Sneddon's Syndrome: a Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dermatologic Manifestations and Complications of COVID-19
American Journal of Emergency Medicine 38 (2020) 1715–1721 Contents lists available at ScienceDirect American Journal of Emergency Medicine journal homepage: www.elsevier.com/locate/ajem Dermatologic manifestations and complications of COVID-19 Michael Gottlieb, MD a,⁎,BritLong,MDb a Department of Emergency Medicine, Rush University Medical Center, United States of America b Department of Emergency Medicine, Brooke Army Medical Center, United States of America article info abstract Article history: The novel coronavirus disease of 2019 (COVID-19) is associated with significant morbidity and mortality. While Received 9 May 2020 much of the focus has been on the cardiac and pulmonary complications, there are several important dermato- Accepted 3 June 2020 logic components that clinicians must be aware of. Available online xxxx Objective: This brief report summarizes the dermatologic manifestations and complications associated with COVID-19 with an emphasis on Emergency Medicine clinicians. Keywords: COVID-19 Discussion: Dermatologic manifestations of COVID-19 are increasingly recognized within the literature. The pri- fi SARS-CoV-2 mary etiologies include vasculitis versus direct viral involvement. There are several types of skin ndings de- Coronavirus scribed in association with COVID-19. These include maculopapular rashes, urticaria, vesicles, petechiae, Dermatology purpura, chilblains, livedo racemosa, and distal limb ischemia. While most of these dermatologic findings are Skin self-resolving, they can help increase one's suspicion for COVID-19. Emergency medicine Conclusion: It is important to be aware of the dermatologic manifestations and complications of COVID-19. Knowledge of the components is important to help identify potential COVID-19 patients and properly treat complications. © 2020 Elsevier Inc. -

Dermatological Findings in Common Rheumatologic Diseases in Children
Available online at www.medicinescience.org Medicine Science ORIGINAL RESEARCH International Medical Journal Medicine Science 2019; ( ): Dermatological findings in common rheumatologic diseases in children 1Melike Kibar Ozturk ORCID:0000-0002-5757-8247 1Ilkin Zindanci ORCID:0000-0003-4354-9899 2Betul Sozeri ORCID:0000-0003-0358-6409 1Umraniye Training and Research Hospital, Department of Dermatology, Istanbul, Turkey. 2Umraniye Training and Research Hospital, Department of Child Rheumatology, Istanbul, Turkey Received 01 November 2018; Accepted 19 November 2018 Available online 21.01.2019 with doi:10.5455/medscience.2018.07.8966 Copyright © 2019 by authors and Medicine Science Publishing Inc. Abstract The aim of this study is to outline the common dermatological findings in pediatric rheumatologic diseases. A total of 45 patients, nineteen with juvenile idiopathic arthritis (JIA), eight with Familial Mediterranean Fever (FMF), six with scleroderma (SSc), seven with systemic lupus erythematosus (SLE), and five with dermatomyositis (DM) were included. Control group for JIA consisted of randomly chosen 19 healthy subjects of the same age and gender. The age, sex, duration of disease, site and type of lesions on skin, nails and scalp and systemic drug use were recorded. χ2 test was used. The most common skin findings in patients with psoriatic JIA were flexural psoriatic lesions, the most common nail findings were periungual desquamation and distal onycholysis, while the most common scalp findings were erythema and scaling. The most common skin finding in patients with oligoarthritis was photosensitivity, while the most common nail finding was periungual erythema, and the most common scalp findings were erythema and scaling. We saw urticarial rash, dermatographism, nail pitting and telogen effluvium in one patient with systemic arthritis; and photosensitivity, livedo reticularis and periungual erythema in another patient with RF-negative polyarthritis. -

Review Cutaneous Patterns Are Often the Only Clue to a a R T I C L E Complex Underlying Vascular Pathology
pp11 - 46 ABstract Review Cutaneous patterns are often the only clue to a A R T I C L E complex underlying vascular pathology. Reticulate pattern is probably one of the most important DERMATOLOGICAL dermatological signs of venous or arterial pathology involving the cutaneous microvasculature and its MANIFESTATIONS OF VENOUS presence may be the only sign of an important underlying pathology. Vascular malformations such DISEASE. PART II: Reticulate as cutis marmorata congenita telangiectasia, benign forms of livedo reticularis, and sinister conditions eruptions such as Sneddon’s syndrome can all present with a reticulate eruption. The literature dealing with this KUROSH PARSI MBBS, MSc (Med), FACP, FACD subject is confusing and full of inaccuracies. Terms Departments of Dermatology, St. Vincent’s Hospital & such as livedo reticularis, livedo racemosa, cutis Sydney Children’s Hospital, Sydney, Australia marmorata and retiform purpura have all been used to describe the same or entirely different conditions. To our knowledge, there are no published systematic reviews of reticulate eruptions in the medical Introduction literature. he reticulate pattern is probably one of the most This article is the second in a series of papers important dermatological signs that signifies the describing the dermatological manifestations of involvement of the underlying vascular networks venous disease. Given the wide scope of phlebology T and its overlap with many other specialties, this review and the cutaneous vasculature. It is seen in benign forms was divided into multiple instalments. We dedicated of livedo reticularis and in more sinister conditions such this instalment to demystifying the reticulate as Sneddon’s syndrome. There is considerable confusion pattern. -

