Fight Club Pittsburgh Mma Michael Morrow
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Paul Vunaks 45 Combat Secrets
Paul Vunaks 45 Combat Secrets Revised June 2020 Chapter 1: Stress Inoculation Chapter 2: Stress Inoculation Standing-Up Chapter 3: The Accordion Drill – “The bread and butter backbone of all of our drills.” Chapter 4: Takedown Defense Chapter 5: My Favorite Takedown Chapter 6: Bruce Lee’s Straight Blast Chapter 7: Bruce Lee’s Pendulum Chapter 8: The secret to intercepting ! Chapter 9: The Art of Defanging (the only weapons technique you will ever need) Chapter 10: Isometrics the Secret to the Guard Chapter 11: Bruce Lee's One Inch Punch Chapter 12: Super Coordination ! Chapter 13: The Secret to De-Fanging The Snake Chapter 14: The Mother of All Drills Chapter 15: The "U-Drill" our most empowering drill Chapter 16: How To Double Your speed ! Chapter 17: The Flagship of Kettlebells Chapter 18: What Makes Us Different? Chapter 19: The Power of the Fork Chapter 20: The double progressive indirect attack (the greatest fake in the world) Chapter 21: Locking the Art of Joint Reversals Chapter 22: Footwork Chapter 23: The nutcracker (the best drill in the world against the street ground and pound) Chapter 24: The Missile, Boxing's Greatest Move Chapter 25: Contemporary JKD"s Progression Chapter 26: Flawless Body Mechanics Chapter 27: The Secret to Keeping Students Chapter 28: Quieting the Mind: Physical Meditation with Ancient Indian Exercises Chapter 29: The Great Eight Chapter 30: The First Minute of the Fight Chapter 31: The rst minute of the ght part 2 Chapter 32: A successful school Chapter 33: The Three Most Common Asked Scenarios Chapter 34: Sizzle Sells Chapter 35: The Best Curriculum Chapter 36: Rickson's Jiu Jitsu Chapter 37: The Prolic Primordial Rear Naked Choke Chapter 38: The Neck Crank Chapter 39: "Handicap" Training for the Ground Chapter 40: How to perform a proper Mount (Brazilian Jiu-Jitsu that is !) Chapter 41: Footlocks Chapter 42: The Deadly Dungeonous Defense against the Prolic Primordial Rear Naked Choke ! Chapter 43: The Curriculum Chapter 44: The Emotional Dimension Part 1 Chapter 45: Differentiating Emotions Vunak's Top Combat Secrets Ch. -
BISPING: Barnett Needs to Push the Pace Vs. Nelson
FS1 UFC TONIGHT Show Quotes – 9/23/15 BISPING: Barnett Needs To Push The Pace Vs. Nelson Florian: “Uriah Hall Is Too Dangerous To Just Stand and Trade With” LOS ANGELES – UFC TONIGHT host Kenny Florian and guest host Michael Bisping break down the upcoming FS1 UFC FIGHT NIGHT: BARNETT VS. NELSON. Karyn Bryant and Ariel Helwani add reports. UFC TONIGHT guest host Michael Bisping on how Josh Barnett can beat Roy Nelson: “Josh needs to not get hit by the right hand of Roy. He needs to push the pace of the fight, move forward, and push Roy up against fence and brutalize him with knees and elbows like he did with Frank Mir. Most of his finishes came from the clinch position. He finishes fights against the fence. He did that against Frank Mir.” UFC TONIGHT host Kenny Florian on Barnett avoiding Nelson’s knock out power: “Josh doesn’t want to be on the outside where Roy’s right hand can get him. He wants to be on the inside. He’s been busy on the submission circuit. He’s dangerous on the mat and that’s where he wants to get Roy.” Bisping on how Nelson should fight Barnett: “What Roy can’t get is predictable. If he just tries to throw the big right hand, Barnett is going to see it coming. Roy has to mix up his striking. I’m not sure he’s going to go for takedowns. But he has to mix his striking. His right hand and left hooks, to keep Josh at bay.” Florian on Nelson mixing up his strikes: “The knock on Nelson is his lack of evolution. -

U.S. and Iraqi Soldiers Aid Bedouin Camp Near Karbala by Pfc
