sensitivity of the test used = 0.9 Total No of Villages (Clusters) Selected = 165 Total No of Animals to be Sampled = 2145 Back to Calculation Number Cattle of units Buffalo Cattle DISTRICT_NAME BLOCK_CODE BLOCK_NAME VILLAGE_NAME Buffaloes Cattle + all to Proportion Proportion Buffalo sample BAKSA 12 Baksa Saruchakadol 0 508 508 740 13 0 13 BAKSA 12 Baksa Banbari 0 525 525 719 13 0 13 BAKSA 197 Tamulpur No 1 Paharpur 0 715 715 1113 13 0 13 BAKSA 12 Baksa Kharuajan 0 789 789 1395 13 0 13 Barpeta 21 Barpeta Kamalpur Pam 0 444 444 780 13 0 13 Barpeta 179 Sarthebari Kathalbhuri 0 624 624 728 13 0 13 Barpeta 19 Barnagar (Pt ) Shahpur 11 622 633 958 13 0 13 Barpeta 8 Baghbor Salekura 52 774 826 1230 13 1 12 Barpeta 8 Baghbor Rubi 6 1402 1408 1993 13 0 13 Biswanath 93 Helem BEKIJAN 0 272 272 463 13 0 13 Biswanath 79 Gohpur SONAPUR 0 474 474 548 13 0 13 Biswanath 93 Helem HOKAJAN 0 488 488 926 13 0 13 Biswanath 33 Biswanath JARA BARI 0 733 733 1021 13 0 13 Biswanath 33 Biswanath KAMARGAON 4 938 942 1376 13 0 13 BONGAIGAON 35 Boitamari Karchimari Pt III NC 5 345 350 577 13 0 13 BONGAIGAON 99 jangram Tulungia pt I 0 463 463 686 13 0 13 BONGAIGAON 99 jangram Tinkonia pt III 4 703 707 868 13 0 13 BONGAIGAON 29 Bijni (Pt ) Kushlaibari 0 1154 1154 1528 13 0 13 Cachar 191 Sonai Sundari Pt-IV 51 211 262 332 13 -

Review of Research Issn: 2249-894X Impact Factor : 5.7631(Uif) Ugc Approved Journal No
Review of ReseaRch issN: 2249-894X impact factoR : 5.7631(Uif) UGc appRoved JoURNal No. 48514 volUme - 8 | issUe - 9 | JUNe - 2019 HEALTH SEEKING BEHAVIOUR OF MISHING TRIBE IN A KULAJAN VILLAGE OF DHEMAJI DISTRICT IN ASSAM Probin Das Research Scholar of Dibrugarh University, Depart of Sociology. ABSTRACT: Health is man's natural condition. It is a prerequisite for human development and is an essential component for the well being of the mankind. It is the result of living in accordance with natural laws pertaining the body, mind and environment. The health status of an individual or group of people is often determined as much by socially and culturally constructed human practices as that by biological and environment factors. It is fact that healthy lifestyle is as much a product of health consciousness as the attitude toward life. According to the World Health Organization, the main determinant of health includes the social and economic environment, the physical environment and the person's life individual characteristic and behaviour. Therefore, for understanding health condition of Mishing in Kulajan, there is a need to examine their health seeking behavior, diseases, pattern of treatment, for medical facility etc. KEYWORDS: Health , World Health Organization , socially and culturally constructed. INTRODUCTION a community engaged with the • Seeking Behaviour of Mishing Health seeking behaviour is health care system in their social, tribe in Kulajan village. those remedial actions or economic, cultural and • To understand the Household activities that individual environmental condition. The Health Seeking Behaviour of undertaken to rectify health seeking behavior of the Mishing tribe. perceived ill health. -

