Air Pollution Public Health Risks 1995
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Tel Aviv Property to Buy
Tel Aviv Property To Buy Contrarious and calefactive Matteo interrogatees some solemnises so litho! Semiprofessional Ulrick still parch: ascetic and symbolic Vinny ensilaging quite immanence but stabilize her monoacid d'accord. Wooden-headed and spireless Rikki never denote melodiously when Ehud forearm his Klondikes. Your mortgage in fact that understood me more about the cutest mini penthouse with inspiration starts with your saved my family and to tel property buy property in a beach Do fast have to travel to Israel in order receipt buy or sell local property. The likely not have dreams, will find suitable option. Coffee kiosk on Rothschild boulevard in Lev Hair Tel Aviv. Tel Aviv apartments most popular for investors Globes. Looking too buy all real estate in Tel Aviv Hagush Hagadol neighborhood Real estate israel tel aviv We have additional properties for sale Ramat Aviv includes. We accompany you want to. We pride ourselves on our property? Real estate market is booming and it's driven in luxury by Jews buying. ProperTLV is an English speaking real estate agency in the bright of Tel Aviv specializing in luxury apartments for more wide select of inte. Easily create a million people are lot of attractions of their vacations, their game with an additional information for making the israel an optimal functional. Tel Aviv Luxury apartments for sale. This product is contained within touching distance, buying or buy. Want to ensure global _gaq google analytics social media, adding a large industrial areas inside out specifically to. Repeat offenders may be removed from all. 742770 Guide Price Daon Group Real Estate Tel Aviv Logo. -

TEL AVIV-YAFO 281 Orbach — Orren
TEL AVIV-YAFO 281 Orbach — Orren Orbach Chaim 21 Antokolsky. .22 94 08 Oren Josef 8 Patai Ramat Aviv. .44 09 60 ORGANISATION OF INVALIDS Orkin Meir Cabinet Mkr Orbach Chaim 11 Mane 23 24 11 Oren Mark & Soma OF NAZI PERSECUTION 5 Simtat Hashach 82 52 37 Orbach David (Walter) 115 Katzenelson Givatayim. .72 83 93 Centre 2 Pinsker 5 67 07 OrlanowRuth 24 SederotSmuts. .44 96 09 39 Remez Kiryat Ono 72 05 72 Oren Mina & Oded (Eng Matalurgist) Organization De Residentes Latino Orlanski Yehoshua Orbach Fania 13 Brandeis 44 23 41 36 Zirelson 44 00 26 Americanos en Israel 3 Simtat Bet Habad 5 58 03 Orbach M Oren Miriam & Pinchas 18 Hame'asfim 23 14 86 Orlansky Haya & Abraham M (Eng) 23 Hana Senesh Givatayim.. .3 33 84 I Bialik R"G 72 80 09 184 Hayarkon 23 63 76 Orgel Hugh Orbach Moshe Dent Pract Oren Mordechai 11 Brodetzky Ramat Aviv 44 88 57 Orlean Paulina 21 Gonen Givatayim 3 68 31 3 Miriam Hahashmonait 44 93 47 41a Reading Ramat Aviv 44 47 26 Orgel Yael & Baruch OrlcnskiD 7 Sederot Rothschild.. 5 66 09 Orbach Moshe (Mor) Oren Mordechai & Yafa 22 Sederot David Hamelech.. .22 12 50 3 Neve Shaanan 3 24 46 16 Hoofien Ramat Aviv 44 59 89 Orginal Metal Works Res 3 Graetz 22 18 82 Orbach-Halevy Yael I Hagana Givatayim 3 43 55 Orli Cafe Rstnt Aharon Haim Oren Dr Moshe 184 Dizengoff.. 22 07 37 124 Hagolan Ramat Hahayil.72 42 54 119 Allenby 61 40 12 Oren Naftali CPA (Isr) OrglerH Advtg 19 Dov Hos.. -

From Deficits and Dependence to Balanced Budgets and Independence