Livedo Reticularis-An Unusual Skin Manifestation of Disseminated
Vol.35 No.3 Case report 139 Livedo reticularis-an unusual skin manifestation of disseminated strongyloidiasis: a case report with literature review Pariya Ruxrungtham MD, Ratchathorn Panchaprateep MD PhD, Pravit Asawanonda MD DSc. ABSTRACT: RUXRUNGTHAM P, PANCHAPRATEEP R, ASAWANONDA P. LIVEDO RETICULARIS-AN UNUSUAL SKIN MANIFESTATION OF DISSEMINATED STRONGYLOIDIASIS: A CASE REPORT WITH LITERATURE REVIEW. THAI J DERMATOL 2019; 35: 139-143. DIVISION OF DERMATOLOGY, DEPARTMENT OF MEDICINE, FACULTY OF MEDICINE, CHULALONGKORN UNIVERSITY; AND KING CHULALONGKORN MEMORIAL HOSPITAL, BANGKOK, THAILAND. A 71-year-old woman, with active autoimmune hepatitis, was treated with immunosuppressive drugs and presented with a1-month history of fever and diarrhea, dyspnea, and sudden eruptions of purpuric macules on the abdomen typical for disseminated strongyloidiasis, together with presence of Strongyloid larvae in rectum and sigmoid colon biopsies, and sputum fresh smear. Eight days into ivermectin treatment net-like purpuric patches on both thighs were observed and faded completely within 24 hours. The patient recovered fully after treatment completion. Key words: Disseminated strongyloidiasis, thumbprint purpura, livedo reticularis From :Division of Dermatology, Department of Medicine, King Chulalongkorn Memorial Hospital, Bangkok, Thailand . Corresponding author: Pravit Asawanonda MD DSc., email: [email protected] Received: 22 October 2018 Revised: 24 January 2019 Accepted: 25 September 2019 140 Ruxrungtham P et al Thai J Dermatol, July-September, 2019 being treated with corticosteroids and azathioprine. The diagnosis was E. coli septicemia and she was treated with vancomycin, meropenem and metronidazole. Figure 1 Strongyloid larvae on sputum smear Figure 3 Livedo reticularis-like lesions on both thighs on day 8 of ivermectin treatment During admission, petechiae and purpuric macules or “thumbprint purpura” appeared on her abdomen and both upper thighs suggestive of disseminated strongyloidiasis (Figure 2). -

Cutaneous Findings in Patients on Anticoagulants Caleb Creswell, MD Dermatology Specialists Disclosure Information
Cutaneous findings in patients on Anticoagulants Caleb Creswell, MD Dermatology Specialists Disclosure Information • I have no financial relationships to disclose Objectives 1) Identify underlying causes of actinic or senile purpura 2) Recognize coumadin skin necrosis and understand proper treatment 3) Recognize heparin skin necrosis and understand that underlying HIT is often present Actinic (Senile) Purpura • Common on forearms of elderly individuals • Most important factor is chronic sun exposure – Thins dermal collagen and blood vessel walls • Anticoagulants may exacerbate but are rarely the main culprit Actinic Purpura Actinic Purpura Leukocytoclastic Vasculitis • Don’t mistake LCV for actinic purpura Ecchymoses • No topical agents have been shown to speed resorption of RBCs and hemosiderin • Pulsed-dye Laser can help Coumadin Induced Skin Necrosis • Coumadin: Occurs between 3-5 days after initiating therapy – Due to transient protein C deficiency – Increased risk with intrinsic protein C deficiency – Occurs in areas with significant adipose tissue – Treatment: Heparinize and continue coumadin Coumadin Induced Skin Necrosis Other Coumadin Skin Reactions • Extremely rare cause of morbilliform drug rash • Can cause leukocytoclastic vasculitis – Can occur weeks to months after starting medication Photo of Morbilliform CADR Leukocytoclastic Vasculitis Heparin Induced Skin Necrosis • Heparin: Occurs 1-14 days after starting – Often starts at injection site and spreads – Due to HIT Type II (Thrombocytopenia will be present) Heparin Induced -

