Pakistan National Emergency Action Plan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cast and Baradri System and Voting Behavior in Pakistan (Elections 2018): a Case Study of Hafizabad District
Cast and Baradri System and Voting Behavior in Pakistan (Elections 2018): A Case Study of Hafizabad District Karim Haider Muhammad Arshad Ali This study scrutinizes the impact of caste and Baradri system on voting behavior evolving from Pakistan’s general elections of 2018. Traditionally, the caste and Baradari system have been playing a substantial role in the elections of Pakistan since its birth especially in the region of Punjab. After the partition the evolution and modernization of electoral system and introduction of democratic institution in Pakistan never fully changed the customary value-system of the society of Punjab which is largely based on caste and Baradari system. With specific reference to caste and Baradari system in Punjab, an analytical research has been made to understand profound origins of Caste and Baradari System and its impact on the voting behavior of four selected constituencies, one of National Assembly and three of Provincial Assembly of Punjab in one of the districts of province of Punjab in general elections of 2018. Further, this study explains that the Punjab is based on social divergence with national political culture; therefore, the people of Punjab always look standing with the authoritarian rule which begins from family system and ends at national politics of Pakistan. Having majority seats in National Assembly the role of Punjab is very important and study about the voting behavior of the people of Punjab has special reference to national politics. Introduction Baradari defined as “brotherhood” initiated by the Persian language word Baradar meaning “brother”. Muslims of south Asian region especially in India and Pakistan, a large number of socialclasses are separated on the origin of Biradaris. -

Crisis Response Bulletin Page 1-16
IDP IDP IDP CRISIS RESPONSE BULLETIN April 06, 2015 - Volume: 1, Issue: 12 IN THIS BULLETIN HIGHLIGHTS: English News 3-29 Punjab to help Sindh computerise land record 03 Three more killed as heavy rain, Hailstones continue to Hit Sindh 03 48,076 Rescued by 1122 in One Month 05 Natural Calamities Section 3-8 NDMA issues flood warning for areas in Punjab 06 Safety and Security Section 9-14 Curbing terrorism:Counter-terror stations to start probes in two weeks 09 Police gear up for Easter Day protection against terrorism 09 Public Services Section 15-29 No country for old Afghans: ‘Post-1951 immigrants to be considered 10 illegal’ Maps 30-36 WB extends financial help of $75m to Fata TDPs 11 Free the streets: SHC orders law enforcers to continue action against 11 barriers Urdu News 50-37 AJK to expel 11,000 Afghans; bans 63 outfits in the region 12 IDPs’ return to North Waziristan begins 13 Natural Calamities Section 50-48 Ranking of Pakistan in education 15 Scheduled and unscheduled load shedding increases in Lahore 17 Safety and Security section 47-43 Power shortfall decreases to 3,400MW 18 Public Service Section 42-37 New cybercrime bill tough on individuals’ rights, soft on crime 19 PAKISTAN WEATHER MAP WIND SPEED MAP OF PAKISTAN TEMPERATURE MAP OF PAKISTAN PUNJAB - FIRE INCIDENTS MAP MAPS CNG SECTOR GAS LOAD MANAGEMENT PLAN-SINDH VEGETATION ANALYSIS MAP OF PAKISTAN REGISTERED AND UNREGISTERED MADRASA IN SINDH 70°0'0"E REGISTERED AND UNREGISTERED MADRASA IN SINDH Legend Number of Registered & KARACHI: Twenty per cent of the seminaries functioning Unregistered Madrasa across the province are situated in Karachi west district alone, it emerged on Friday as the home department Registered carried out an exercise aimed at establishing a database 35 Kashmore of madressahs and streamlining their registration Balochistan 54 Punjab process. -

