Prenatal Development Timeline
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

3 Embryology and Development
BIOL 6505 − INTRODUCTION TO FETAL MEDICINE 3. EMBRYOLOGY AND DEVELOPMENT Arlet G. Kurkchubasche, M.D. INTRODUCTION Embryology – the field of study that pertains to the developing organism/human Basic embryology –usually taught in the chronologic sequence of events. These events are the basis for understanding the congenital anomalies that we encounter in the fetus, and help explain the relationships to other organ system concerns. Below is a synopsis of some of the critical steps in embryogenesis from the anatomic rather than molecular basis. These concepts will be more intuitive and evident in conjunction with diagrams and animated sequences. This text is a synopsis of material provided in Langman’s Medical Embryology, 9th ed. First week – ovulation to fertilization to implantation Fertilization restores 1) the diploid number of chromosomes, 2) determines the chromosomal sex and 3) initiates cleavage. Cleavage of the fertilized ovum results in mitotic divisions generating blastomeres that form a 16-cell morula. The dense morula develops a central cavity and now forms the blastocyst, which restructures into 2 components. The inner cell mass forms the embryoblast and outer cell mass the trophoblast. Consequences for fetal management: Variances in cleavage, i.e. splitting of the zygote at various stages/locations - leads to monozygotic twinning with various relationships of the fetal membranes. Cleavage at later weeks will lead to conjoined twinning. Second week: the week of twos – marked by bilaminar germ disc formation. Commences with blastocyst partially embedded in endometrial stroma Trophoblast forms – 1) cytotrophoblast – mitotic cells that coalesce to form 2) syncytiotrophoblast – erodes into maternal tissues, forms lacunae which are critical to development of the uteroplacental circulation. -

Te2, Part Iii
TERMINOLOGIA EMBRYOLOGICA Second Edition International Embryological Terminology FIPAT The Federative International Programme for Anatomical Terminology A programme of the International Federation of Associations of Anatomists (IFAA) TE2, PART III Contents Caput V: Organogenesis Chapter 5: Organogenesis (continued) Systema respiratorium Respiratory system Systema urinarium Urinary system Systemata genitalia Genital systems Coeloma Coelom Glandulae endocrinae Endocrine glands Systema cardiovasculare Cardiovascular system Systema lymphoideum Lymphoid system Bibliographic Reference Citation: FIPAT. Terminologia Embryologica. 2nd ed. FIPAT.library.dal.ca. Federative International Programme for Anatomical Terminology, February 2017 Published pending approval by the General Assembly at the next Congress of IFAA (2019) Creative Commons License: The publication of Terminologia Embryologica is under a Creative Commons Attribution-NoDerivatives 4.0 International (CC BY-ND 4.0) license The individual terms in this terminology are within the public domain. Statements about terms being part of this international standard terminology should use the above bibliographic reference to cite this terminology. The unaltered PDF files of this terminology may be freely copied and distributed by users. IFAA member societies are authorized to publish translations of this terminology. Authors of other works that might be considered derivative should write to the Chair of FIPAT for permission to publish a derivative work. Caput V: ORGANOGENESIS Chapter 5: ORGANOGENESIS -

Download PDF Version
FIG. 4–1 Dorsal aspect of the 10-somite embryo. 24 IV the fourth week of life somite and neural tube period I. EMBRYO PROPER caudal openings of the tube are called neuropores. The rostral neuropore closes between 18 and 20 somites. The caudal neuro- A. EXTERNAL APPEARANCE pore closes at 25 somites. Figs. 4–1, 4–2 1. The specimens measure approximately 1 to 3.5 mm in length Brain and have 1 to 29 pairs of somites. Three brain subdivisions are present in the cranial portion of the 2. The head and tail folds move the attachment of the amnion tube and are named, from cranial to caudal, the prosencephalon, to the ventral side of the head and tail regions, respectively. mesencephalon and rhombencephalon. The boundary between the The lateral body folds move the amnion attachment to the pros- and mesencephalon is demarcated by a ventral bend, called ventrolateral surface in the midportion of the embryo. the cephalic flexure. An external groove and a prominent swelling 3. The head region is elevated above the yolk sac by the large on the medial surface of the neural plate may also demarcate the pericardial sac, the midportion lies upon the yolk sac and the boundary. The boundary between the mes- and rhombencephalon caudal region is curved toward the yolk sac. is distinguished by a groove on the medial and lateral surfaces of 4. The embryo possesses somites, which are apparent through the neural plate or tube. the ectoderm. 5. The neural tube develops from the neural plate and remains Prosencephalon open at each end for 2 to 4 days. -