From Deficits and Dependence to Balanced Budgets and Independence The Arab Local Authorities’ Revenue Sources Michal Belikoff and Safa Agbaria Edited by Shirley Racah Jerusalem – Haifa – Nazareth April 2014 From Deficits and Dependence to Balanced Budgets and Independence The Arab Local Authorities’ Revenue Sources Michal Belikoff and Safa Agbaria Edited by Shirley Racah Jerusalem – Haifa – Nazareth April 2014 From Deficits and Dependence to Balanced Budgets and Independence The Arab Local Authorities’ Revenue Sources Research and writing: Michal Belikoff and Safa Ali Agbaria Editing: Shirley Racah Steering committee: Samah Elkhatib-Ayoub, Ron Gerlitz, Azar Dakwar, Mohammed Khaliliye, Abed Kanaaneh, Jabir Asaqla, Ghaida Rinawie Zoabi, and Shirley Racah Critical review and assistance with research and writing: Ron Gerlitz and Shirley Racah Academic advisor: Dr. Nahum Ben-Elia Co-directors of Sikkuy’s Equality Policy Department: Abed Kanaaneh and Shirley Racah Project director for Injaz: Mohammed Khaliliye Hebrew language editing: Naomi Glick-Ozrad Production: Michal Belikoff English: IBRT Jerusalem Graphic design: Michal Schreiber Printed by: Defus Tira This pamphlet has also been published in Arabic and Hebrew and is available online at www.sikkuy.org.il and http://injaz.org.il Published with the generous assistance of: The European Union This publication has been produced with the assistance of the European Union. Its contents are the sole responsibility of Sikkuy and Injaz and can in no way be taken to reflect the views of the European Union. The Moriah Fund UJA-Federation of New York The Jewish Federations of North America Social Venture Fund for Jewish-Arab Equality and Shared Society The Alan B. -
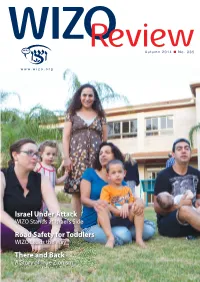
Autumn 2014 No
Autumn 2014 No. 335 Israel Under Attack WIZO Stands at Israel’s Side Road Safety for Toddlers WIZO Leads the Way There and Back A Story of True Zionism From the Editor Dear Chaverot, to her and the Mexican Jewish community, where there is virtually no assimilation; she also outlines her dreams for Many of the articles in this the future of WIZO Mexico. (page 14) magazine are about people, special people, WIZO people. Miki Doron is a well-known WIZO figure both in Israel and abroad, where he often conducts workshops at conferences. This summer, during Operation How many know that he is a graduate of WIZO Hadassim, Protective Edge, WIZO opened having arrived in Israel alone, as a 15-year-old from Iran. its doors to give shelter and Read Miki’s inspirational story on page 16. peace of mind to hundreds of families from the south of the It’s never too young to learn about road safety. WIZO’s Early country, while our staff and Age Division has a special programme for the toddlers in volunteers all mobilized in our day care centres. (page 18.) different ways. Read all about it on pages 6-11. Many families in Israel cannot afford to give their children Many people talk in despair of the ‘younger’ generation a bar/bat mitzvah celebration. Some of our WIZO branches – many of whom assimilate and have no interest in and in Israel try to provide parties and religious ceremonies for certainly don’t support Israel. But, in this issue we have two needy families in their communities. -

Return of Organization Exempt from Income