SEF Assisted Schools (SAS)
Sindh Education Foundation, Govt. of Sindh SEF Assisted Schools (SAS) PRIMARY SCHOOLS (659) S. No. School Code Village Union Council Taluka District Operator Contact No. 1 NEWSAS204 Umer Chang 3 Badin Badin SHUMAILA ANJUM MEMON 0333-7349268 2 NEWSAS179 Sharif Abad Thari Matli Badin HAPE DEVELOPMENT & WELFARE ASSOCIATION 0300-2632131 3 NEWSAS178 Yasir Abad Thari Matli Badin HAPE DEVELOPMENT & WELFARE ASSOCIATION 0300-2632131 4 NEWSAS205 Haji Ramzan Khokhar UC-I MATLI Matli Badin ZEESHAN ABBASI 0300-3001894 5 NEWSAS177 Khan Wah Rajo Khanani Talhar Badin HAPE DEVELOPMENT & WELFARE ASSOCIATION 0300-2632131 6 NEWSAS206 Saboo Thebo SAEED PUR Talhar Badin ZEESHAN ABBASI 0300-3001894 7 NEWSAS175 Ahmedani Goth Khalifa Qasim Tando Bago Badin GREEN CRESCENT TRUST (GCT) 0304-2229329 8 NEWSAS176 Shadi Large Khoski Tando Bago Badin GREEN CRESCENT TRUST (GCT) 0304-2229329 9 NEWSAS349 Wapda Colony JOHI Johi Dadu KIFAYAT HUSSAIN JAMALI 0306-8590931 10 NEWSAS350 Mureed Dero Pat Gul Mohammad Johi Dadu Manzoor Ali Laghari 0334-2203478 11 NEWSAS215 Mureed Dero Mastoi Pat Gul Muhammad Johi Dadu TRANSFORMATION AND REFLECTION FOR RURAL DEVELOPMENT (TRD) 0334-0455333 12 NEWSAS212 Nabu Birahmani Pat Gul Muhammad Johi Dadu TRANSFORMATION & REFLECTION FOR RURAL DEVELOPMENT (TRD) 0334-0455333 13 NEWSAS216 Phullu Qambrani Pat Gul Muhammad Johi Dadu TRANSFORMATION AND REFLECTION FOR RURAL DEVELOPMENT (TRD) 0334-0455333 14 NEWSAS214 Shah Dan Pat Gul Muhammad Johi Dadu TRANSFORMATION AND REFLECTION FOR RURAL DEVELOPMENT (TRD) 0334-0455333 15 RBCS002 MOHAMMAD HASSAN RODNANI -

Cyclone Contigency Plan for Karachi City 2008
Cyclone Contingency Plan for Karachi City 2008 National Disaster Management Authority Government of Pakistan July 2008 ii Contents Acronyms………………………………………………………………………………………………………………..iii Executive Summary…………………………………………………………………………………………………....iv General…………………………………………………………………………………………………………………..1 Aim………………………………………………………………………………………………………………………..2 Scope…………………………………………………………………………………………………………………….2 Tropical Cyclone………………………………………………………………………………………..……………….2 Case Studies Major Cyclones………………………..……………………………………… ……………………….3 Historical Perspective – Cyclone Occurrences in Pakistan…...……………………………………….................6 General Information - Karachi ….………………………………………………………………………………….…7 Existing Disaster Response Structure – Karachi………………………. ……………………….…………….……8 Scenarios for Tropical Cyclone Impact in Karachi City ……………………………………………………….…..11 Scenario 1 ……………………………………………………………………………………………….…..11 Scenario 2. ……………………………………………………………………………………………….….13 Response Scenario -1…………………… ……………………………………………………………………….…..14 Planning Assumptions……………………………………………………………………………………....14 Outline Plan……………………………………………………………………………………………….….15 Pre-response Phase…………………………………………………………………………………….… 16 Mid Term Measures……………………………………………………………………..………..16 Long Term Measures…………………...…………………….…………………………..……...20 Response Phase………… ………………………..………………………………………………..………21 Provision of Early Warning……………………. ......……………………………………..……21 Execution……………………….………………………………..………………..……………....22 Health Response……………….. ……………………………………………..………………..24 Coordination Aspects…………………………………………….………………………...………………25 -

