Atlas of Acupuncture Points
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bilateral Anomalous Muscle in the Popliteal Fossa & Its Clinical
International Journal of Anatomy and Research, Int J Anat Res 2014, Vol 2(4):614-16. ISSN 2321- 4287 Case Report DOI: 10.16965/ijar.2014.501 BILATERAL ANOMALOUS MUSCLE IN THE POPLITEAL FOSSA & ITS CLINICAL SIGNIFICANCE Sowmya S *, Meenakshi Parthasarathi, Sharmada KL, Sujana M. Department of anatomy, Bangalore Medical College & Research Institute, Bangalore, India. ABSTRACT Muscle variation may occur due to genetic or developmental causes. Some variations may compromise the vascular, muscular or nervous system in the region. Bilateral muscle variation in popliteal fossa is very rare. In present study an instance of bilateral muscle variation in popliteal fossa, arising from different muscles like gastrocnemius and from biceps femoris is recorded. There is no report of such variations. These observations are rare of its kind because of bilateral asymmetrical presence and difference in the origins in different legs. This is the first report as for the literatures available. Clinical and functional importance of such variation is discussed with the morphological aspects of this anomalous muscle. KEY WORDS: Popliteal fossa, Gastrocnemius, Biceps femoris, Popliteal Artery Entrapment Syndrome. Address for Correspondence: Dr.Sowmya S, Assistant Professor, Department of Anatomy, Bangalore Medical College & Research Institute, Bangalore-560002, India. Mobile: +919482476545. E-Mail: [email protected] Access this Article online Quick Response code Web site: International Journal of Anatomy and Research ISSN 2321-4287 www.ijmhr.org/ijar.htm Received: 08 Sep 2014 Peer Review: 08 Sep 2014 Published (O):31 Oct 2014 DOI: 10.16965/ijar.2014.501 Accepted: 22 Sep 2014 Published (P):31 Dec 2014 INTRODUCTION Insertion of muscle slips from biceps femoris into gastrocnemius and into tendocalcaneus have The popliteal fossa is a rhomboidal region been reported [3]. -

Recognizing When a Child's Injury Or Illness Is Caused by Abuse
U.S. Department of Justice Office of Justice Programs Office of Juvenile Justice and Delinquency Prevention Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE U.S. Department of Justice Office of Justice Programs 810 Seventh Street NW. Washington, DC 20531 Eric H. Holder, Jr. Attorney General Karol V. Mason Assistant Attorney General Robert L. Listenbee Administrator Office of Juvenile Justice and Delinquency Prevention Office of Justice Programs Innovation • Partnerships • Safer Neighborhoods www.ojp.usdoj.gov Office of Juvenile Justice and Delinquency Prevention www.ojjdp.gov The Office of Juvenile Justice and Delinquency Prevention is a component of the Office of Justice Programs, which also includes the Bureau of Justice Assistance; the Bureau of Justice Statistics; the National Institute of Justice; the Office for Victims of Crime; and the Office of Sex Offender Sentencing, Monitoring, Apprehending, Registering, and Tracking. Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE NCJ 243908 JULY 2014 Contents Could This Be Child Abuse? ..............................................................................................1 Caretaker Assessment ......................................................................................................2 Injury Assessment ............................................................................................................4 Ruling Out a Natural Phenomenon or Medical Conditions -