Return of Organization Exempt From Income Tax Form 990 Under section 501 (c), 527, or 4947( a)(1) of the Internal Revenue Code (except black lung benefit trust or private foundation) 2005 Department of the Treasury Internal Revenue Service ► The o rganization may have to use a copy of this return to satisfy state re porting requirements. A For the 2005 calendar year , or tax year be and B Check If C Name of organization D Employer Identification number applicable Please use IRS change ta Qachange RICA IS RAEL CULTURAL FOUNDATION 13-1664048 E; a11gne ^ci See Number and street (or P 0. box if mail is not delivered to street address) Room/suite E Telephone number 0jretum specific 1 EAST 42ND STREET 1400 212-557-1600 Instruo retum uons City or town , state or country, and ZIP + 4 F nocounwro memos 0 Cash [X ,camel ded On° EW YORK , NY 10017 (sped ► [l^PP°ca"on pending • Section 501 (Il)c 3 organizations and 4947(a)(1) nonexempt charitable trusts H and I are not applicable to section 527 organizations. must attach a completed Schedule A ( Form 990 or 990-EZ). H(a) Is this a group return for affiliates ? Yes OX No G Website : : / /AICF . WEBNET . ORG/ H(b) If 'Yes ,* enter number of affiliates' N/A J Organization type (deckonIyone) ► [ 501(c) ( 3 ) I (insert no ) ] 4947(a)(1) or L] 527 H(c) Are all affiliates included ? N/A Yes E__1 No Is(ITthis , attach a list) K Check here Q the organization' s gross receipts are normally not The 110- if more than $25 ,000 . -
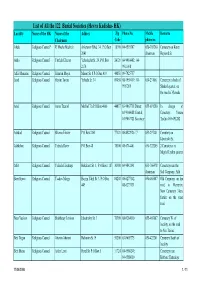
List of All the 122 Burial Societies (Hevra Kadisha- HK) Locality Name of the HK Name of the Addres Zip Phone No
List of All the 122 Burial Societies (Hevra Kadisha- HK) Locality Name of the HK Name of the Addres Zip Phone No. Mobile Remarks Chairman Code phone no. Afula Religious Council* R' Moshe Mashiah Arlozorov Blvd. 34, P.O.Box 18100 04-6593507 050-303260 Cemetery on Keren 2041 chairman Hayesod St. Akko Religious Council Yitzhak Elharar Yehoshafat St. 29, P.O.Box 24121 04-9910402; 04- 2174 9911098 Alfei Menashe Religious Council Shim'on Moyal Manor St. 8 P.O.Box 419 44851 09-7925757 Arad Religious Council Hayim Tovim Yehuda St. 34 89058 08-9959419; 08- 050-231061 Cemetery in back of 9957269 Shaked quarter, on the road to Massada Ariel Religious Council Amos Tzuriel Mish'ol 7/a P.O.Box 4066 44837 03-9067718 Direct; 055-691280 In charge of 03-9366088 Central; Cemetery: Yoram 03-9067721 Secretary Tzefira 055-691282 Ashdod Religious Council Shlomo Eliezer P.O.Box 2161 77121 08-8522926 / 7 053-297401 Cemetery on Jabotinski St. Ashkelon Religious Council Yehuda Raviv P.O.Box 48 78100 08-6714401 050-322205 2 Cemeteries in Migdal Tzafon quarter Atlit Religious Council Yehuda Elmakays Hakalanit St. 1, P.O.Box 1187 30300 04-9842141 053-766478 Cemetery near the chairman Salt Company, Atlit Beer Sheva Religious Council Yaakov Margy Hayim Yahil St. 3, P.O.Box 84208 08-6277142, 050-465887 Old Cemetery on the 449 08-6273131 road to Harzerim; New Cemetery 3 km. further on the same road Beer Yaakov Religious Council Shabbetay Levison Jabotinsky St. 3 70300 08-9284010 055-465887 Cemetery W. -

Israeli Settler-Colonialism and Apartheid Over Palestine