Malir-Karachi
Malir-Karachi 475 476 477 478 479 480 Travelling Stationary Inclass Co- Library Allowance (School Sub Total Furniture S.No District Teshil Union Council School ID School Name Level Gender Material and Curricular Sport Total Budget Laboratory (School Specific (80% Other) 20% supplies Activities Specific Budget) 1 Malir Karachi Gadap Town NA 408180381 GBLSS - HUSSAIN BLAOUCH Middle Boys 14,324 2,865 8,594 5,729 2,865 11,459 45,836 11,459 57,295 2 Malir Karachi Gadap Town NA 408180436 GBELS - HAJI IBRAHIM BALOUCH Elementary Mixed 24,559 4,912 19,647 4,912 4,912 19,647 78,588 19,647 98,236 3 Malir Karachi Gadap Town 1-Murad Memon Goth (Malir) 408180426 GBELS - HASHIM KHASKHELI Elementary Boys 42,250 8,450 33,800 8,450 8,450 33,800 135,202 33,800 169,002 4 Malir Karachi Gadap Town 1-Murad Memon Goth (Malir) 408180434 GBELS - MURAD MEMON NO.3 OLD Elementary Mixed 35,865 7,173 28,692 7,173 7,173 28,692 114,769 28,692 143,461 5 Malir Karachi Gadap Town 1-Murad Memon Goth (Malir) 408180435 GBELS - MURAD MEMON NO.3 NEW Elementary Mixed 24,882 4,976 19,906 4,976 4,976 19,906 79,622 19,906 99,528 6 Malir Karachi Gadap Town 2-Darsano Channo 408180073 GBELS - AL-HAJ DUR MUHAMMAD BALOCH Elementary Boys 36,374 7,275 21,824 14,550 7,275 29,099 116,397 29,099 145,496 7 Malir Karachi Gadap Town 2-Darsano Channo 408180428 GBELS - MURAD MEMON NO.1 Elementary Mixed 33,116 6,623 26,493 6,623 6,623 26,493 105,971 26,493 132,464 8 Malir Karachi Gadap Town 3-Gujhro 408180441 GBELS - SIRAHMED VILLAGE Elementary Mixed 38,725 7,745 30,980 7,745 7,745 30,980 123,919 -

12086393 01.Pdf
Exchange Rate 1 Pakistan Rupee (Rs.) = 0.871 Japanese Yen (Yen) 1 Yen = 1.148 Rs. 1 US dollar (US$) = 77.82 Yen 1 US$ = 89.34 Rs. Table of Contents Chapter 1 Introduction ...................................................................................................................... 1-1 1.1 Karachi Transportation Improvement Project ................................................................................... 1-1 1.1.1 Background................................................................................................................................ 1-1 1.1.2 Work Items ................................................................................................................................ 1-2 1.1.3 Work Schedule ........................................................................................................................... 1-3 1.2 Progress of the Household Interview Survey (HIS) .......................................................................... 1-5 1.3 Seminar & Workshop ........................................................................................................................ 1-5 1.4 Supplementary Survey ....................................................................................................................... 1-6 1.4.1 Topographic and Utility Survey................................................................................................. 1-6 1.4.2 Water Quality Survey ............................................................................................................... -