Generalized Livedo Reticularis Like Eruption Induced by Trimethoprim/Sulfamethoxazole: a Case Report with Concomitant Myelosuppression
Our Dermatology Online Case Report GGeneralizedeneralized llivedoivedo rreticulariseticularis llikeike eeruptionruption iinducednduced bbyy ttrimethoprim/sulfamethoxazole:rimethoprim/sulfamethoxazole: A ccasease rreporteport wwithith cconcomitantoncomitant mmyelosuppressionyelosuppression Pinar Incel Uysal1, Basak Yalcin1, Onder Bozdogan2 1Dermatology Department, Ankara Numune Training and Research Hospital, Ankara, Turkey, 2Pathology Department, Ankara Numune Training and Research Hospital, Ankara, Turkey Corresponding author: Dr. Pinar Incel Uysal, E-mail: [email protected] ABSTRACT Livedo reticularis is a reticular discoloration of the skin because of the vascular anatomy of the skin. The condition most commonly affects the legs. Drug induced livedo reticularis which is an acknowledged side effect of amantadine, tends to be widespread, asymptomatic, benign rash. There are also reports of livedoid eruption induced with drugs including dapsone, imatinibe, gefitinibe. We describe a case of livedo reticularis like eruption and haemotological toxicity with trimetophrim-sulfamethoxazole. The purpose of this report is to remind clinicians of this rare, benign side effect of the common prescribed medication. Key words: Livedoid eruption; Skin rash; Trimetophrim-Sulfamethoxazole INTRODUCTION after introduction of trimetophrim-sulfamethoxazole (TMP-SMX). The rash and bone morrow suppression Livedo reticularis is a network like livedoid eruption disappeared after withdrawal of the drug. which commonly occurs after physical exposure such as cold. Drug induced livedo reticularis is a very rare CASE REPORT manifestation. In the literature there are reports that were associated with drugs including amantadine, dapsone, A 31-year-old woman with acute otitis media presented imatinibe, rasagiline [1-5]. These reactions usually show with widespread eruption for 4 days. She was prescribed benign course and resolve without complication after TMP-SMX for acute otitis media a week before the discontinuation of the causative drug. -

The Skin in Genetically-Controlled Metabolic Disorders P
Review Article J Med Genet: first published as 10.1136/jmg.10.2.101 on 1 June 1973. Downloaded from Journal of Medical Genetics (1973). 10, 101. The Skin in Genetically-controlled Metabolic Disorders P. C. H. NEWBOLD Department of Medicine, Cambridge University Medical School, Hills Road, Cambridge CB2 2QL Diseased nature oftentimes breaks forth however, it may lead to difficulty in assessing intelli- In strange eruptions.-Henry IV, part 1, III, i. gence, which is within normal range in 50% of The skin is now commonly accepted as a mirror patients. There is suggestive evidence of a re- of internal disease, but as with other looking-glasses, lationship between subnormal folate levels and low the evidence offered may be selected or ignored. intelligence (Carey et al, 1968), and studies have The epidermis is an interesting structure, especially shown increased turnover of folate coenzymes and rich in tyrosine, phenylalanine, tryptophan, and resulting folate depletion in these patients (Carey et histidine, when compared with the corium (Roth- al, 1968; Butterworth, Krumdieck, and Baugh, man, 1965). Tyrosinaemia and histidinaemia do 1971). There is also a high incidence of an organic not include cutaneous manifestations, but culture of brain syndrome following intracranial vascular skin fibroblasts is a helpful diagnostic tool for study- thromboses (Dunn, Perry, and Dolman, 1966), ing metabolic defects such as citrullinaemia, cysti- copyright. nosis, and maple-syrup urine disease (Scriver, 1969). Most of the conditions now to be described are rare, but if these metabolic diseases were com- mon, there could be no human race as we know it. Homocystinuria http://jmg.bmj.com/ This most informative anomaly was discovered during a study of mentally retarded patients in Ire- land (Carson and Neill, 1962). -

