(S1) Profile of Atmospheric Pahs in Rawalpindi, Lahore And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

S# BRANCH CODE BRANCH NAME CITY ADDRESS 1 24 Abbottabad
BRANCH S# BRANCH NAME CITY ADDRESS CODE 1 24 Abbottabad Abbottabad Mansera Road Abbottabad 2 312 Sarwar Mall Abbottabad Sarwar Mall, Mansehra Road Abbottabad 3 345 Jinnahabad Abbottabad PMA Link Road, Jinnahabad Abbottabad 4 131 Kamra Attock Cantonment Board Mini Plaza G. T. Road Kamra. 5 197 Attock City Branch Attock Ahmad Plaza Opposite Railway Park Pleader Lane Attock City 6 25 Bahawalpur Bahawalpur 1 - Noor Mahal Road Bahawalpur 7 261 Bahawalpur Cantt Bahawalpur Al-Mohafiz Shopping Complex, Pelican Road, Opposite CMH, Bahawalpur Cantt 8 251 Bhakkar Bhakkar Al-Qaim Plaza, Chisti Chowk, Jhang Road, Bhakkar 9 161 D.G Khan Dera Ghazi Khan Jampur Road Dera Ghazi Khan 10 69 D.I.Khan Dera Ismail Khan Kaif Gulbahar Building A. Q. Khan. Chowk Circular Road D. I. Khan 11 9 Faisalabad Main Faisalabad Mezan Executive Tower 4 Liaqat Road Faisalabad 12 50 Peoples Colony Faisalabad Peoples Colony Faisalabad 13 142 Satyana Road Faisalabad 585-I Block B People's Colony #1 Satayana Road Faisalabad 14 244 Susan Road Faisalabad Plot # 291, East Susan Road, Faisalabad 15 241 Ghari Habibullah Ghari Habibullah Kashmir Road, Ghari Habibullah, Tehsil Balakot, District Mansehra 16 12 G.T. Road Gujranwala Opposite General Bus Stand G.T. Road Gujranwala 17 172 Gujranwala Cantt Gujranwala Kent Plaza Quide-e-Azam Avenue Gujranwala Cantt. 18 123 Kharian Gujrat Raza Building Main G.T. Road Kharian 19 125 Haripur Haripur G. T. Road Shahrah-e-Hazara Haripur 20 344 Hassan abdal Hassan Abdal Near Lari Adda, Hassanabdal, District Attock 21 216 Hattar Hattar -
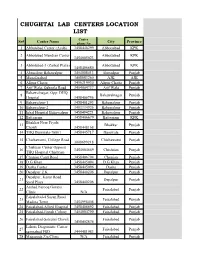
Chughtai Lab Centers Location List
CHUGHTAI LAB CENTERS LOCATION LIST Center Sr# Center Name City Province phone No 1 Abbotabad Center (Ayub) 3458448299 Abbottabad KPK 2 Abbotabad Mandian Center Abbottabad KPK 3454005023 3 Abbotabad-3 (Zarbat Plaza) Abbottabad KPK 3458406680 4 Ahmedpur Bahawalpur 3454008413 Ahmedpur Punjab 5 Muzafarabad 3408883260 AJK AJK 6 Alipur Chatta 3456219930 Alipur Chatta Punjab 7 Arif Wala, Qaboola Road 3454004737 Arif Wala Punjab Bahawalnagar, Opp: DHQ 8 Bahawalnagar Punjab Hospital 3458406756 9 Bahawalpur-1 3458401293 Bahawalpur Punjab 10 Bahawalpur-2 3403334926 Bahawalpur Punjab 11 Iqbal Hospital Bahawalpur 3458494221 Bahawalpur Punjab 12 Battgaram 3458406679 Battgaram KPK Bhakhar Near Piyala 13 Bhakkar Punjab Chowk 3458448168 14 THQ Burewala-76001 3458445717 Burewala Punjab 15 Chichawatni, College Road Chichawatni Punjab 3008699218 Chishtian Center Opposit 16 3454004669 Chishtian Punjab THQ Hospital Chishtian 17 Chunian Cantt Road 3458406794 Chunian Punjab 18 D.G Khan 3458445094 D.G Khan Punjab 19 Daska Center 3458445096 Daska Punjab 20 Depalpur Z.K 3458440206 Depalpur Punjab Depalpur, Kasur Road 21 Depalpur Punjab Syed Plaza 3458440206 Arshad Farooq Goraya 22 Faisalabad Punjab Clinic N/A Faisalabad-4 Susan Road 23 Faisalabad Punjab Madina Town 3454998408 24 Faisalabad-Allied Hospital 3458406692 Faisalabad Punjab 25 Faisalabad-Jinnah Colony 3454004790 Faisalabad Punjab 26 Faisalabad-Saleemi Chowk Faisalabad Punjab 3458402874 Lahore Diagonistic Center 27 Faisalabad Punjab samnabad FSD 3444481983 28 Maqsooda Zia Clinic N/A Faisalabad Punjab Farooqabad, -