Nasolabial and Forehead Flap Reconstruction of Contiguous Alar
Journal of Plastic, Reconstructive & Aesthetic Surgery (2017) 70, 330e335 Nasolabial and forehead flap reconstruction of contiguous alareupper lip defects Jonathan A. Zelken a,b, Sashank K. Reddy c, Chun-Shin Chang a, Shiow-Shuh Chuang a, Cheng-Jen Chang a, Hung-Chang Chen a, Yen-Chang Hsiao a,* a Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital, College of Medicine, Chang Gung University, Taipei, Taiwan b Department of Plastic and Reconstructive Surgery, Breastlink Medical Group, Laguna Hills, CA, USA c Department of Plastic and Reconstructive Surgery, Johns Hopkins Hospital, Baltimore, MD, USA Received 4 May 2016; accepted 31 October 2016 KEYWORDS Summary Background: Defects of the nasal ala and upper lip aesthetic subunits can be Nasal reconstruction; challenging to reconstruct when they occur in isolation. When defects incorporate both Nasolabial flap; the subunits, the challenge is compounded as subunit boundaries also require reconstruc- Rhinoplasty; tion, and local soft tissue reservoirs alone may provide inadequate coverage. In such cases, Forehead flap we used nasolabial flaps for upper lip reconstructionandaforeheadflapforalarrecon- struction. Methods: Three men and three women aged 21e79 years (average, 55 years) were treated for defects of the nasal ala and upper lip that resulted from cancer (n Z 4) and trauma (n Z 2). Unaffected contralateral subunits dictated the flap design. The upper lip subunit was excised and replaced with a nasolabial flap. The flap, depending on the contralateral reference, determined accurate alar base position. A forehead flap resurfaced or replaced the nasal ala. Autologous cartilage was used in every case to fortify the forehead flap reconstruction. Results: Patients were followed for 25.6 months (range, 1e4 years). -

Part 1 the Thorax ECA1 7/18/06 6:30 PM Page 2 ECA1 7/18/06 6:30 PM Page 3
ECA1 7/18/06 6:30 PM Page 1 Part 1 The Thorax ECA1 7/18/06 6:30 PM Page 2 ECA1 7/18/06 6:30 PM Page 3 Surface anatomy and surface markings The experienced clinician spends much of his working life relating the surface anatomy of his patients to their deep structures (Fig. 1; see also Figs. 11 and 22). The following bony prominences can usually be palpated in the living subject (corresponding vertebral levels are given in brackets): •◊◊superior angle of the scapula (T2); •◊◊upper border of the manubrium sterni, the suprasternal notch (T2/3); •◊◊spine of the scapula (T3); •◊◊sternal angle (of Louis) — the transverse ridge at the manubrio-sternal junction (T4/5); •◊◊inferior angle of scapula (T8); •◊◊xiphisternal joint (T9); •◊◊lowest part of costal margin—10th rib (the subcostal line passes through L3). Note from Fig. 1 that the manubrium corresponds to the 3rd and 4th thoracic vertebrae and overlies the aortic arch, and that the sternum corre- sponds to the 5th to 8th vertebrae and neatly overlies the heart. Since the 1st and 12th ribs are difficult to feel, the ribs should be enu- merated from the 2nd costal cartilage, which articulates with the sternum at the angle of Louis. The spinous processes of all the thoracic vertebrae can be palpated in the midline posteriorly, but it should be remembered that the first spinous process that can be felt is that of C7 (the vertebra prominens). The position of the nipple varies considerably in the female, but in the male it usually lies in the 4th intercostal space about 4in (10cm) from the midline. -

The Alchemical Body in Daoism
The Alchemical Body in Daoism FABRIZIO PREGADIO Abstract This paper surveys some of the main features of the view of the human body in Daoist internal alchemy (neidan 內丹). The first sections discuss three different terms that refer to the body; cosmological, political, theological, natural, and al- chemical metaphors used to describe it; and the use of the body as a support for the system of correspondences that tie the human being to the cosmos. On this background, the development of internal alchemy closely relates to the earlier Daoist meditation practices on the inner gods. The figure of the Red Child (the innermost deity of the human being), in particular, bears close analogies to the “embryo” that alchemists generate through their practices. The final sections are concerned with the two main alchemical charts of the human body and with the use of the Buddhist concept of “dharma-body,” which some masters describe as the true immortal body. It is virtually impossible to distinguish the Daoist understanding of the body from its understanding of the human being, and this point consti- tutes on its own a central aspect of the Daoist way of seeing. For a Daoist, knowledge of the anatomic forms and the physiological workings of the body, or any of its parts and organs, is virtually irrelevant. The physical body performs another function: it serves to support different sets of metaphors that express the relation of the whole person to the Dao, the ultimate principle to which the person owes its existence. These metaphors may be cosmological (the body as a microcosm), political (the body as an administrative system), theological (the body as the residence of inner gods), natural (the body as a “landscape”), and alchemical (the body as a laboratory for compounding the elixir), to name the most important ones. -