East-Karachi
East-Karachi 475 476 477 478 479 480 Travelling Stationary Inclass Co- Library Allowance (School Sub Total Furniture S.No District Teshil Union Council School ID School Name Level Gender Material and Curricular Sport Total Budget Laboratory (School Specific (80% Other) 20% supplies Activities Specific Budget) 1 East Karachi Jamshed Town 1-Akhtar Colony 408070173 GBLSS - H.M.A. Middle Mixed 7,841 1,568 4,705 3,137 1,568 6,273 25,093 6,273 31,366 2 East Karachi Jamshed Town 2-Manzoor Colony 408070139 GBPS - BILAL MASJID NO.2 Primary Mixed 12,559 2,512 10,047 2,512 2,512 10,047 40,189 10,047 50,236 3 East Karachi Jamshed Town 2-Manzoor Colony 408070174 GBLSS - UNION Middle Mixed 16,613 3,323 13,290 3,323 3,323 13,290 53,161 13,290 66,451 4 East Karachi Jamshed Town 9-Central Jacob Line 408070171 GBLSS - BATOOL GOVT` BOYS`L/SEC SCHOOL Middle Mixed 12,646 2,529 10,117 2,529 2,529 10,117 40,466 10,117 50,583 5 East Karachi Jamshed Town 10-Jamshed Quarters 408070160 GBLSS - AZMAT-I-ISLAM Middle Boys 22,422 4,484 17,937 4,484 4,484 17,937 71,749 17,937 89,687 6 East Karachi Jamshed Town 10-Jamshed Quarters 408070162 GBLSS - RANA ACADEMY Middle Boys 13,431 2,686 8,059 5,372 2,686 10,745 42,980 10,745 53,724 7 East Karachi Jamshed Town 10-Jamshed Quarters 408070163 GBLSS - MAHMOODABAD Middle Boys 20,574 4,115 12,344 8,230 4,115 16,459 65,836 16,459 82,295 8 East Karachi Jamshed Town 11-Garden East 408070172 GBLSS - GULSHAN E FATIMA Middle Mixed 16,665 3,333 13,332 3,333 3,333 13,332 53,327 13,332 66,658 9 East Karachi Gulshan-e-Iqbal Town 3-PIB -

Pakistan the Factsheet July2013
July 2013 Factsheet PAKISTAN July 2013 Pakistan: A History of Violence THE U.S. COMMISSION ON INTERNATIONAL RELIGIOUS FREEDOM was created by the International Religious Freedom Act of 1998 to monitor the status of freedom of thought, conscience, and religion or belief abroad, as defined in the Universal Declaration of Human Rights and related international instruments, and to give independent policy recommendations to the President, The Pakistan Religious Violence Project, an undertaking of the U.S. Com- Secretary of State, mission on International Religious Freedom, tracked over the past 18 and Congress. months publicly-reported attacks against religious communities in Paki- stan. The findings are sobering: 203 incidents of sectarian violence result- ing in more than 1,800 casualties, including over 700 deaths. The Shi’a community bore the brunt of attacks from militants and terrorist organiza- tions, with some of the deadliest attacks occurring during holy months and pilgrimages. *Map from the CIA: https://www.cia.gov/library/publications/cia-maps-publications/Pakistan.html 732 N. Capitol St. N.W. , Suite A714 Washington, D.C. 20401 Phone: (202) 786-0613 [email protected] www.uscirf.gov PAKISTAN July 2013 Factsheet U.S. Commission on International Religious Freedom Pakistan While Shi’a are more at risk of becoming victims of suicide bombings and targeted shootings, the already poor religious freedom environment for Christians, Ahmadis, and Hindus continued to deteriorate, with a number violent incidents occurring against members of these communities. The information the Project gathered is based on reports and news articles available in the public domain. The Project seeks to be inclusive, tracking all reported incidents involving physical attacks targeting a member of a religious community or a major religious gathering place (church, shrine, or mosque). -