Islamabad: Rawalpindi: Lahore: Karachi: Quetta
Contact list – Photo Studios - Pakistan The list below of photo studios in Pakistan has been compiled by the Australian High Commission, based on past experience, for client convenience only. The Australian High Commission does not endorse any of the photo studios appearing in the list, provides no guarantees as to their quality and does not accept any liability if you choose to engage one of these photo studios. Islamabad: Simco Photo Studio and Digital Colour Lab Photech Block 9-E, School Road, F-6 Markaz, Super Shop No. 7, Block 12, School Road, F-6 Markaz, Market, Islamabad – Pakistan, Super Market, Islamabad 051-2822600, 051-2826966 051-2275588, 051-2874583 Rawalpindi: Lahore: Jumbo Digital Lab & Photo Studio AB Digital Color Lab and Studio Chandni Chowk, Murree Road, Rawalpindi Kashif Centre, 80-Chowk Nisbat Road 051-4906923, 051-4906089, 051-4456088 Lahore – Pakistan, 042-37226496, 042-37226611 Karachi: Dossani’s Studio Disney’s Digital Photo Studio Hashoo Terrace, Khayaban-e-Roomi, Boat Basin, Shop No. 3, Decent Tower Shopping Centre, Clifton , Karachi, Gulistan-e-Johar, Block 15, Karachi Tell: +92-21-34013293, 0300-2932088 021-35835547, 021-35372609 Quetta: Sialkot Yadgar Digital Studio Qazi Studio Hussain Abad, Colonal Yunas Road, Hazara Qazi Mentions Town, Quetta. 0343-8020586 Railay Road Sialkot – Pakistan 052-4586083, 04595080 Peshawar: Azeem Studio & Digital Labs 467-Saddar Road Peshawar Cantt Tell: +91-5274812, +91-5271482 Camera Operator Guidelines: Camera: Prints: - High-quality digital or film camera - Print size 35mm -

Usg Humanitarian Assistance to Pakistan in Areas
USG HUMANITARIAN ASSISTANCE TO CONFLICT-AFFECTED POPULATIONS IN PAKISTAN IN FY 2009 AND TO DATE IN FY 2010 Faizabad KEY TAJIKISTAN USAID/OFDA USAID/Pakistan USDA USAID/FFP State/PRM DoD Amu darya AAgriculture and Food Security S Livelihood Recovery PAKISTAN Assistance to Conflict-Affected y Local Food Purchase Populations ELogistics Economic Recovery ChitralChitral Kunar Nutrition Cand Market Systems F Protection r Education G ve Gilgit V ri l Risk Reduction a r Emergency Relief Supplies it a h Shelter and Settlements C e Food For Progress I Title II Food Assistance Shunji gol DHealth Gilgit Humanitarian Coordination JWater, Sanitation, and Hygiene B and Information Management 12/04/09 Indus FAFA N A NWFPNWFP Chilas NWFP AND FATA SEE INSET UpperUpper DirDir SwatSwat U.N. Agencies, E KohistanKohistan Mahmud-e B y Da Raqi NGOs AGCJI F Asadabad Charikar WFP Saidu KUNARKUNAR LowerLower ShanglaShangla BatagramBatagram GoP, NGOs, BajaurBajaur AgencyAgency DirDir Mingora l y VIJaKunar tro Con ImplementingMehtarlam Partners of ne CS A MalakandMalakand PaPa Li Î! MohmandMohmand Kabul Daggar MansehraMansehra UNHCR, ICRC Jalalabad AgencyAgency BunerBuner Ghalanai MardanMardan INDIA GoP e Cha Muzaffarabad Tithwal rsa Mardan dd GoP a a PeshawarPeshawar SwabiSwabi AbbottabadAbbottabad y enc