Gross Anatomy
www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY www.BookOfLinks.com Notice Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The authors and the publisher of this work have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the authors nor the publisher nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they disclaim all responsibility for any errors or omissions or for the results obtained from use of the information contained in this work. Readers are encouraged to confirm the infor- mation contained herein with other sources. For example and in particular, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this work is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs. www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY David A. Morton, PhD Associate Professor Anatomy Director Department of Neurobiology and Anatomy University of Utah School of Medicine Salt Lake City, Utah K. Bo Foreman, PhD, PT Assistant Professor Anatomy Director University of Utah College of Health Salt Lake City, Utah Kurt H. -
Anatomical Snuffbox
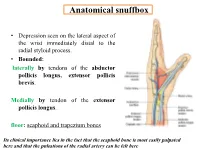
Anatomical snuffbox • Depression seen on the lateral aspect of the wrist immediately distal to the radial styloid process. • Bounded: laterally by tendons of the abductor pollicis longus, extensor pollicis brevis. Medially by tendon of the extensor pollicis longus. floor: scaphoid and trapezium bones Its clinical importance lies in the fact that the scaphoid bone is most easily palpated here and that the pulsations of the radial artery can be felt here Anatomical snuffbox Anatomical snuffbox • Contents: 2) Origin of the 1) The radial artery cephalic vein pass subcutaneously over the snuffbox. 3) Superficial branch of the radial nerve pass subcutaneously over the snuffbox. Blood supply of the hand Anastomoses occur between the radial and ulnar arteries via the superficial and deep palmar arches The Deep palmar arch is formed mainly by the radial artery while the superficial palmar arch is formed mainly by the ulnar artery 3-On entering the palm, it curves laterally behind (deep) the palmar 4-The arch is aponeurosis and in front completed on (superficial) of the long flexor the lateral side tendons forming by the the superficial palmar arch superficial branch of the radial artery. 2-Then it gives off its deep branch of which runs in front of the FR , and joins the radial artery to complete the deep palmar arch 1-Enters the hand anterior (superficial) to the Superficial flexor retinaculum palmar branch of radial artery through Guyon’s canal Radial artery 5-The superficial palmar arch gives off digital arteries from its convexity which pass to the fingers and supply them Superficial palmar arch Deep palmar branch of ulnar artery Superficial palmar branch of radial artery Ulnar artery Radial artery Radial Artery first dorsal interosseous muscle 1-From the floor of the anatomical snuff-box the radial artery leaves the dorsum of the hand by turning forward between the two heads of the first dorsal interosseous muscle. -