Click here to subscribe September 1, 2009 U.S. and Iraqi Soldiers aid Bedouin camp near Karbala By Pfc. Bethany L. Little Bedouins are nomadic shepherds who choose to live in 172nd Inf. Bde. the desert and are able to sustain themselves by bartering KARBALA - Soldiersldiers ooff 1st Platoon, Bravo Batt ery, 1st their livestock and things they produce. Batt alion, 77th Fieldld ArtilleryA ill helped Soldiers of the 33rd There are three Bedouin camps in the area surrounding Iraqi Army Brigade hand out 20 boxes fi lled with toys, Karbala constantly changing locations in search of the best clothes, shoes, coloring books and crayons to a Bedouin conditions for their livestock. camp just outside of Karbala recently. “We only visited one of the camps today, because we knew the exact location,” said Staff Sgt. Joseph W. Rippey, squad leader, 1st plt., Bravo Btry., 1st Bn., 77th FA Regt.. “This is our second time here; last time there were approx- imately 12 tents, but now there are only three tents and one permanent dwelling.” The clothing, shoes and toys were a combined dona- tion from the 172nd Infantry Brigade Public Aff airs Of- fi ce, Tactical Psychological Operations Detachment 303-1, Thompson Toyota car dealership and Sherah Oberman from Doylestown, Pa. The Bedouin children cheered and shrieked with excite- ment as Soldiers passed out the donated items. “We are very grateful,” said Ali Shallal, a young camp resident. “These are all things that everyone here can use, especially the clothes and shoes for the smaller children.” Bedouin camps are spread throughout the Middle East. -

Adjustment Description Alterations to V-Shift's
Adjustment Description Abilities granting invincibility or armor from the 1st frame, as well as low- risk or high-return moves invincible to throws have all been adjusted to have less effective throw invincibility. Alterations to V-Shift's Considering V-Shift's offensive and defensive capabilities, normal throws offensive/defensive should have enough impact to reliably handle V-Shifts, but characters with capabilities the invincible abilities mentioned above had an easy way to deal with throws and strikes. This gave their defense such a strong advantage that offensive opponents struggled against it. These adjustments seek to correct this issue. These general adjustments are a continuation of previous adjustments. Improvements to While V-Skills and V-Triggers have already been adjusted overall, players infrequently used V-Triggers tend to use one V-Skill and V-Trigger over the other, so we have further and V-Skills strengthened the techniques themselves and the moves that rely on their input. Some characters have been rebalanced in light of previous adjustments. We have buffed characters who were lacking in strength or who were Rebalancing of some largely left alone in previous adjustments. characters Characters with downward adjustments have not had their moves altered significantly; rather, the risks and returns of moves have been properly balanced. Balance Change Overview We've adjusted Nash's close-quarters attack, standing light kick, to yield more of an advantage on hit, and we have further improved Nash's impressive mid to long-distance combat. Standing light kick was previously adjusted to have faster start-up and to be easier to land, but we noticed that it didn't grant the same rewards as it did for other characters. -

1St May, 2017, 11:50 AM
CQB KAJUKENBO CLUB Combatives, Personal Protection & Defensive Tactics FAQhttp://www.cqbkajukenbo.com Last Modified: 1st May, 2017, 11:50 AM “Only a warrior chooses pacifism; others are condemned to it.” — Unknown “We make war that we may live in peace.” — Aristotle “Civilize the mind but make savage the body.” — Chairman Mao Q: “WHAT IS KAJUKENBO?” Kajukenbo is a hybrid martial art that combines multiple martial arts including (but not limited to) western boxing, judo, jujutsu, kenpo karate, tang soo do, and kung fu. Kajukenbo is considered by many experts to be America’s first ‘Mixed Martial Art‘ — commonly known as ‘MMA‘. It was founded around 1947 in Oahu, Hawaii and the first classes were taught in the Palama Settlement Gym. The original purpose of the art was to deal with local crime, and to help the people defend themselves against U.S. Navy sailors from Pearl Harbor who would start fights with the locals. The creators are recognized as being Sijo (“founder”) Adriano Emperado, Peter Young Yil Choo, Joe Holck, Frank Ordonez, and George Chang, who were later called the ‘Black Belt Society’. The founders of Kajukenbo wanted to develop an art that would be readily useful on the street. As they trained and fought in and around Palama Settlement, the founders of Kajukenbo quickly gained reputations as formidable street-fighters. While similar to -and compatible with- Jeet Kune Do, Kajukenbo predates JKD by about 20 years. Kajukenbo uses hard, fast strikes to soft targets and vital points throughout the body, takedowns involving high impact throws and many joint and limb destruction techniques — usually as follow-ups to takedowns or grappling. -