Peshawar Ag Jamrud NowsheraNowshera HaripurHaripur AJKAJK Parachinar ber Khy Attock Punch Sadda OrakzaiOrakzai TribalTribal AreaArea Î! Adj.Adj. PeshawarPeshawar KurrumKurrum AgencyAgency Islamabad Gardez TribalTribal AreaArea AgencyAgency Kohat Adj.Adj. KohatKohat Rawalpindi HanguHangu Kotli AFGHANISTAN KohatKohat ISLAMABADISLAMABAD Thal Mangla reservoir TribalTribal AreaArea AdjacentAdjacent KarakKarak FATAFATA BannuBannu us Bannu Ind " WFP Humanitarian Hub NorthNorth WWaziristanaziristan BannuBannu SOURCE: WFP, 11/30/09 Bhimbar AgencyAgency SwatSwat" TribalTribal AreaArea " Adj.Adj. -

Sr. No College Name District Gender Division Contact 1 GOVT
Sr. College Name District Gender Division Contact No 1 GOVT. COLLEGE FOR WOMEN ATTOCK ATTOCK Female RAWALPINDI 572613336 2 GOVT. DEGREE COLLEGE FOR WOMEN FATEH JANG, ATTOCK ATTOCK Female RAWALPINDI 572212505 3 GOVT. COLLEGE FOR WOMEN PINDI GHEB, ATTOCK ATTOCK Female RAWALPINDI 4 GOVT. DEGREE COLLEGE FOR WOMEN, JAND ATTOCK ATTOCK Female RAWALPINDI 572621847 5 GOVT. DEGREE COLLEGE FOR WOMEN HASSAN ABDAL ATTOCK ATTOCK Female RAWALPINDI 6 GOVT. DEGREE COLLEGE FOR WOMEN HAZRO, ATTOCK ATTOCK Female RAWALPINDI 572312884 7 GOVT. POST GRADUATE COLLEGE ATTOCK ATTOCK Male RAWALPINDI 579316163 8 Govt. Commerce College, Attock ATTOCK Male RAWALPINDI 9 GOVT. DEGREE COLLEGE FATEH JANG ATTOCK ATTOCK Male RAWALPINDI 10 GOVT. INTER COLLEGE OF BOYS, BAHTAR, ATTOCK ATTOCK Male RAWALPINDI 11 GOVT. DEGREE COLLEGE (BOYS) PINDI GHEB ATTOCK ATTOCK Male RAWALPINDI 572352909 12 Govt. Institute of Commerce, Pindigheb ATTOCK Male RAWALPINDI 572352470 13 GOVT. DEGREE COLLEGE BOYS, JAND, ATTOCK ATTOCK Male RAWALPINDI 572622310 14 GOVT. INTER COLLEGE NARRAH KANJOOR CHHAB ATTOCK ATTOCK Male RAWALPINDI 572624005 15 GOVT. DEGREE COLLEGE BASAL ATTOCK ATTOCK Male RAWALPINDI 572631414 16 Govt. Institute of Commerce, Jand ATTOCK Male RAWALPINDI 572621186 17 GOVT. DEGREE COLLEGE FOR BOYS HASSAN ABDAL, ATTOCK ATTOCK Male RAWALPINDI 18 GOVT.SHUJA KHANZADA SHAHEED DEGREE COLLEGE, HAZRO, ATTOCK ATTOCK Male RAWALPINDI 572312612 19 GOVT. COLLEGE FOR WOMEN CHAKWAL CHAKWAL Female RAWALPINDI 543550957 20 GOVT. DEGREE COLLEGE FOR WOMEN , DHADIAL , CHAKWAL CHAKWAL Female RAWALPINDI 543590066 21 GOVT. DEGREE COLLEGE FOR WOMEN MULHAL MUGHLAN, CHAKWAL CHAKWAL Female RAWALPINDI 543585081 22 GOVT. DEGREE COLLEGE FOR WOMEN BALKASSAR , CHAKWAL CHAKWAL Female RAWALPINDI 543569888 23 Govt Degree College for women Ara Basharat tehsil choa Saidan Shah chakwal CHAKWAL Female RAWALPINDI 543579210 24 GOVT. -

Survey of Ecotourism Potential in Pakistan's Biodiversity Project Area (Chitral and Northern Areas): Consultancy Report for IU
Survey of ecotourism potential in Pakistan’s biodiversity project area (Chitral and northern areas): Consultancy report for IUCN Pakistan John Mock and Kimberley O'Neil 1996 Keywords: conservation, development, biodiversity, ecotourism, trekking, environmental impacts, environmental degradation, deforestation, code of conduct, policies, Chitral, Pakistan. 