SARHAD CHAMMBER of COMMERCE and INDUSTRY Chamber House, G.T.Road, Peshawar
SARHAD CHAMMBER OF COMMERCE AND INDUSTRY Chamber House, G.T.Road, Peshawar. Tele No. +92-91-9225413-15, Fax No. +92-91-9225416 Emai.:[email protected], Websit:sccip.com.pk List of Corporate Members 2019-2020 S No Representative/Firm Name/Address NTN # STN # CNIC # 1 Shakeel Khan 7136832-3 1730113212387 24/7 Call & BPO (Pvt)Ltd 47-D Old Jamrud Road University Town Peshawar 2 Majid Zulfiqar 7143929-8 1730135068433 A & M Tours Travels and Events (Pvt)Ltd LG-203 Deans Trade Centre Peshawar Cantt 3 Qaisar Aziz 0922306-1 0501382200537 1730195842205 A Fasqa Enterprises Off: # 1, 5th Floor, Rahim Medical Centre, G.T.Road, Peshawar 4 Ishfaq Ahmed 2143316-0 0501090202273 1730116432461 A S Trading Co. Katra Neel Chowk Yadgar Peshawar 5 Shahzad Ali 2269481-1 0501360502219 1730107771859 A.I.S Trading Company 132, St # 2, Gulbahar # 1, Peshawar 6 M. Hasan Jamshed 4276319-3 1430119580665 A.J Industries (Pvt)Ltd G.T Road Pabbi Opp: Ghaznavi CNG, Peshawar 7 Mohsin Aziz 30-02-1419651-4 0307520500519 1730189397339 A.J Spinning Mills (Pvt) Ltd 90-B,Industrial Estate,Jamrud Road,Peshawar 8 Afan Aziz 1419650-6 0506551100373 1730114972413 A.J Textile Mills Limited 90-B,Industrial Estate,Jamrud Road,Peshawar 9 Adeel Rauf 1319480-1 0501290000764 1730112887923 A.Y.S Commercial Corporation Arbab Road Peshawar Cantt 10 Shakir Ullah 2250436-2 2100225043615 4230107951133 A2Z E-Payments (Pvt)Ltd 7-A 2 Z Epayments, Deans Trade Center Peshawar Cantt 11 Malik Altaf Hussain 3789794-2 2100378979419 6110119865707 AA Papers (Pvt)Ltd 30-6 GPO Link Mall Road , Peshawar 12 Sarfaraz Siraj 1147431-9 0501980502428 1730157550663 Aalee Enterprises G-3, NWR Plaza, Khyber Supper Market, Bara Road, Peshawar Cantt. -
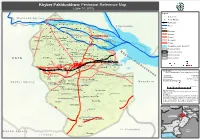
Khyber Pakhtunkhwa- Peshawar Reference Map (June 14, 2012)
Khyber Pakhtunkhwa- Peshawar Reference Map (June 14, 2012) Legend ! ! ! Settlements M o h m a n d A g e n c y ! ! ! ! ! ! "' Health Facilities WAZIRBAGH Railway Line ! ! ! ! "' ! SHA!GI BAL!A(KHAT!KI) ! ! ! Jogani "' Rivers ! C h a r s a d d a ! C h a r s a d d a ! ! ! ! ! ! Kha! tki ! ! Roads SAEED ABAD ! CHAGHAR MATTI "' FAQIR KILLAYGARA TAJIK"' Motorway ! ! "'! ! "' ! ! ! ! ! ! ! ! Highway HUSSAIN ABAD Gul Bela GUL BELLA ! "' TAKHT ABAD "' "' ! !Gar!hi S! her D!ad ! ! ! ! ! ! ! ! ! ! NASIR BAGH "' "' Primary KAFOOR DHERI Chaghar "'Matti ! "' MATHRA NAHAQI ! "' MATHRA "' KHARAKI Secondary ! Pana!m Dhe!ri ! ! ! ! ! ! ! ! ! ! ! ! ! "' ! ! ! "' CHARPERIZATakhat Abad ! "' Tertiary SUFAID DHERI PUTWAR BALLA KHAZANA ! "' ! ! "'! ! ! ! ! ! ! ! ! ! ! "' Flood Extenct (Oct -Nov 2010) ! ! Nahaqi ! Kaniza Ka!foor D!heri ! ! ! ! ! ! MA! NDRA !KHEL ! ! ! ! ! Peshawar District ! "' DARMANGI K Provincial boundary ! ! ! ! "' ! ! ! Khaza! na ! ! ! ! h "' Haryana Payan ! Mathra PAKHA GHULAM WADPAGA y District boundary ! TARAI PAYAN(SHAQI H.K) "' Kankola "' b ! ! Shahi Bala ! ! ! ! ! ! ! ! ! ! ! e Union Councils PALOSA!IUrban BUDH!AI F A T A "' ! ! "'! r ! Budhni Palosi Pajjagi ! ! P ! ! ! ! ! ! ! ! ! ! ! "' JO!GANI ! JHAGRA a Dag CHAMKAN"'I "' "' ! k REGAI PESHAWAR Laram "'BAZAR KALAN TARNAB FARM k "' "' ! Pakha Ghulam "' RASHID ABAD (NCB) h ! ! ! ! ! ! ! t ISLAMIA COLLEGE HOSPITAL, PESHAWZANANA HOSPITAL, PESHAWAR Wad Paga t ! PHANDOO PAYAN u "' "' "' Regi Palosi Lala n ! Urban Ar! ! ! LANDI ARBAB k Map Doc Name: "' h iMMAP_Peshawar District Reference -