2015 Topps UFC Chronicles Checklist
BASE FIGHTER CARDS 1 Royce Gracie 2 Gracie vs Jimmerson 3 Dan Severn 4 Royce Gracie 5 Don Frye 6 Vitor Belfort 7 Dan Henderson 8 Matt Hughes 9 Andrei Arlovski 10 Jens Pulver 11 BJ Penn 12 Robbie Lawler 13 Rich Franklin 14 Nick Diaz 15 Georges St-Pierre 16 Patrick Côté 17 The Ultimate Fighter 1 18 Forrest Griffin 19 Forrest Griffin 20 Stephan Bonnar 21 Rich Franklin 22 Diego Sanchez 23 Hughes vs Trigg II 24 Nate Marquardt 25 Thiago Alves 26 Chael Sonnen 27 Keith Jardine 28 Rashad Evans 29 Rashad Evans 30 Joe Stevenson 31 Ludwig vs Goulet 32 Michael Bisping 33 Michael Bisping 34 Arianny Celeste 35 Anderson Silva 36 Martin Kampmann 37 Joe Lauzon 38 Clay Guida 39 Thales Leites 40 Mirko Cro Cop 41 Rampage Jackson 42 Frankie Edgar 43 Lyoto Machida 44 Roan Carneiro 45 St-Pierre vs Serra 46 Fabricio Werdum 47 Dennis Siver 48 Anthony Johnson 49 Cole Miller 50 Nate Diaz 51 Gray Maynard 52 Nate Diaz 53 Gray Maynard 54 Minotauro Nogueira 55 Rampage vs Henderson 56 Maurício Shogun Rua 57 Demian Maia 58 Bisping vs Evans 59 Ben Saunders 60 Soa Palelei 61 Tim Boetsch 62 Silva vs Henderson 63 Cain Velasquez 64 Shane Carwin 65 Matt Brown 66 CB Dollaway 67 Amir Sadollah 68 CB Dollaway 69 Dan Miller 70 Fitch vs Larson 71 Jim Miller 72 Baron vs Miller 73 Junior Dos Santos 74 Rafael dos Anjos 75 Ryan Bader 76 Tom Lawlor 77 Efrain Escudero 78 Ryan Bader 79 Mark Muñoz 80 Carlos Condit 81 Brian Stann 82 TJ Grant 83 Ross Pearson 84 Ross Pearson 85 Johny Hendricks 86 Todd Duffee 87 Jake Ellenberger 88 John Howard 89 Nik Lentz 90 Ben Rothwell 91 Alexander Gustafsson -

25 Pro Fighters, Managers, and Coaches Reveal Their Best Tips to Land a Sponsorship by Solmadrid Vazquez Follow Me on Twitter Here
25 Pro Fighters, Managers, and Coaches Reveal Their Best Tips to Land a Sponsorship by Solmadrid Vazquez Follow me on Twitter here. Sponsorships can make or break you. The problem is, the process of landing a sponsorship is counter-intuitive. Being a great fighter is NOT enough. I’m sure you’ve seen fighters who land sponsors left and right. What’s their secret? How come they can get 27 sponsors in one day and you can’t even get one freakin’ rep to look at you? What THE hell is going on?! To get to this bottom of this conundrum, I contacted some of the best fighters, managers, and trainers in the game and asked them a simple question: “What is your #1 tip to land a sponsorship?” Each tip has a custom tweet link after it so feel free to share your favorite tips with your followers. Let’s Get Ready To Ruuuummmmbllllllleee!!! Frank Shamrock Frank Shamrock is a retired MMA Fighter. He was the first UFC Middleweight Champion and retired as the four-time defending undefeated champion. He was also the first WEC Light Heavyweight Champion, and the first Strikeforce Middleweight Champion. He was a brand spokesman for Strikeforce and is a Sports Commentator for Showtime. Frank can be found at his site, on Facebook, and on Twitter. My number one tip to landing a sponsorship is presenting yourself properly. Present a long-term consistent growth plan that somebody, or a sponsor, could attach themselves to, so you can show how you will grow together. “Present a long-term consistent growth plan.” Tweet this. -

Legalization of Cage Fighting in New York Dear State Assembly Member