1.0.0. Introduction In Pakistan, the National Tourism Policy and the National Conservation Strategy emphasize the crucial interdependence between tourism and the environment. Tourism has a significant impact upon the physical and social environment, while, at the same time, tourism's success depends on the continued well-being of the environment. Because the physical and social environment constitutes the resource base for tourism, tourism has a vested interest in conserving and strengthening this resource base. Hence, conserving and strengthening biodiversity can be said to hold the key to tourism's success. The interdependence between tourism and the environment is recognized worldwide. A recent survey by the Industry and Environment Office of the United Nations Environment Programme (UNEP/IE) shows that the resource most essential for the growth of tourism is the environment (UNEP 1995:7). Tourism is an environmentally-sensitive industry whose growth is dependent upon the quality of the environment. Tourism growth will cease when negative environmental effects diminish the tourism experience. By providing rural communities with the skills to manage the environment, the GEF/UNDP funded project "Maintaining Biodiversity in Pakistan with Rural Community Development" (Biodiversity Project), intends to involve local communities in tourism development. The Biodiversity Project also recognizes the potential need to involve private companies in the implementation of tourism plans (PC II:9). -

PRCS Sitrep No.6, Monsoon Floods 15Th Sep, 14
MONSOON 2014 Info Report - 6: Dated 15-09-14 18-09- HIGHLIGHT Forecast from Pakistan Meteorological Department says “Seasonal low lies over north Baluchistan and adjoining areas. A shallow trough of westerly wave is also prevailing over Kashmir and adjoining areas”. As per the report of NDMA dated 14th September, 2014, Monsoon rains have affected 2,459,704 individuals caused 301 deaths and 507 people got injured in AJK, Punjab and GB. As per UNOCH report of 11th September, the authorities expect an estimated 3 million people to be affected by the floods in the coming days. PRCS is responding in Punjab, AJK, GB and Sindh with an initial plan to assist 13,000 families (91,000 indiv), with provision of food, non food items, emergency shelter and health and care services. In Punjab three PRCS health units have already started working and disaster preparedness stocks are being sent to the affected districts for distribution. So far PRCS Punjab Provincial Branch has distributed 2,350 x food packs to the flood affected families of Jhang, Sialkot, Shikarpur, Chinniot, Gujrat, Hafizabad and Toba Take Singh. In GB 70 x NFIs have been distributed among the flood affected families of Astor District. In AJK 840 families have been assisted with provision of emergency shelter and NFIs in district Bagh, Poonch, Haveli and Muzafarabad. 2 MHUs have also been deployed in District Haveli today. So far, 51 patients were treated in Hallan Shamil of Union Council Kala Mula, District Haveli. than 15,200 flood afected people all over Pakistan with services including food and non food items provision, 1.WEATHER OUTLOOK (as of 15th Sep,2014 at 1045 hrs by pak met) HYDROLOGICAL SITUATION: River Chenab at Punjnad is in High Flood Level. -