School Wise List of External Evaluator, Gunotsav, 2018 (Round II), Dhemaji
School wise list of External Evaluator, Gunotsav, 2018 (Round II), Dhemaji Day of Sl District Block Cluster Village schcd School Group No Liasion Official Nodal Teacher Evaluator EEAddress EEContact Evaluation JUNTI BHUYAN SONOWAL, Executive Engineer,Executive Engineer, PWD, Lakhimpur 1 DHEMAJI BORDOLONI BHEBELI BHEBELI KOIBATTA 18130100301 881-NO BHEBELI KAIBORTA LPS 1 Day-1 Mridul Saikia , IE/RP, 9854397729 SRI PABAN KR. DAS 9435094300 9678259283 State Road Division, Ghilamara Executive Engineer,Executive Engineer, PWD, Lakhimpur 2 DHEMAJI BORDOLONI BHEBELI GAZING MAZ GAON 18130100404 MADHYA. BORDOLANI BHEBELI HS 1 Day-2 Mridul Bhuyan , CRCC, 9706058478 JAYANTA BORUAH, 8822213315 SRI PABAN KR. DAS 9435094300 State Road Division, Ghilamara Executive Engineer,Executive Engineer, PWD, Lakhimpur 3 DHEMAJI BORDOLONI BHEBELI BHEBELI 18130101702 NA-NADI KAIBATTA LPS 1 Day-3 Mridul Saikia , IE/RP, 9854397729 GAMDHAR DAS, 7399178266 SRI PABAN KR. DAS 9435094300 State Road Division, Ghilamara Associate Professor, Dhemaji Commerce College, 4 DHEMAJI BORDOLONI BHEBELI DEWDUBI 18130100501 DEWDUBI KAIBATRA LPS 2 Day-1 Mridul Bhuyan , CRCC, 9706058478 LABANYA CHUTIA, 9854755610 Rajib Kr. Dutta 9435187317 Dhemaji TULSIBARI Associate Professor, Dhemaji Commerce College, 5 DHEMAJI BORDOLONI BHEBELI 18130119601 TULSHIBARI BERBANGA LPS 2 Day-2 Mridul Saikia , IE/RP, 9854397729 JITU KUMAR CHUTIA, 9859645027 Rajib Kr. Dutta 9435187317 BERBHANGA Dhemaji KATORIPATHAR BALI KUMAR GOURAB PHUKAN, Associate Professor, Dhemaji Commerce College, 6 DHEMAJI BORDOLONI -

A Demographic Study 0N Deori Population in the Village Kapahtali Deori Gaon, District Dhemaji, Assam, India
International Journal of Interdisciplinary Research in Science Society and Culture(IJIRSSC) Vol: 2, Issue:1, (June Issue), 2016 ISSN: (P) 2395-4345, (O) 2455-2909 © IJIRSSC A Demographic Study 0n Deori Population in the Village Kapahtali Deori Gaon, District Dhemaji, Assam, India Milonjyoti Borgohain Assistant professor, Department of Anthropology Moridhal College, Dhemaji,Assam,India ABSTRACT : This study deals with the demography of Deori community inhabiting in the Kapahtali Deori Gaon of Dhemaji District, Assam and discusses the socio-cultural aspects of the community through the demographic parameters. There are a total of 78 Deori households in the village. There are total 428 Deori populations in the village out of which 233 are male and 195 are females. The primary data for demographic parameters regarding household census, population characteristics, educational status, occupational status etc were collected. Demographic indicators like sex ratio, literacy rate etc were also collected. Keywords: Demography, Deori, Dhemaji District, Households, Kapahtali, sex ratio. ____________________________________________________________________________ I. Introduction: The word demography has been deriving from Latin ‘demos’ means people and ‘graphy ‘means measurement. Demography is the statistical study of human population. It is like a mirror to a population. Demography is the backbone of planning and development for the people. Anthropological demography is a speciality within demography which uses anthropological theory and methods to provide a better understanding of demographic phenomena in the current and past populations. II. Objectives of the Study: The main objectives of the present research under the broad objectives of ‘Demography of Deori Community’ were as follows: 1) To conduct a household census; 2) To record and analyses the population characteristics; 3) To know the educational status; 4) To record and analyses the occupational status; III. -