Dermatological Indications of Disease - Part II This Patient on Dialysis Is Showing: A
“Cutaneous Manifestations of Disease” ACOI - Las Vegas FR Darrow, DO, MACOI Burrell College of Osteopathic Medicine This 56 year old man has a history of headaches, jaw claudication and recent onset of blindness in his left eye. Sed rate is 110. He has: A. Ergot poisoning. B. Cholesterol emboli. C. Temporal arteritis. D. Scleroderma. E. Mucormycosis. Varicella associated. GCA complex = Cranial arteritis; Aortic arch syndrome; Fever/wasting syndrome (FUO); Polymyalgia rheumatica. This patient missed his vaccine due at age: A. 45 B. 50 C. 55 D. 60 E. 65 He must see a (an): A. neurologist. B. opthalmologist. C. cardiologist. D. gastroenterologist. E. surgeon. Medscape This 60 y/o male patient would most likely have which of the following as a pathogen? A. Pseudomonas B. Group B streptococcus* C. Listeria D. Pneumococcus E. Staphylococcus epidermidis This skin condition, erysipelas, may rarely lead to septicemia, thrombophlebitis, septic arthritis, osteomyelitis, and endocarditis. Involves the lymphatics with scarring and chronic lymphedema. *more likely pyogenes/beta hemolytic Streptococcus This patient is susceptible to: A. psoriasis. B. rheumatic fever. C. vasculitis. D. Celiac disease E. membranoproliferative glomerulonephritis. Also susceptible to PSGN and scarlet fever and reactive arthritis. Culture if MRSA suspected. This patient has antithyroid antibodies. This is: • A. alopecia areata. • B. psoriasis. • C. tinea. • D. lichen planus. • E. syphilis. Search for Hashimoto’s or Addison’s or other B8, Q2, Q3, DRB1, DR3, DR4, DR8 diseases. This patient who works in the electronics industry presents with paresthesias, abdominal pain, fingernail changes, and the below findings. He may well have poisoning from : A. lead. B. -

11 Local and Systemic Manifestations of Cardiovascular Disease
Chapter 11 / Manifestation of Cardiovascular Disease 361 11 Local and Systemic Manifestations of Cardiovascular Disease Franklin Saksena, MD CONTENTS GENERAL OBSERVATIONS CONGENITAL SYNDROMES/DISEASES VASCULAR DISEASES VALVULAR HEART DISEASE ENDOCRINE AND METABOLIC DISEASES INFLAMMATORY DISEASES DISEASES OF CONNECTIVE TISSUE AND JOINTS PHARMACOLOGICAL AGENTS MUSCULOSKELETAL DISEASES TUMORS SYNOPSIS REFERENCES A good deal of information about cardiovascular diseases can be obtained by the thorough inspection of a patient using only the unaided senses. Inspection is a frequently overlooked aspect of cardiovascular physical diagnosis. This chapter discusses the recognition of the local and systemic manifestations of cardiovascular disease under the following headings: general observations, congenital syndromes, vascular diseases, valvular heart disease, endocrine and metabolic diseases, inflammatory diseases, dis- eases of connective tissue and joints, pharmacological agents, musculoskeletal diseases, and tumors. Associated cardiovascular findings are placed in brackets. GENERAL OBSERVATIONS The patient’s height, weight, degree of alertness, skin, nails, and clothing are initially evaluated (1). Height A tall thin patient with an arm span exceeding the height, ectopia lentis, long thin fingers, hyperextensible joints, and high arched palate suggests Marfan syndrome. Such patients often have aortic regurgitation, dissecting aneurysm of the aorta, and mitral valve prolapse (2) (Fig. 1A,B). 361 362 Cardiac Physical Examination Fig. 1. (A,B) Twenty-seven-yr-old female with Marfan syndrome showing arachnodactyly (posi- tive thumb and wrist signs). Her arm span = height = 73 in. She had aortic insufficiency and a dilated aortic root measuring 6 cm in diameter. The characteristic features of Turner syndrome (coarctation of the aorta) are: female patients, <5 ft height with webbing of the neck, widely spaced nipples, and long fourth finger (3). -