Transportation Disadvantage and Activity Participation in the Cities of Rawalpindi and Islamabad, Pakistan
Muhammad Adeel, Anthony G.O Yeh, Zhang Feng Transportation disadvantage and activity participation in the cities of Rawalpindi and Islamabad, Pakistan Article (Accepted version) (Refereed) Original citation: Adeel, Muhammad, Yeh, Anthony Gar-On and Zhang, Feng (2016) Transportation disadvantage and activity participation in the cities of Rawalpindi and Islamabad, Pakistan. Transport Policy, 47 . pp. 1-12. ISSN 0967-070X DOI: 10.1016/j.tranpol.2015.12.001 © 2015 Elsevier Ltd. This version available at: http://eprints.lse.ac.uk/65025/ Available in LSE Research Online: January 2016 LSE has developed LSE Research Online so that users may access research output of the School. Copyright © and Moral Rights for the papers on this site are retained by the individual authors and/or other copyright owners. Users may download and/or print one copy of any article(s) in LSE Research Online to facilitate their private study or for non-commercial research. You may not engage in further distribution of the material or use it for any profit-making activities or any commercial gain. You may freely distribute the URL (http://eprints.lse.ac.uk) of the LSE Research Online website. This document is the author’s final accepted version of the journal article. There may be differences between this version and the published version. You are advised to consult the publisher’s version if you wish to cite from it. Transportation disadvantage and activity participation in the twin cities of Rawalpindi and Islamabad, Pakistan Muhammad Adeel Corresponding Author [email protected] Research Officer (Spatial Analyst) LSE Cities / LSE Kuwait Programme, London School of Economics and Political Science Houghton Street, London WC2A 2AE, United Kingdom Tel: +44 (0)20 7852 3631 Anthony G.O Yeh [email protected] Chair Professor Department of Urban Planning and Design, The University of Hong Kong (HKU), 8F, Knowels Building, Pokfulam Road Hong Kong, S.A.R., China Dr. -

Rahim Yar Khan District Is a District in the Punjab Province of Pakistan, the City of Rahim Yar Khan Is the Capital
World Water Day April-2011 17 DRINKING WATER QUALITY CHALLENGES IN PAKISTAN By Z. A. Soomro1, Dr. M. I. A. Khokhar, W. Hussain and M. Hussain Abstract: Pakistan is facing drastic decrease in per capita water availability due to rapid increase in population. The water shortage and increasing competition for multiple uses of water has adversely affected the quality of water. Pakistan Council of Research in Water Resources has launched a national water quality monitoring program. This program covered water sampling and their analysis from 21 major cities. The water samples were analyzed for physical, chemical and bacteriological contamination. Results showed that most of the samples in all four provinces are microbiologically contaminated. Arsenic problem is major in cities of Punjab, Nitrate contamination in Balochistan, Iron contamination in KPK and higher turbidity values found in water samples found in Sindh. This valuable data would serve the regulatory bodies and implementing authorities towards the quality drinking water supply. Key words: Water Quality, Surface water, Groundwater contamination, Hand pumps, Pollution, Microbiology, Chemical contamination. 