Traditional Chinese Medicine and Modern Medicine --- When East Meets West
TRADITIONAL CHINESE MEDICINE AND MODERN MEDICINE --- WHEN EAST MEETS WEST BY MK Sastry TRADITIONAL CHINESE MEDICINE (TCM) Simplified Chinese: 中医学 Traditional Chinese: 中醫學 Pin Yin: zhōng yī xué HISTORY OF TRADITIONAL CHINESE MEDICINE TCM MODERN MEDICINE Several Thousand Years Several Hundred Years Huang-di Nei-jing (Canon of Medicine): Suwen and Lingshu The earlist medical classic in China Compiled between 500 – 300 B.C. Summary of the medical experience and theoretical knowledge including yin-yang, the five elements, zang- fu, meridians (channels and collaterals), qi (vital energy) and blood, etiology, pathology, dignostic methods, differentiation of syndromes, As well as basic knowledge of acupuncture points and needling methods PRACTICES OF TRADITIONAL CHINESE MEDICINE MODERN MEDICINE Internal Medicine Surgery Immunotherapy Radiotherapy Chemotherapy 1. Chinese Herbal Medicine 中药 2. Acupuncture and Moxibustion 針灸 Cupping Gua Sha 刮痧 3. Chinese Massage – Tui Na 推拿 Die-da or Tieh Ta – 跌打 THE BASIC THEORIES OF TRADITIONAL CHINESE MEDICINE MODERN MEDICINE Anatomy Biology Physiology Biochemistry Immunology Microbiology Genetics Pathology Radiology 1. Yin-Yang Theory 2. The Five Elements 3. Zang-Fu Therory 4. Meridians (Channels and Collaterals) 5. Qi, Blood, and Body Fluid THE THEORIES OF YIN-YANG AND FIVE ELEMENTS The theories of yin-yang and the five elements were two kinds of outlook on nature in ancient China Chinese ancient physicians applied these two theories in traditional Chinese medicine, which have guided clinical practice up to -

Anatomical Variants in the Termination of the Cephalic Vein Stoyan Novakov1*, Elena Krasteva2
Institute of Experimental Morphology, Pathology and Anthropology with Museum Bulgarian Anatomical Society Acta morphologica et anthropologica, 25 (3-4) Sofia • 2018 Anatomical Variants in the Termination of the Cephalic Vein Stoyan Novakov1*, Elena Krasteva2 1 Department of Anatomy, Histology and Embryology, 2Department of Propaedeutics of Surgical Di- seases, Medical Faculty, Medical University of Plovdiv * Corresponding author e-mail: [email protected] Jugulocephalic vein is atavistic structure which is very rare. The low incidence of the variations of the cephalic vein in deltopectoral triangle and its position on the anterior surface of the clavicle and the neck doesn’t make it less important for the clinical practice. Phylo- and ontogenesis explain the formation of the above mentioned variations. We followed the pattern of the cephalic vein in its proximal part and termination to describe possible variations. In this long term study on 140 upper limbs of 70 cadavers, 4 or 2,9% of the cephalic veins were variable. The direct empting of the cephalic vein into internal jugular is an exception with few descriptions at the moment. The rareness of this anatomical variation doesn’t make it less important for clinical practice. It is described as a possible obstacle in catheter implantation, clavicle fractures and creation of arteriovenous fistula in patients on hemodialysis. Key words:cadavers, human anatomy variation, cephalic vein, external jugular vein, jugulocephalic vein Introduction Cephalic vein (CV) belongs to the group of superficial veins of the upper limb. It usually forms over the anatomical snuff-box on the radial side of the wrist from the radial end of the dorsal venous plexus. -

New Fixation Approach for Transverse Metacarpal Neck Fracture: a Biomechanical Study
Chiu et al. Journal of Orthopaedic Surgery and Research (2018) 13:183 https://doi.org/10.1186/s13018-018-0890-2 RESEARCHARTICLE Open Access New fixation approach for transverse metacarpal neck fracture: a biomechanical study Yung-Cheng Chiu1,2, Ming-Tzu Tsai3, Cheng-En Hsu4,5, Horng-Chaung Hsu1,2, Heng-Li Huang6,7 and Jui-Ting Hsu6,7* Abstract Background: Fifth metacarpal neck fracture, also known as boxer’s fracture, is the most common metacarpal fracture. Percutaneous Kirschner-wire (K-wire) pinning has been shown to produce favorable clinical results. However, the fixation power of K-wires is a major concern. Plate fixation is also a surgical option, but it has the disadvantages of tendon adhesion, requirement of secondary surgery for removal of the implant, and postoperative joint stiffness. A fixation method that causes little soft tissue damage and provides high biomechanical stability is required for patients with fifth metacarpal neck fracture for whom surgical intervention is indicated. The present study proposed fixation using K-wires and a cerclage wire to treat fifth metacarpal neck fracture. The fixation power of this new method was compared with that of K-wires alone and plates. Methods: We used a saw blade to create transverse metacarpal neck fractures in 16 artificial metacarpal bone specimens, which were then treated with four types of fixation as follows: (1) locking plate with five locking bicortical screws (LP group), (2) regular plate with five bicortical screws (RP group), (3) two K-wires (K group), and (4) two K-wires and a figure-of-eight cerclage wire (KW group). -