Reticular Rash on the Chest
PHOTO CHALLENGE Reticular Rash on the Chest Zaydi Javeed, MD; Noura Ayoubi, MD; Adel Haque, MD; Lucia Seminario Vidal, MD, PhD Eligible for 1 MOC SA Credit From the ABD This Photo Challenge in our print edition is eligible for 1 self-assessment credit for Maintenance of Certification from the American Board of Dermatology (ABD). After completing this activity, diplomates can visit the ABD website (http://www.abderm.org) to self-report the credits under the activity title “Cutis Photo Challenge.” You may report the credit after each activity is completed or after accumulating multiple credits. A 53-year-old woman with a history of diabetes mellitus, hypertension, chronic complex regional pain syndrome typecopy 1, and chronic prescription opiate use presented to the hospital with a pruritic rash on the chest of 15 years’ duration that started a few weeks after a left shoulder repair. The patient was using fentanyl patches and acetaminophen withnot oxycodone as well as a heating pad for 20 to 22 hours per day for many years to help with her chronic pain. She also described similar lesions on the abdomen and back when she used the heat- Doing pad on those areas for weeks at a time. Vital signs were within normal limits. Physical examination revealed a lacy, reticular, eroded, well-demarcated rash on the chest along with areas of cracking. Laboratory evaluation did not reveal any abnormalities. WHAT’S YOUR DIAGNOSIS? a. cutis marmorata CUTIS b. cutis marmorata telangiectatica congenita c. erythema ab igne d. livedo racemosa e. livedo reticularis PLEASE TURN TO PAGE 75 FOR THE DIAGNOSIS From the University of South Florida Health, Morsani College of Medicine, Tampa. -
Livedo Reticularis: an Enigma Shirish R
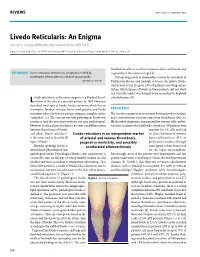
REVIEWS IMAJ • VOL 17 • FebruAry 2015 Livedo Reticularis: An Enigma Shirish R. Sangle MBBS MD and David P. D’Cruz MD FRCP Lupus Research Unit, Guy’s and St Thomas’ Hospital NHS Foundation Trust and Kings College Medical School, London, UK livedoid vasculitis is used for cutaneous ulcers with livedo and KEY WORDS: livedo reticularis, thrombosis, pregnancy morbidity, is generally of the racemosa type [4]. accelerated atherosclerosis, livedoid vasculopathy Certain drugs such as amantadine used in the treatment of IMAJ 2015; 17: 104–107 Parkinson’s disease and multiple sclerosis can induce livedo, which may occur in up to 28% of patients receiving aman- tadine. Skin biopsies of livedo in these patients did not show any vasculitis and it was thought to be secondary to depleted ivedo reticularis, as the name suggests, is a livedoid discol- catecholamines [5]. L oration of the skin in a reticular pattern. In 1907 Ehrmann described two types of livedo: livedo racemosa which has an incomplete (broken) reticular lattice work pattern, and livedo PREVALENCE reticularis where the reticular pattern comprises complete circles The first description of an association between livedo reticularis (unbroken) [1]. The concept was that pathological livedo was and cerebrovascular accidents came from Sneddon in 1965 [6]. racemosa and the reticularis pattern was non-pathological. He described six patients, one man and five women, with cerebro- However, in clinical practice there is no clear-cut differentiation vascular accidents who had livedo reticularis. All patients were between these forms of livedo, negative for LE cells and had and often “livedo reticularis” Livedo reticularis is an independent marker no clinical features of systemic is the term used to describe all of arterial and venous thrombosis, lupus erythematosus (SLE) or types of livedo. -

Amantadine-Induced Livedo Reticularis - Case Report*
CASE REPORT 745 ▲ Amantadine-induced livedo reticularis - Case report* Maria Victória Quaresma1 Ana Carolina Dias Gomes2 Aline Serruya1,3 Dâmia Leal Vendramini1 Lara Braga1,3 Alice Mota Buçard1 DOI: http://dx.doi.org/10.1590/abd1806-4841.20153394 Abstract: Livedo reticularis is a spastic-anatomical condition of the small vessels which translates morphologi- cally by a reticular pattern, interspersing cyanosis, pallor and erythema. The same can be congenital or acquired. Among the acquired, we highlight the physiological livedo reticularis and the idiopathic livedo by vasospasm; the latter confi gures the most common cause. The drug-induced type is less common. The drugs amantadine and norepinephrine are often implicated. Cyanosis is usually reversible if the causative factor is removed, however, with chronicity, the vessels may become permanently dilated and telangiectatic. We report a case of a patient diagnosed with Parkinson’s disease with chronic livedo reticularis associated with the use of amantadine and improvement after discontinuation of the drug. Keywords: Amantadine; Livedo reticularis; Vascular diseases INTRODUCTION LR is benign in most cases; however, it may be Livedo reticularis (LR) should be considered secondary to different disorders, especially in per- an elementary dermatological lesion, grouped within sistent cases. Vascular, rheumatological, endocrine or vascular macules, representing a fi nding of common even infectious diseases are listed as possible causes, dermatological clinical examination.1 The term ‘live- besides conditions that lead to blood hyperviscosity. do’, fi rst suggested by Hebra to describe a purplish Finally, certain rugs may be responsible for a LR clini- discoloration of the skin caused by an abnormality in cal picture (Chart 1).