1. INTRODUCTION Nature has blessed Pakistan with adequate surface and groundwater resources. However, rapid population growth, urbanization and the continued industrial development has placed immense stress on water resources of the country. The extended droughts and non-development of additional water resources have further aggravated the water scarcity situation. Pakistan has been blessed with abundance of availability of surface and ground water resources to the tune of 128300 million m3 and 50579 million m3 per year respectively (The Pakistan National Conservation Strategy, 1992).Consequently per capita water availability has decreased from 5600 m3 to 1000 m3 / annum(Water quality status 2003). -

Towards an Inclusive Public Transport System in Pakistan1
TOWARDS AN INCLUSIVE PUBLIC TRANSPORT SYSTEM IN PAKISTAN1 Muhammad Adeel, Anthony G.O Yeh and Zhang Feng2 Abstract Urban transport in Pakistan is characterized by the coexistence of formal and informal transit services. While urban transport is deregulated and - somehow – multimodal in the country, the transport service providers often compete with each other within their particular constrains and their equilibrium defines the overall landscape of urban accessibility. With examples from the cities of Islamabad and Rawalpindi, the paper discusses three broad constraints on the urban modes of transportation, namely regulatory, spatial and demand related constraints, using a number of important system characteristics. Results show that the overall level of constraints remains ‘Very High’ on the newly constructed BRT, followed by ‘High’ constraints on the informal paratransit mode, ‘Qinqui’. Whereas the Suzuki and Wagon modes coverage remains maximum and they carry relatively lower level of constraints. In this context, an inclusive urban mobility largely depends on a proactive approach by management authorities to minimize these constraints through a number of initiatives including integration of modes, improvements of the quality of service and condition of vehicle, and by facilitating the mobility of women and non-motorized travellers. Keywords: Transport, accessibility, Pakistan, BRT, Qingqi 1. BACKGROUND Population explosion and rapid urbanization in Asian countries have brought complex mobility challenges for a vast majority of their people who also face issues of poverty, inequality and limited access to basic services (Gakenheimer, 1999). While the average distances between activities are increasing with time, so are the issues of mobility and accessibility. Lack of access to public transport, poor quality of transportation infrastructure, rising levels of personal automobile ownership and a persistent disregard of traffic regulations pose further issues to the already challenging mobility environment (Dimitriou and Gakenheimer, 2011). -
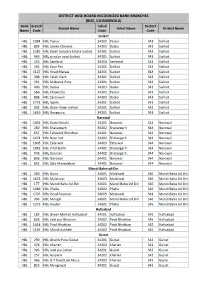
District Wise Board Recognized Bank Branches