Signs to Help the Deaf Included in This Packet
Signs to help the Deaf Included in this packet: Medical Signs Color Signs People Signs This is made by: Deanna Zander, I am a parent of a deaf son. Here is my email address: [email protected], if you have any questions, please email your question, Please put in the Subject box- RE: Medical Signs. For more information, or to obtain a hospital kit for Deaf or Hard of Hearing, please contact Pam Smith, Adult Outreach Coordinator @ 701-665-4401 Medical Signs (Medicine) Medical Medicine- Tip of bent middle finger rubs circle on left palm Sign- Palm-out indexes circle Signs alternately Made By: Deanna Zander Hi, Hello, Howdy Good-Bye, Yes, Yep Bye Right “S” hand & head nods (both head & hand nod) No, Nope Flat hand, Touch forehead, Just wave First two fingers close onto move forward slightly right thumb, & shake your head Appointment Schedule Fingertips of the right palm- out “5” draws down left palm; then turn palm-in & draws across palm The right “S” hand palm down, is postitioned above the left “S” hand, also palm- down. The right hand circels above the left in a clockwise manner & is brought on the back of left hand. Your Name, My Name Birthday My, Mine- Your- The right middle finger touches the chin, Palm of flat Vertical flat palm moves then moves down to touch the chest hand on chest toward person Fingerspell- The right hand, palm- out, is move left to right, fingers wiggling up & Name- Right “H” touches left “H” at right angles MM/DD/YYYY down Call, phone Left “Y” hand, thumb near ear, little finger near mouth The upturned thumbs -

The Square Flap Technique for Burn Contractures: Clinical Experience and Analysis of Length Gain
Annals of Burns and Fire Disasters - vol. XXXI - n. 4 - December 2018 THE SQUARE FLAP TECHNIQUE FOR BURN CONTRACTURES: CLINICAL EXPERIENCE AND ANALYSIS OF LENGTH GAIN DOUBLE LAMBEAU RHOMBOÏDE POUR BRIDE SÉQUELLAIRE DE BRÛ- LURE: EXPÉRIENCE PRATIQUE ET ANALYSE DE LA LONGUEUR GAGNÉE Hifny M.A. Department of Plastic Surgery, Faculty of Medicine, Qena University Hospital, South Valley University, Egypt SUMMARY. Post-burn contractures, affecting the joints especially, are demanding problems. Many surgical techniques have been designated for burn contracture release. The aim of this study is to investigate the efficiency of the square flap technique to release a post-burn scar contracture, and assess the post-operative length gain that can be achieved by simple mathematical calculation. In this study, sixteen patients with linear contracture bands were treated with the square flap tech- nique. The anatomical distribution of the contractures was: axilla, cubital fossa, flank, perineum and popliteal fossa. Scar maturity ranged from 4 months - 9 years. Square flap width and contracture band length before and immediately after surgery were recorded by simple mathematical calculation. Flap complication was assessed. Patient satisfaction was also assessed during the follow-up period. All square flaps were effective in lengthening the contracture bands. The length of the contracture that was released ranged from 2 to 6 cm. The gain in length provided with this technique ranged from 212 to 350%, average 247%, and adequate contracture release was achieved in all cases postoperatively. All square flaps healed uneventfully except for one (6%), which demonstrated limited epidermolysis that healed by secondary intention. The fol- low-up interval ranged from 6 months to 1.5 years.