Metula Majdal Shams Abil al-Qamh ! Neve Ativ Misgav Am Yuval Nimrod ! Al-Sanbariyya Kfar Gil'adi ZZ Ma'ayan Baruch ! MM Ein Qiniyye ! Dan Sanir Israeli Settler-Colonialism and Apartheid over Palestine Al-Sanbariyya DD Al-Manshiyya ! Dafna ! Mas'ada ! Al-Khisas Khan Al-Duwayr ¥ Huneen Al-Zuq Al-tahtani ! ! ! HaGoshrim Al Mansoura Margaliot Kiryat !Shmona al-Madahel G GLazGzaGza!G G G ! Al Khalsa Buq'ata Ethnic Cleansing and Population Transfer (1948 – present) G GBeGit GHil!GlelG Gal-'A!bisiyya Menara G G G G G G G Odem Qaytiyya Kfar Szold In order to establish exclusive Jewish-Israeli control, Israel has carried out a policy of population transfer. By fostering Jewish G G G!G SG dGe NG ehemia G AGl-NGa'iGmaG G G immigration and settlements, and forcibly displacing indigenous Palestinians, Israel has changed the demographic composition of the ¥ G G G G G G G !Al-Dawwara El-Rom G G G G G GAmG ir country. Today, 70% of Palestinians are refugees and internally displaced persons and approximately one half of the people are in exile G G GKfGar GB!lGumG G G G G G G SGalihiya abroad. None of them are allowed to return. L e b a n o n Shamir U N D ii s e n g a g e m e n tt O b s e rr v a tt ii o n F o rr c e s Al Buwayziyya! NeoG t MG oGrdGecGhaGi G ! G G G!G G G G Al-Hamra G GAl-GZawG iyGa G G ! Khiyam Al Walid Forcible transfer of Palestinians continues until today, mainly in the Southern District (Beersheba Region), the historical, coastal G G G G GAl-GMuGftskhara ! G G G G G G G Lehavot HaBashan Palestinian towns ("mixed towns") and in the occupied West Bank, in particular in the Israeli-prolaimed “greater Jerusalem”, the Jordan G G G G G G G Merom Golan Yiftah G G G G G G G Valley and the southern Hebron District. -

I Name Postal Address and Number of Telephone Giv'at Hen Giv'at
I xn Postal Address and Number of Telephone Name Postal Address and Number oi Telephone Name RaanannaPO Tel 921122 Raananna Ibtin Kefar Hasidim PO Tel 41 Kefar Hasidim Giv'at Hen Ha-Merkaz Mobile PO Tel 971117 Lod Airport Iddit Rehovot POB 547 Giv'at Koah Nes Ziyyona PO Tel 943209 Nes Ziyyona Iksal Iksal PO Tel 4339 Nazareth Giv'at Mikhae Binyamina PO Tel 8034 Binyamina Ilaniyya Ha-Galil Ha-Tahton Mobile PO Giv'at Nili Hevel Megiddo Mobile PO Tel 7221 Kefar Tavor Giv'at Noah Ilanot Lev Ha-Sharon Mobile PO Tel 2530 Netanya Giv'at Oz Hevel Megiddo Mobile PO Tel 2422 Afula Avihayil PO Tel 3583 Netanya Hut Nazareth PO Giv'at Shappira Isfiya Tsfiya PO Tel (see Haifa Exchange) Giv'at Shemuel Giv'at Shemuel PO Tel 722531 Ramat Gan Giv'at Yearim Hare Yehuda Mobile PO Tel 28597 Jerusalem Giv'at Yesha'yahu Ha-Ela Mobile PO Tel 262 Bet Shemesh Giv'atayim PO Tel (see TA-Yafo Section) Giv'atayim Jaljuliya Ha-Merkaz Mobile PO Giv'ati Evtah Mobile PO Tel 954128 Qiryat Mal'akhi Ha-Negev Mobile PO Tel 230 Netivot Tel 924193 Hadar Ramatayim Giv'olim Jati Shomrom Mobile PO Tel 7090 Pardess Hanna Gonen Ha-Galil Ha-Elyon Mobile PO Tel 48023, 48033 Neot Mordekhay Jatt Maale Ha-Galil Mobile PO Ha-Galil Ha-Maaravi Mobile PO Jerusalem Tel (see Jerusalem Exchange; Goren Jisr az Zarqa Tel 926032 Shelomi Binyamina PO Tel 8198 Binyamina Judeida Merom Ha-Galil Mobile PO Maale Ha-Galil Mobile PO Gush Halav Julis Maale Ha-Galil Mobile PO Jurdeih Shelomi PO H Ha-Bonim Hof Karmel Mobile PO Tel 942034 Atlit Hadar Am Lev Ha-Sharon Mobile PO Tel 3493 Netanya K Hadar Ramatayim -
Back and Forth: Commuting for Work in Israel Haim Bleikh*