A 29-Year-Old Man with Acute Onset Blurry Vision, Weakness, and Gait Abnormality
Journal of the Louisiana State Medical Society CLINICAL CASE OF THE MONTH A 29-Year-Old Man With Acute Onset Blurry Vision, Weakness, and Gait Abnormality Deepu Thoppil, MD; Murtuza J. Ali, MD; Neeraj Jain, MD; Sanjay Kamboj, MD; Pramilla Subramaniam, MD; and Fred A. Lopez, MD (Section Editor) A 29-year-old man, with no significant past medical history, was in his usual state of health until the afternoon of admission. The patient was seated at work eating lunch when he suddenly noticed that his vision became blurry. He covered his right eye and had no visual difficulty but noted blurry vision upon covering his left eye. At this point, the patient tried to stand up, but had difficulty walking and noticed he was “falling toward his left.” Facial asymmetry when smiling was also appreciated. The patient denied any alteration in mental status, confusion, antecedent or current headaches, aura, chest pains, or shortness of breath. He was not taking any prescribed medications and had no known allergies. The patient denied any prior hospitalization or surgery. He denied use of tobacco, alcohol, or illicit drugs, and worked as a maintenance worker in a hotel. His family history is remarkable for his father who died of pancreatic cancer in his 50s and his mother who died of an unknown heart condition in her late 40s. Vital signs on presentation to the emergency department included temperature of 97.6oF; respiratory rate of 18 per minute; pulse of 68 per minute; blood pressure of 124/84 mmHg; pulse oximetry of 99% on ambient air. -

Folding of Embryo
❑There is progressive increase in the size of the embryonic disc due to rapid growth of cells of central part of embryonic disc and rapid growth of somites. ❑ This causes conversion of flat pear-shaped germ disc into a cylindrical embryo. ❑The head and tail ends of the disc remain relatively close together.The increased length of the disc causes it to bulge upward into the amniotic cavity. ❑With the formation of the head and tail folds, parts of the yolk sac become enclosed within the embryo. ❑ In this way, a tube lined by endoderm is formed in the embryo. This is the primitive gut, from which most of the gastrointestinal tract is derived. ❑ At first, the gut is in wide communication with the yolk sac. The part of the gut cranial to this communication is called the foregut; the part caudal to the communication is called the hindgut; while the intervening part is called the midgut . ❑The communication with the yolk sac becomes progressively narrower. As a result of these changes, the yolk sac becomes small and inconspicuous, and is now termed the definitive yolk sac (also called the umbilical vesicle). ❑The narrow channel connecting it to the gut is called the vitellointestinal duct (also called vitelline duct; yolk stalk or omphalomesenteric duct). This duct becomes elongated and eventually disappears. ❑With the formation of the cavity, the embryo (along with the amniotic cavity and yolk sac) remains attached to the trophoblast only by extraembryonic mesoderm into which the coelom does not exist. This extraembryonic mesoderm forms the connecting stalk. -