January 10, 2012 Re: Legalization of cage fighting in New York Dear State Assembly Member: We are writing you to raise concerns about renewed efforts by Zuffa LLC, the parent company of the Ultimate Fighting Championship (UFC), to legalize cage fighting in the State of New York. You are no doubt aware that the State of New York banned cage fighting in 1997. We urge you to continue to uphold the ban on cage fighting, given that the UFC, the largest promoter of cage fighting events in the U.S., has failed to demonstrate that it is willing to ensure its fighters behave in a socially responsible way, even as the company expressly markets its fights and fighters to children. We believe that the UFC contributes to a culture of violence against women, and lesbian, gay, bisexual and transgender (LGBT) people. Children, in particular, should not be exposed to the homophobic, misogynistic and violent language that has been permitted by the UFC. Please see the following website, UFC = Unfit For Children (www.UnfitForChildren.org), for more information. Some examples of anti-gay and anti-women statements by people associated with the UFC include the following: In videos, UFC light heavyweight Quinton “Rampage” Jackson repeatedly urged Japanese fans to repeat an anti-gay slur.1 The fans, who do not appear to understand English, repeated the anti-gay slur at Jackson’s urging. In one video, Jackson instructed a Japanese man to say, “Goodbye, I want you to piss on my face.”2 Recently, a UFC fighter taunted his opponent by threatening to act like former Penn State assistant football coach Jerry Sandusky, who has been charged with 52 counts of molesting boys. -

Featuring Advice from UFC Hall of Famers Randy Couture, Ken Shamrock, Bas Rutten, Pat Miletich, Dan Severn and More! Online
narm4 (Ebook pdf) The Ultimate Guide to Preventing and Treating MMA Injuries: Featuring advice from UFC Hall of Famers Randy Couture, Ken Shamrock, Bas Rutten, Pat Miletich, Dan Severn and more! Online [narm4.ebook] The Ultimate Guide to Preventing and Treating MMA Injuries: Featuring advice from UFC Hall of Famers Randy Couture, Ken Shamrock, Bas Rutten, Pat Miletich, Dan Severn and more! Pdf Free Dr. Jonathan Gelber M.D. M.S. ePub | *DOC | audiobook | ebooks | Download PDF Download Now Free Download Here Download eBook #1405868 in Books Gelber M D M S Jonathan 2016-05-10Original language:EnglishPDF # 1 8.90 x .40 x 6.00l, .0 #File Name: 1770411720200 pagesThe Ultimate Guide to Preventing and Treating MMA Injuries Featuring advice from UFC Hall of Famers Randy Couture Ken Shamrock Bas Rutten Pat Miletich Dan Severn and more | File size: 76.Mb Dr. Jonathan Gelber M.D. M.S. : The Ultimate Guide to Preventing and Treating MMA Injuries: Featuring advice from UFC Hall of Famers Randy Couture, Ken Shamrock, Bas Rutten, Pat Miletich, Dan Severn and more! before purchasing it in order to gage whether or not it would be worth my time, and all praised The Ultimate Guide to Preventing and Treating MMA Injuries: Featuring advice from UFC Hall of Famers Randy Couture, Ken Shamrock, Bas Rutten, Pat Miletich, Dan Severn and more!: 2 of 2 people found the following review helpful. This is truly a great read if you are interested in Preventing and Treating ...By MikeSiljanoskiI purchased this book about 3 weeks ago and plan on sharing it with several friends that train for MMA. -
2021 UFC Select Checklist
2021 Select UFC Checklist - By Fighter Fighter Set Card # Team Print Run Al Iaquinta Auto - Octagon Action Sigs + Parallels 24 Lightweight 185 Aleksandar Rakic Base - Concourse 6 Light Heavyweight Aleksandar Rakic Base - Octagonside 226 Light Heavyweight Aleksandar Rakic Base - Premier Level 153 Light Heavyweight Alexander Gustafsson Auto - Octagon Action Sigs + Parallels 25 Heavyweight 285 Alexander Gustafsson Insert - Global Icons 23 Heavyweight Alexander Volkanovski Auto - Signatures + Parallels 40 Featherweight 135 Alexander Volkanovski Base - Concourse 16 Featherweight Alexander Volkanovski Base - Octagonside 246 Featherweight Alexander Volkanovski Base - Premier Level 155 Featherweight Alexander Volkanovski Insert - Global Icons 9 Featherweight Alexander Volkanovski Insert - Phenomenon 21 Featherweight Alexander Volkov Base - Concourse 26 Heavyweight Alexander Volkov Base - Octagonside 266 Heavyweight Alexander Volkov Base - Premier Level 157 Heavyweight Aljamain Sterling Base - Concourse 46 Bantamweight Aljamain Sterling Base - Octagonside 206 Bantamweight Aljamain Sterling Base - Premier Level 151 Bantamweight Aljamain Sterling Insert - Select Grapplers 15 Bantamweight Amanda Nunes Insert - Select Strikers 13 Women's Bantamweight Amanda Nunes Auto - Signatures + Parallels 16 Women's Featherweight 135 Amanda Nunes Base - Concourse 56 Women's Featherweight Amanda Nunes Base - Octagonside 216 Women's Featherweight Amanda Nunes Base - Premier Level 152 Women's Featherweight Amanda Nunes Insert - Global Icons 17 Women's Featherweight -