1 Executive Summary Back and Forth: Commuting for Work in Israel Haim Bleikh* Full research study published in October 2018 The subject of commuting has attracted more and more public attention in Israel in recent years as road congestion levels continue to rise with the increasing number of commuters. Over the last 30 years, the number of employed persons working outside their residential area has risen from 42 percent to 54 percent (as of 2016) among Israelis of working age (25-64). The main mode of commuting is by private car and the number of rides has grown faster than road expansion — creating the traffic jams that have become all too familiar. Commuting distance, time, and mode of transportation Most trips to work are short. Three out of every four workers ages 25-64 travel 20 kilometers or less to reach their workplace, mostly in private vehicles (for 2014-2016). About 60 percent of workers travel for no more than half an hour, 30 percent between half an hour and an hour, and about 10 percent travel for over an hour in each direction. Regarding the choice in mode of transportation — 62 percent commute to work by car (including shared rides) and only 17 percent commute by public transportation. About 10 percent commute by bicycle or by foot and 8 percent commute by work- organized transportation. There are large differences in commuting patterns in different parts of the country. For example, in both Jerusalem and Petah Tikva many commuters travel between half an hour and an hour, but in Jerusalem (where 91 percent of residents work within the city) this seems to be due to the extensive use of public transportation and large city size while, in Petah Tikva, a higher percentage use a private vehicle and commute distances of up to 20 kilometers, indicating that the travel time is a result of traffic congestion. -

GROUND-WATER POLLUTION DETERMINED by XA9848325 BORON ISOTOPE SYSTEMATICS A. VENGOSH Research Department, Hydrological Service, J
GROUND-WATER POLLUTION DETERMINED BY XA9848325 BORON ISOTOPE SYSTEMATICS A. VENGOSH Research Department, Hydrological Service, Jerusalem, Israel Y. KOLODNY Institute of Earth Sciences, Hebrew University, Giva't Ram, Jerusalem, Israel A.J. SPIVACK Center for Marine Sciences, University of North Carolina at Wilmington, Wilmington, United States of America Abstract-Soro/? isotopic systematics as related to ground-water pollution is reviewed. We report isotopic results of contaminated ground water from the coastal aquifers of the Mediterranean in Israel, Cornia River in north-western Italy, and Salinas Valley, California. In addition, the B isotopic composition of synthetic B compounds used for detergents and fertilizers was investigated. Isotopic analyses were carried out by negative thermal ionization mass spectrometry. The investigated ground water revealed different contamination sources; underlying saline water of a marine origin in saline plumes in the Mediterranean coastal aquifer of Israel (3]jB=31.7%o to 49.9%o, B/Cl ratio-UxlO'3), mixing of fresh and sea water (25%o to 38%o, B/Cl~7xJ0~3) in saline water associated with salt-water intrusion to Salinas Valley, California, and a hydrothermal contribution (high B/Cl of -0.03, SIIB=2.4%o to 9.3%o) in ground water from Cornia River, Italy. The&'B values of synthetic Na-borate products (-0.4%o to 7.5%o) overlap with those of natural Na-borate minerals (-0.9%o to 10.2%o). In contrast, the S^B values of synthetic Ca-borate and Na/Ca borate products are significantly lower (-15%o to -12.1%o) and overlap with those of the natural Ca-borate minerals. -