Development of Right Ventricle
DEVELOPMENT OF THE HEART II. David Lendvai M.D., Ph.D. Mark Kozsurek, M.D., Ph.D. • Septation of the common atrioventricular (AV) orifice. • Formation of the interatrial septum. • Formation of the muscular interventricular septum. • Appearance of the membranous interventricular septum and the spiral aorticopulmonary septum. right left septum primum septum primum septum primum septum primum septum primum septum primum foramen primum foramen primum septum primum septum primum foramen primum foramen primum septum primum septum primum foramen secundum foramen secundum foramen primum foramen primum septum primum foramen secundum septum primum foramen secundum foramen primum foramen primum septum primum septum primum foramen secundum foramen secundum septum secundum septum secundum foramen secundum foramen ovale foramen ovale septum primum septum primum septum secundum septum secundum foramen secundum foramen ovale foramen ovale septum primum septum primum septum secundum septum secundum foramen secundum septum primum foramen ovale foramen ovale septum primum SUMMARY • The septation of the common atrium starts with the appearance of the crescent-shaped septum primum. The opening of this septum, the foramen primum, becomes progressively smaller. • Before the foramen primum completly closes, postero-superiorly several small openings appear on the septum primum. These perforations coalesce later and form the foramen secundum. • On the right side of the septum primum a new septum, the septum secundum, starts to grow. The orifice of the septum secundum is the foramen ovale. • Finally two crescent-like, incomplete, partially overlapping septa exist with one hole on each. Septum secundum is more rigid and the septum primum on its left side acts as a valve letting the blood flow exclusively from the right to the left. -

Persistent Patent Foramen Ovale in Adult Male
Internatiional Journal of Biioassays ISSN: 2278-778X www.ijbio.com Case Report PERSISTENT PATENT FORAMEN OVALE IN ADULT MALE Santhoshkumar N, Kunjumon PC and Anju Balaji More* Department of Anatomy, Sree Mookambika Institute of Medical Sciences, Kulasekharam, Tamilnadu, 629161, India Received for publication: February 17, 2014; Accepted: March 13, 2014 Abstract: In this case report, we want to present a persistent foramen ovale with length of 1.4 cm in an adult male cadaver approximately 60 years of age. The person had a heavy built up and appeared well nourished. The foramen ovale is a normal interatrial communication during fetal life. The persistence of this opening in the later life may go unnoticed if asymptomatic. But symptoms can begin in adult life due to pulmonary hypertension. It will become an added complication to any cardio-vascular disorder developing in later life. With no other anomalous findings in the heart, it appears that the foramen ovale was probe patent. There are five types of foramen ovale according to its location. The present finding belongs to type I that is patent foramen ovale of ostium secundum type. Echocardiogram, Electrocardiogram, Doppler image, Cardiac catheterization, Chest x-ray and MRI of the heart are the various imaging techniques which can detect this variance. Keywords: Atrium, Foramen ovale (Patent oval foramen), Fossa ovalis (Oval fossa). INTRODUCTION An atrial septal defect (ASD) is an opening in made available for the purpose of dissection under the interatrial septum. It allows oxygen rich blood in Anatomy Act. left atrium to mix with oxygen-poor blood in right atrium. -
Primitive Blood Circulation. • Heart Development (Dev. of Heart Tube, Septa and Valves) • Aortal Arches and Their Derivatives
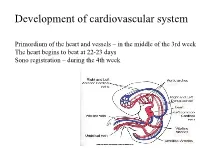
Development of cardiovascular system Primordium of the heart and vessels – in the middle of the 3rd week The heart begins to beat at 22-23 days Sono registration – during the 4th week • Primitive blood circulation. • Heart development (dev. of heart tube, septa and valves) • Aortal arches and their derivatives. • Fetal blood circulation. • Cardiovascular system malformations. Vessels development: (from week 3) hemangiogenesis - blood islands (insulae sanguinae) DAY 15 – 16 in extraembryonic mesoderm of - yolk sac (vasa omphalomesenterica /vitellina/), - connecting stalk and placenta (vasa umbilicalia) DAY 17 – 18 in mesenchyme of embryo Groups of angiogenic cells in mesenchyma ectoderm Blood islet mesenchyme angioblasts endoderm hemoblasts primitive erythrocytes primitive endothelium Differentiation of mesenchymal cells angiogenic cells: - angioblasts endothelium (at the periphery of blood islets) - hemoblasts primitive erythrocytes (in the center of blood islets) angiogenic cells form a "horseshoe-shaped" space between somatic and splanchnic layer of mesoderm = pericardial cavity. Two endothelial tubes arrise in splanchnic mesoderm. The ventral portion with tubes forms the cardiogenic area two heart tubes, while the lateral portions form the dorsal aortae. Cardiogenic region just cranial to the prechordal plate. Fusion of heart tubes mesocardium dorsale diferentiation of heart wall: endocardium ● heart jelly epimyocardium Vitelline, umbilical and intraembryonic vessels fuse together and form the primitive blood circulation ( fetal blood circulation!) Pericardial cavity Cor tubulare simplex Septum transversum branchial arteries 1-6 Right Leftt Desc.aorta Ventral wiew Truncus arteriosus Asc.aorta Sinus venosus right horn degenerate Saccus aorticus Vessels v. cardinalis ant. sin. + v. cardinalis com.sin. cor tubulare Yolk sac v. cardinalis post. sin. aa.omphalomesentericae a. mesenterica sin. -