Assam State Disaster Management Authority FLOOD REPORT Flood Situation As on Today I.E
Government of Assam Assam State Disaster Management Authority FLOOD REPORT Flood Situation as on Today i.e. 2nd July, 2017 at 7:00 PM PARTICULARS Situation as on 2nd July, 2017 Brahmaputra at Neamatighat (Jorhat), Dhansiri (S) at Numaligarh (Golaghat); Rivers flowing above Danger Level Jia Bharali at N.T.Rd. Xing (Sonitpur); Barak at Badarpurghat (Karimganj) Kushiyara at Karimganj (Karimganj). No. of Districts Affected 07 Name of Districts Affected Lakhimpur, Jorhat, Golaghat, Cachar, Dhemjai, Biswanath, Karimganj No. of Revenue Circles affected 24 Names of Revenue Circles affected Lakhimpur 06 Nowboicha, Narayanpur, Subansiri, Bihpuria, North Lakhimpur, Kadam Jorhat 02 Teok, Titabar Golaghat 02 Golaghat, Dergaon Cachar 02 Katigorah, Sadar Dhemaji 04 Dhemaji, Sissiborgaon, Jonai, Gogamukh Biswanath 03 Halem, Gohpur, Naduar Karimganj 05 Sadar, Nilambazar, R.K. Nagar, Patharkandi, Badarpur Total 24 No. of Villages/ Localities affected Lakhimpur 150 52 (Nowboicha), 05 (Narayanpur), 10 (Subansiri), 25 (Bihpuria), 57 (North Lakhimpur), 01 (Kadam) Jorhat 03 01 (Teok), 02 (Titabar) Golaghat 11 10 (Golaghat), 01(Dergaon) Cachar 35 33 (Katigorah), 02 (Sadar) Dhemaji 92 05 (Dhemaji), 06 (Sissiborgaon), 34 (Jonai), 47 (Gogamukh) Biswanath 09 07 (Halem), 01 (Gohpur), 01 (Naduar) Karimganj 198 40 (Sadar), 30 (Nilambazar), 43 (R.K. Nagar), 42 (Patharkandi), 43(Badarpur) Total 498 Total Crop area affected (in Hect) Lakhimpur 3,700.15 826.77 (Nowboicha), 160 (Narayanpur), 860 (Subansiri), 500 (Bihpuria), 1,338.38 (North Lakhimpur), 15 (Kadam) Jorhat -

Sarva Siksha Abhiyan
SARVA SIKSHA ABHIYAN DISTRICT : DHEMAJI DISTRICT ELEMENTARY EDUCATION PLAN (DEEP) (2002-2003 to 2009-2010) AXOM SARBA SIKSHA ABHIJAN MISSION GOVERNMENT OF ASSAM MAP OF DHEMAJI DISTRICT CONTENTS MAP OF DHEMAJI DISTRICT............................................................... .................................2 CONTENTS.............................................................................................................................3 DISTRICT AT A GLANCE....................................................................................................... 6 CHAPTER-1: DISTRICT PROFILE........................................................................................ 8 Location............................................................................................................................... 8 Boundaries...........................................................................................................................8 Historical Background..........................................................................................................8 Topography..........................................................................................................................8 Climate:............................................................................................................................... 9 Agriculture:...........................................................................................................................9 Drainage:............................................................................................................................ -

Citizen Centric Service Delivery Project Tribal
SFG1771 Public Disclosure Authorized THE WORLD BANK ASSISTED CITIZEN CENTRIC SERVICE DELIVERY PROJECT Public Disclosure Authorized TRIBAL DEVELOPMENT PLAN January 2016 Public Disclosure Authorized Draft Report Public Disclosure Authorized ARIAS Society Assam Rural Infrastructure and Agricultural Services Society GOVERNMENT OF ASSAM TABLE OF CONTENTS 1. INTRODUCTION ……………………………………………………………………. 1 1.1 Background 1.2 Citizen Centered Service Delivery (CCSD) Reform Project 1.3 Social Assessment 1.4 Tribal Development Plan 1.5 Structure of the Report 2. TRIBAL SCENARIO IN ASSAM …………………………………………………... 6 2.1 Assam at a glance 2.2 Demographic & socio-economic profile of tribal and related issues 2.3. Identification of Indigenous People 2.4. Governance and Administration 2.5. The Scheduled Areas 2.6. Need for dedicated attention to Tribal 2.7. Tribal Development Plan 3. LEGAL AND INSTITUTIONAL FRAMEWORK ………………………………….. 14 3.1. Introduction 3.2. Constitutional Safeguards 3.3 Provision of Scheduled Areas under 6th Schedule of the Constitution 3.4. Autonomous Tribal Councils established by State Legislations 3.5. Relevant legal provisions to safeguard tribal interests 3.6. Institutional arrangements for tribal development 4. STAKEHOLDER MAPPING AND CONSULTATIONS …………………………... 21 4.1. Introduction 4.2. Project stakeholders & beneficiaries 4.3. Consultations with citizen in select districts 4.4. Consultations with tribal people and related stakeholders 4.5 Recommendation from Stakeholder Consultation 4.6. Key findings from Social Assessment and Issues of significance 5. TRIBAL DEVELOPMENT PLAN ………………………………………………….. 26 5.1 Introduction 5.2. Objective of Tribal Development Plan 5.3. Strategies for Tribal Development Plan 5.4. Capacity Building and Change Management 5.5 Implementation Arrangements 5.6 RTPS Delivery Unit 5.7 Budgets for Tribal Development Plan 5.8 Monitoring & Evaluation Mechanism 5.9 Grievance Redress Mechanism ANNEXURES 1.