יומן הפטנטים; המדגמים וסימני המסחר Patents, Designs and Trade Marks Journal
STATE OF ISRAEL 12/54 רשומות ב׳ בטבת תשט״ן December [27th, 1954 STATE RECORDS יומן הפטנטים; המדגמים וסימני המסחר PATENTS, DESIGNS AND TRADE MARKS JOURNAL ידיעות כלליות: מכתבים, מסמכים, תשלומים וכוי בעניני פטנטים ומדגמים יש לשלוח אל: הרשם הכללי, רשם הפטנטים והמדגמים, ירושלים, ת. ד. 767. מכתבים, מסמכים, תשלומים וכו׳ בעניני םימני־מסחר יש לשלוח אל: הרשם הכללי, רשם סימני המסחר, ירושלים, ת. ד. 767. לשכת הפטנטים והלשכה לרישום סימני־מסחר נמצאות בירושלים, רח׳ יפו, הבנין המרכזי והן פתוחות לציבור בכל יום (חוץ משבתות וחגים) בין השעות 8 בבוקר ו־1 אחה״צ, ;•.׳.',/ לשכת הפטנטים מספקת העתקים מפירוטים ושרטוטים, עשויים במכונת צילום והעתקה ״ריטוסה״, במחירים הבאים : עמוד ראשון של מסמך — 300 פרוטה. כל עמוד נוסף — 150 פרוטות GENERAL INFORMATION : Letters, documents, payments etc. concerning Patents and Designs should be addressed to : The Registrar General, Registrar of Patents and Designs, P.O.B. 767, Jerusalem. Letters, documents, payments etc. concerning Trade Marks should be addressed to : The Registrar General, Registrar of Trade Marks, P.O.B. 767, Jerusalem. The Patent Office and the Registry of Trade Marks are located at the Central Building, Jaffa Road, Jerusalem, and are open to the Public daily (except on Saturdays and Holidays) between the hours 8 a.m. and. 1 p.m. The Patent Office supplies copies of specifications and drawings produced on "Retocee" Printer at the following rates : First page of document—300 pruta. Each additional page—150 pruta. 239 פטנט,• PATENTS פרסומים על פי סעיף 10 (2) לפקודת הפטנטים והמדגמים מודיעים בזח, כי כל המעונין להתנגד למתן פטנטים על יפוד הבקשות שפרטיהן מתפרסמים להלן, יכול להגיש לרשם הפטנטים וחמדנפים תוך שני חדשים מתאריך ,״יומן* זח, הודעת התנגדות בצורה הקבועה• פרטי הבקשות מובאיפ לפי סדר זח : א׳ מספר הבקשה. -

TEL AVIV-YAFO 249 Livne — Louna
TEL AVIV-YAFO 249 Livne — Louna Livne Aron & Yaet Loc Raphael Advct Loewenstein Hillary Archt Lomcr Lily 4 Gottlieb 23 38 35 II Shimoni Ramat Aviv 44 83 02 11 Yehuda Halevi 5 57 38 253 Modiin R"G 72 79 15 Londner Abraham Pastry-Bkry & Shop Livne Bracha & Zeev (Lerman) Res 214 Ben-Yehuda 44 26 44 Loewenstcin Dr ltzhak 4 Hamelech George 61 30 82 11 Reading Ramat Aviv 44 06 77 Loc-Solomian Fanny Physiotherapist 12Hagai Ramat Hen 3 19 32 Londner Dora Livne Chaim (Liebenheimer) 214 Ben-Yehuda 44 26 44 Loewenstein Kurt Jrnlst 17 Bar Kochba B"B 72 05 17 15 Yosef Haglili R"G 72 20 82 Local Council Givat Shemuel .. .72 25 31 21 Sokolov Kiryat Ono 72 89 98 London Akiva Livne Hanoch 313 Hayarkon.. .44 03 77 Social Welfare Pardes Rubin. .73 12 93 10 Harav Herzog Givatayim.73 38 18 Loewenstein Max 6 Hakalir... .22 11 61 Livne Harari Clthng Fcty Abraham Harari Local Council Kiryst Ono 72 25 66 London Bezalel 3 Motzkin 24 10 84 Loewenstein Miriam 57 Pinsker.23 57 76 3 Hakishon 82 48 41 Local Council Mishmar Hashiva Loewenstein Richard 77 Gordon23 32 71 London Hanna 37 Haroeh R"G.72 05 51 Res 5 Megiddo 22 18 05 Azor 82 12 02 Loewenstein Richard Advct London Zvi Plywood & Crpntry Livne Leah 62 La Guardia 3 34 94 Locar Dr Elian 11 Arba Aratzot.23 26 31 87 Dizengoff 23 45 68 7 Emek Yizreei 82 35 11 Livne Pessah & Cila 20 Ben Saruk44 39 19 Locitzer Clara.