DISTRICT WISE BOARD RECOGNIZED BANK BRANCHES (BISE, GUJRANWALA) Bank Branch Tehsil District Branch Name Tehsil Name District Name Name Code Code Code Sialkot HBL 1084 HBL Pasrur 34302 Pasrur 343 Sialkot HBL 895 HBL Jamke Cheema 34303 Daska 343 Sialkot HBL 1285 HBL Small Industry Estate Sialkot 34301 Sialkot 343 Sialkot HBL 969 HBL circular road Sialkot 34301 Sialkot 343 Sialkot HBL 425 HBL Sambrial 34304 Sambrial 343 Sialkot HBL 492 HBL Koor Pur 34301 Sialkot 343 Sialkot HBL 1127 HBL Head Marala 34301 Sialkot 343 Sialkot HBL 308 HBL Fateh Garh 34301 Sialkot 343 Sialkot HBL 291 HBL Mubarak Pura 34301 Sialkot 343 Sialkot HBL 406 HBL Daska 34303 Daska 343 Sialkot HBL 566 HBL Chawinda 34302 Pasrur 343 Sialkot HBL 808 HBL Saranwali 34303 Daska 343 Sialkot HBL 1773 HBL Ugoki 34301 Sialkot 343 Sialkot HBL 992 HBL Bazar Kalan Sialkot 34301 Sialkot 343 Sialkot HBL 1619 HBL Rungpura 34301 Sialkot 343 Sialkot Narowal HBL 1405 HBL Bado Malahi 34401 Narowal 344 Narowal HBL 260 HBL Shakargarh 34402 Shakargarh 344 Narowal HBL 637 HBL Talwandi Bhindran 34401 Narowal 344 Narowal HBL 1474 HBL Noor kot 34402 Shakargarh 344 Narowal HBL 1805 HBL Zafarwal 34403 Zafarwal 344 Narowal HBL 1842 HBL Pindi Bohri 34401 Shakargarh 344 Narowal HBL 978 HBL Darman 34402 Shakargarh 344 Narowal HBL 836 HBL Narowal 34401 Narowal 344 Narowal HBL 852 HBL Qila Ahmedabad 34401 Narowal 344 Narowal Mandi Baha-ud-Din HBL 560 HBL Gojra 34601 Malakwal 346 Mandi Baha Ud Din HBL 1623 HBL Malakwal 34603 Malakwal 346 Mandi Baha Ud Din HBL 177 HBL Mandi Baha Ud Din 34601 Mandi Baha Ud -
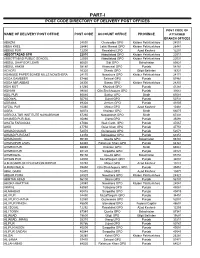
Part-I: Post Code Directory of Delivery Post Offices
PART-I POST CODE DIRECTORY OF DELIVERY POST OFFICES POST CODE OF NAME OF DELIVERY POST OFFICE POST CODE ACCOUNT OFFICE PROVINCE ATTACHED BRANCH OFFICES ABAZAI 24550 Charsadda GPO Khyber Pakhtunkhwa 24551 ABBA KHEL 28440 Lakki Marwat GPO Khyber Pakhtunkhwa 28441 ABBAS PUR 12200 Rawalakot GPO Azad Kashmir 12201 ABBOTTABAD GPO 22010 Abbottabad GPO Khyber Pakhtunkhwa 22011 ABBOTTABAD PUBLIC SCHOOL 22030 Abbottabad GPO Khyber Pakhtunkhwa 22031 ABDUL GHAFOOR LEHRI 80820 Sibi GPO Balochistan 80821 ABDUL HAKIM 58180 Khanewal GPO Punjab 58181 ACHORI 16320 Skardu GPO Gilgit Baltistan 16321 ADAMJEE PAPER BOARD MILLS NOWSHERA 24170 Nowshera GPO Khyber Pakhtunkhwa 24171 ADDA GAMBEER 57460 Sahiwal GPO Punjab 57461 ADDA MIR ABBAS 28300 Bannu GPO Khyber Pakhtunkhwa 28301 ADHI KOT 41260 Khushab GPO Punjab 41261 ADHIAN 39060 Qila Sheikhupura GPO Punjab 39061 ADIL PUR 65080 Sukkur GPO Sindh 65081 ADOWAL 50730 Gujrat GPO Punjab 50731 ADRANA 49304 Jhelum GPO Punjab 49305 AFZAL PUR 10360 Mirpur GPO Azad Kashmir 10361 AGRA 66074 Khairpur GPO Sindh 66075 AGRICULTUR INSTITUTE NAWABSHAH 67230 Nawabshah GPO Sindh 67231 AHAMED PUR SIAL 35090 Jhang GPO Punjab 35091 AHATA FAROOQIA 47066 Wah Cantt. GPO Punjab 47067 AHDI 47750 Gujar Khan GPO Punjab 47751 AHMAD NAGAR 52070 Gujranwala GPO Punjab 52071 AHMAD PUR EAST 63350 Bahawalpur GPO Punjab 63351 AHMADOON 96100 Quetta GPO Balochistan 96101 AHMADPUR LAMA 64380 Rahimyar Khan GPO Punjab 64381 AHMED PUR 66040 Khairpur GPO Sindh 66041 AHMED PUR 40120 Sargodha GPO Punjab 40121 AHMEDWAL 95150 Quetta GPO Balochistan 95151