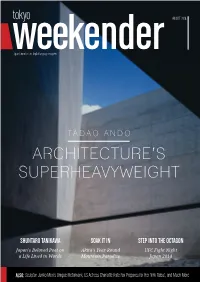
Tadao Ando Architecture’S Superheavyweight
AUGUST 2014 Japan’s number one English language magazine TADAO ANDO ARCHITECTURE’S SUPERHEAVYWEIGHT SHUNTARO TANIKAWA SOAK IT IN STEP INTO THE OCTAGON Japan’s Beloved Poet on Akita’s Year-Round UFC Fight Night a Life Lived in Words Mountain Paradise Japan 2014 ALSO: Sculptor Junko Mori’s Unique Metalwork, US Actress Charlotte Kate Fox Prepares for Her NHK Debut, and Much More AUGUST 2014 www.tokyoweekender.com AUGUST 2014 CONTENTS 8 AKITA ONSENS Dipping into the hospitality of Nyuto Mountain’s hot spring ryokan 16 18 22 TADAO ANDO JUNKO MORI CHARLOTTE KATE FOX One of the world’s most celebrated Transmuting metal into organic forms of Say hello to the face of NHK’s upcoming architects reveals his passion for the craft subtle grace and beauty morning drama, Massan 6 UFC Preview 20 Is Japan Expensive? 31 Weekender Insiders Club We take a look ahead at three of the top Ken Seeroi dispels one of the country’s Join in, sign on, and find out about matchups at Fight Night Japan 2014 biggest myths product launches and special offers 7 Takanori Gomi 24 People, Parties, Places 32 Agenda The Fireball Kid prepares for his battle The latest updates from Tokyo’s nonstop Celebrate the closing of summer any way with Myles “Fury“ Jury social scene you like it, from udon to samba 13 Shuntaro Tanikawa 30 Movies 34 Back in the Day Looking back at more than six decades of Scarlett Johansson updates her grey In which a shady character from the life as a public poet matter and Lupin goes live action Weekender’s past ‘fesses up www.tokyoweekender.com AUGUST 2014 THIS MONTH IN THE WEEKENDER clean, minimal lines of his monumental AUGUST 2014 designs, the Osaka-born architect has a AUGUST 2014 fascinating background that includes a Japan’s number one English language magazine stint in the boxing ring and no formal schooling whatsoever. -

Trident Academy of Martial Arts Presents
Trident Martial Arts Is Proud To Present: FOR A SPECIAL EVENT: 04/25/2015 & 04/26/2015 11a.m. to 2 p.m. Since 1974, Erik Paulson has trained in many disciplines including Freestyle and Greco-Roman Wrestling, TKD, Boxing, Jeet Kune Do, Filipino Kali/Eskrima, Sambo (martial art), Catch Wrestling and Brazilian Jiu-Jitsu, studying first with Rorion Gracie, Royce Gracie, Rickson Gracie in 1989. He has studied with 40 different teachers over his 30 years of training including Rick Faye, Greg Nelson, Yorinaga Nakamura, Larry Hartsell, Tim Tackett, Ajarn Chai Sirisute, Nic Saignac, Rigan Machado, Rico Chipparelli, and the legendary Dan Inosanto, who claims Erik is one of the world's most dynamic grapplers. He currently runs the CSW Training Center in Fullerton, California where he trains MMA fighters such as Josh Barnett, Ken Shamrock, Renato Sobral, Cub Swanson, Ben Jones and Ginelle Marquez. He is closely affiliated with Sean Sherk and Brock Lesnar of the Minnesota Martial Arts Academy. Erik holds the rank of Black Belt in Brazilian Jiu-Jitsu from Rigan Machado. He also trained extensively with Rorion, Royce, and Rickson Gracie. Erik is the founder of Combat Submission Wrestling, and STX Kickboxing. Whether you want to increase and improve your knowledge base and skills, or you’re preparing for competition, you won’t want to miss this opportunity to train with the legendary Erik Paulson. Seminar is open to all ages. All participants (or parent, if under age 18) must sign a Release From Liability. No videotaping without permission. LOCATION: TRIDENT MARTIAL ARTS, 3310 Noble Pond Way #104, Woodbridge, VA 22193 REGISTER/CONTACT: 703-490-2425 or [email protected] Advance Registration (by 04/18/14): 1 Day $ 95 2 Days $180 At the Door: 1 Day $110 2 Days $210 ADDITIONAL $5 FOR PAYPAL TRANSACTIONS MC/VI/DS/AX ACCEPTED VIA TELEPHONE .