The Sinus Venosus Typeof Interatrial Septal Defect*
Thorax: first published as 10.1136/thx.13.1.12 on 1 March 1958. Downloaded from Thorax (I9%8), 13, 12. THE SINUS VENOSUS TYPE OF INTERATRIAL SEPTAL DEFECT* BY H. R. S. HARLEY Cardiff (RECEIVED FOR PUBLICATION DECEMBER 30, 1957) Defects of the interatrial septum, other than namely, (1) it lies above and independent of valvular patency of the foramen ovale, are often the fossa ovalis; (2) its margin is incomplete, classified into ostium primum and ostium secun- being absent superiorly and incomplete pos- dum varieties. The relationship of the former type teriorly; and (3) it is associated with anomalous to abnormal development of the atrioventricular drainage of the right superior, and sometimes of canal has been stressed by several workers, includ- the right middle or inferior, pulmonary vein. This ing Rogers and Edwards (1948), Wakai and type of defect is illustrated in Fig. 1 (after Lewis Edwards (1956), Wakai, Swan, and Wood (1956), et al., 1955) and Fig. 2 (after Geddes, 1912). In Brandenburg and DuShane (1956), Toscano- the case reported by Ross (1956), who kindly per- Barbosa, Brandenburg, and Burchell (1956), and mitted me to see the heart, the interatrial Cooley and Kirklin (1956). These workers prefer communication was described as ". lying the term "persistent common within the orifice of atrioventricular the superior vena cava in itscopyright. canal " to "persistent ostium primum." medial wall opposite the mouths of the anomalous In addition to the above types of interatrial pulmonary veins." Ross goes on to say: "On septal defect there is a third variety, which was casual inspection of the interior of the left atrium, described as long ago as 1868 by Wagstaffe, but the defect was not visible unless a search was made which has come into prominence only since the within the superior caval orifice." The relation- http://thorax.bmj.com/ introduction of surgical repair of interatrial ship of the defect to the orifice of the superior communications under direct vision. -

THE CARDIOVASCULAR SYSTEM the Picture Shows the Tranverse Section of the Embryo Demonstrating the Formation of the Angioblastic Cords
EMBRYOLOGY: THE CARDIOVASCULAR SYSTEM The picture shows the tranverse section of the embryo demonstrating the formation of the angioblastic cords . In which region do these cords develop? The picture shows the lateral folding of the embryo and the fusion of the endocardial heart tubes . What is the significance of this folding? This picture shows the formation of cardiac loop . What are the five dilatations which form on the primordial heart tube? . What results in the bending of the heart tube? The picture shows the structure of a primordial heart . Give the three pairs of veins which are received by the sinus nenosus. The picture shows blood circulation through a primordial heart . Describe the circulation of blood through the primordial heart. The picture shows the formation of endocardial cushions . What are endocardial cushions and what is their significance? The picture shows the septation of the atrium in the primordial heart . Give the two septa which are responsible for the formation of the interatrial septa. What results in the perforations denoted by the red arrows? . What results in the formation of foramen primum and foramen secundum? . What is its significance? . What result in the formation of foramen ovale? What is the significance of this foramen? . What structure does formen ovale forms in the adult? The diagram shows the division of the sinus venosus into the left and right horns . Which structure is responsible for this division? . What are the derivatives/remnants of the left horn of the sinus venosus? . What is the fate of the right horn of the sinus venosus? The picture shows the absorption of the pulmonary vein into the left atrium . -