List of Stations
Sr # Code Division Name of Retail Outlet Site Category City / District / Area Address 1 101535 Karachi AHMED SERVICE STATION N/V CF KARACHI EAST DADABHOY NOROJI ROAD AKASHMIR ROAD 2 101536 Karachi CHAND SUPER SERVICE N/V CF KARACHI WEST PSO RETAIL DEALERSST/1-A BLOCK 17F 3 101537 Karachi GLOBAL PETROLEUM SERVICE N/V CF KARACHI EAST PLOT NO. 234SECTOR NO.3, 4 101538 Karachi FAISAL SERVICE STATION N/V CF KARACHI WEST ST 1-A BLOCK 6FEDERAL B AREADISTT K 5 101540 Karachi RAANA GASOLINE N/V CF KARACHI WEST SERVICE STATIONPSO RETAIL DEALERAPWA SCHOOL LIAQA 6 101543 Karachi SHAHGHAZI P/S N/V DFA MALIR SURVEY#81,45/ 46 KM SUPER HIGHWAY 7 101544 Karachi GARDEN PETROL SERVICE N/V CF KARACHI SOUTH OPP FATIMA JINNAHGIRLS HIGH SCHOOLN 8 101545 Karachi RAZA PETROL SERVICE N/V CF KARACHI SOUTH 282/2 LAWRENCE ROADKARACHIDISTT KARACHI-SOUTH 9 101548 Karachi FANCY SERVICE STATION N/V CF KARACHI WEST ST-1A BLOCK 10FEDERAL B AREADISTT KARACHI WEST 10 101550 Karachi SIDDIQI SERVIC STATION S/S DFB KARACHI EAST RASHID MINHAS ROADKARACHIDISTT KARACHI EAST 11 101555 Karachi EASTERN SERIVCE STN N/V DFA KARACHI WEST D-201 SITEDIST KARACHI-WEST 12 101562 Karachi AL-YASIN FILL STN N/V DFA KARACHI WEST ST-1/2 15-A/1 NORTHKAR TOWNSHIP KAR WEST 13 101563 Karachi DUREJI FILLING STATION S/S DFA LASBELA KM-4/5 HUB-DUREJI RDPATHRO HUBLASBE 14 101566 Karachi R C D FILLING STATION N/V DFA LASBELA HUB CHOWKI LASBELADISTT LASBELA 15 101573 Karachi FAROOQ SERVICE CENTRE N/V CF KARACHI WEST N SIDDIQ ALI KHAN ROADCHOWRANGI NO-3NAZIMABADDISTT 16 101577 Karachi METRO SERVICE STATION -

Polio NL Jan 2019.Fh10
Volume: VIII/MMXIX - Issue No. 01 poliopolio++January 2019 A Rotary Delegation from USA visit Pakistan to participate in the January 2019 NIDs. (story on page 04 & 05) January 2019 NIDs: Every Last Child Chitral: A member of the polio eradication team administers vaccination drops to a child during campaign outside a house in the snow covered region of Lowari tunnel on Jan 28th. Photo courtesy: DAWN newspaper The New Year heralds a new dawn; a year of hope and optimismto put an end to the transmission of polio virus. Not to say our efforts have been in vain in 2018, but we need to redouble our efforts in 2019. We are unwavering in our support, equipped with the tools, the people and the determination. I would like to share some experts of my speech at the International Assembly for a gathering of Governor Elects in San Diego, on 17th January 2019. “Through our hard work and persistence, we have made astonishing progress since we formed the GPEI in 1988. We have reduced the cases to 99.9%.” In 2018, we saw 33 cases in two countries, Pakistan & Afghanistan. We must keep pushing with patience and resolve, for in Rotary, We can and we will eradicate this disease, but to do so we are facing unique challenges. Now the membership must apply our energy and creativity to innovate, so we can deliver vaccines to more children in the hardest to reach areas and focus on making surveillance system better than before, in Afghanistan, Nigeria and Pakistan. The partnership is redoubling efforts to address the issues, of conflict in security compromised zones, remote geographies, inaccessible highly volatile population and other logistic challenge.