Human Embryologyembryology
HUMANHUMAN EMBRYOLOGYEMBRYOLOGY Department of Histology and Embryology Jilin University ChapterChapter 22 GeneralGeneral EmbryologyEmbryology DevelopmentDevelopment inin FetalFetal PeriodPeriod 8.1 Characteristics of Fetal Period 210 days, from week 9 to delivery. characteristics: maturation of tissues and organs rapid growth of the body During 3-5 month, fetal growth in length is 5cm/M. In last 2 month, weight increases in 700g/M. relative slowdown in growth of the head compared with the rest of the body 8.2 Fetal AGE Fertilization age lasts 266 days, from the moment of fertilization to the day when the fetal is delivered. menstrual age last 280 days, from the first day of the last menstruation before pregnancy to the day when the fetal is delivered. The formula of expected date of delivery: year +1, month -3, day+7. ChapterChapter 22 GeneralGeneral EmbryologyEmbryology FetalFetal membranesmembranes andand placentaplacenta Villous chorion placenta Decidua basalis Umbilical cord Afterbirth/ secundines Fusion of amnion, smooth chorion, Fetal decidua capsularis, membrane decidua parietalis 9.1 Fetal Membranes TheThe fetalfetal membranemembrane includesincludes chorionchorion,, amnion,amnion, yolkyolk sac,sac, allantoisallantois andand umbilicalumbilical cord,cord, originatingoriginating fromfrom blastula.blastula. TheyThey havehave functionsfunctions ofof protection,protection, nutrition,nutrition, respiration,respiration, excretion,excretion, andand producingproducing hormonehormone toto maintainmaintain thethe pregnancy.pregnancy. delivery 1) Chorion: villous and smooth chorion Villus chorionic plate primary villus trophoblast secondary villus extraembryonic tertiary villus mesoderm stem villus Amnion free villus decidua parietalis Free/termin al villus Stem/ancho chorion ring villus Villous chorion Smooth chorion Amniotic cavity Extraembyonic cavity disappears gradually; Amnion is added into chorionic plate; Villous and smooth chorion is formed. -

Study of Morphological Characteristics of Fossa Ovalis and Its Clinical Importance - a Cadaveric Study Dr
Scholars International Journal of Anatomy and Physiology Abbreviated Key Title: Sch Int J Anat Physiol ISSN 2616-8618 (Print) |ISSN 2617-345X (Online) Scholars Middle East Publishers, Dubai, United Arab Emirates Journal homepage: http://saudijournals.com/sijap/ Original Research Article Study of Morphological Characteristics of Fossa Ovalis and Its Clinical Importance - A Cadaveric Study Dr. Ashita Kaore1, Dr. Ashish Kamdi2*, Dr. N. Y. Kamdi3 1Assistant Professor, DepartmentofAnatomy, Government Medical College, Nagpur, Maharashtra, India 2Assistant Professor, Department of Anatomy, Government Medical College, Chhindwara, Madhya Pradesh, India 3Professor and Head, Department of Anatomy, Government Medical College, Nagpur Maharashtra, India *Corresponding author: Dr. Ashish Kamdi | Received: 02.03.2019 | Accepted: 05.03.2019 | Published: 30.03.2019 DOI:10.21276/sijap.2019.2.3.2 Abstract Transseptal access from right atrium to left atrium through the fossa ovalis using transseptal puncture and patent fossa ovalis repair are widely used cardiac techniques. These techniques require through knowledge of the cardiac anatomy especially of the fossa ovalis .Evaluation of the various morphological parameters of the fossa ovalis forms an important prerequisite before undertaking any surgical procedure in this region. This study was conducted on 60 cadaveric hearts from the department of Anatomy, Government medical college, Nagpur. The right atrium was opened and the fossa ovalis was studied for its shape, size, floor and the prominence and extent of the limbus fossa ovalis was noted. The fossa ovalis was observed for the presence of any patent foramen ovale or probe patency. In majority of the cases the shape of fossa ovalis was found to be oval 66.7% cases, the average craniocaudal diameter was found to be 15.03mm, and average anteroposterior diameter was found to be 14.44mm.