Kansas Resource Guide for Families with Infants and Toddlers Who Are
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
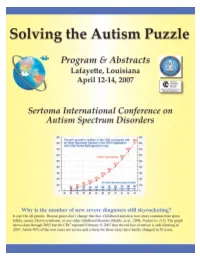
Solving the Autism Puzzle
Contents Foreword .............................. 4 Saturday (Schedule) .................... 18 Acknowledgments by Sertoma . 5 Poster Session 1: Friday 9:30 am . 20 Purpose of Autism07 .................... 6 Poster Session 2: Friday 3:00 pm . 21 Continuing Education Credit . 9 Poster Session 3: Saturday 9:30 am . 22 Thursday (Schedule).................... 11 Exhibitors............................. 25 Downstairs Floor Plan of the Cajundome Partners............................... 25 Convention Center .................. 11 Advertisers............................ 25 Upstairs floor plan for the Cajundome Planning & Organizing Committee . 25 Convention Center .................. 12 Index of Names & Companies . 26 Friday (Schedule) ..................... 13 Copyright © of this Program for Autism07 by the Sertoma Club of Lafayette 2007 Foreword The autism puzzle is about it? This conference addresses that critical question among the most troubling along with questions about the diagnosis and treatment of of today’s world. Severe autism and related disorders. Autism07 has received the autism robs parent and highest possible rating for continuing education from the child of a normal relation American Medical Association. Qualified participants can with each other. Jon receive up to 13.25 AMA PRA Category 1 CreditsTM . Shestack, the producer of Continuing education is also available to dentists, nurses, Father of the Bride and behavior analysts, psychologists, hygienists, social other Hollywood motion workers, occupational therapists, teachers, and -

General Information Mission
LaSertoma International Manual – General Information The LaSertoma International emblem is a registered trademark of the organization and cannot be used for or by any other organization. Mission Statement To enhance the lives of all persons and to promote youth and education through public awareness as we strive to be “Leaders in Service to Mankind” LaSertoma International, 6545 Steitz Road, Powell, OH 43065 Phone: 1-866-701-1950 Email: [email protected] Contents HOW LASERTOMA IS ORGANIZED ................................................................................................................. 3 LASERTOMA INTERNATIONAL GEOGRAPHIC AREAS ..................................................................................... 4 HISTORY OF LASERTOMA INTERNATIONAL .................................................................................................. 5 FACTS ABOUT LASERTOMA INTERNATIONAL ............................................................................................... 6 LASERTOMA PIN AND COLORS ..................................................................................................................... 7 LASERTOMA SONG ........................................................................................................................................ 7 LASERTOMA PLEDGE TO ALL NATIONS ......................................................................................................... 7 OFFICIAL TOAST TO THE NATIONS ............................................................................................................... -

Resources Resources
RESOURCES RESOURCES Pediatric audiological Service ProviderS For Children with Hearing Loss In Central Ohio Columbus City Schools Phone: 614-365-5977 Huy Elementary/A. G. Bell Program FAX: 614-365-5491 Columbus Hearing Impaired Program (C.H.I.P.) TTY: 614-365-5977 1545 Huy Road Columbus, Ohio 43224 Website: Columbus.k12.oh.us/agbell Diagnostic Audiological Evaluation: Infants Screenings (Birth–12 Months) or OAE o ABR 0-6 7-23 24-36 (months) Hearing Aid Services: OAE or or ro o Hearing Aids ro Loaner Hearing Aids ABR o o o o Monitored Sedation o Medical/ENT Evaluation ASSR o o o Tympanometry o or ro ro FM technology in the classroom Cochlear Implant Services: (Check all that applies to your services) o Comprehensive Cochlear Implant Program – Medical team; ENT Cochlear Implant, Surgeon, CI Coordinator, Audiologist, Speech & Language Pathologist, Psychologist, Social Worker, Occupational Therapist, Physical Therapist o Cochlear Implant Candidacy Evaluation o ENT Cochlear Implant Surgeon ro Psychologist ro Audiologist ro Speech & Language Pathologist ro Counselor ro Occupational Therapy ro Physical Therapy Financial: N/A – School System o Insurance Accepted o Medicaid Provider o BCMH (Ohio) Provider o Financial Assistance We are part of a school system and only serve those children enrolled in Columbus City Schools or in the Regional Infant Hearing Program (ages 0-3 years). If you have any questions or would like to discuss please call Rachel Nadal, Au.D. 614-365-5977. 154 Pediatric Audiological Service Providers Information in this section was provided by the individual service providers. If a provider is not listed, they did not submit information. -

Washburn Lawyer, V. 46, No. 1 (Fall 2008)
WASHBURN VOLUME 46, ISSUE 1 Lawyer FALL 2008 I Do Solemnly Swear… WashburnWashbu Law Alumni Sworn in to U.S. Supreme Court WASHBURN UNIVERSITY SCHOOL OF LAW ALUMNI MAGAZINE DEAN Thomas J. Romig Dear Alumni and Friends, Having completed my fi rst year as dean of Washburn University School of Law, it is apparent to me that the support of our alumni is critical to the success of Washburn Law. Alumni like you assist us by serving as speakers, adjunct professors, mentors, and judges for competition teams, as well as supporting our law school in numerous other ways. We had a great year, and this issue of the Washburn Lawyer will give you a brief recap of the programs Washburn Law has been involved with over the past 12 months, and an indication of what is to come. In October, we hosted our symposium on Humanizing Legal Education with nearly 100 law professors and deans from 40 law schools and three countries. In March, we had our American Bar Association/American Association of Law Schools accreditation site visit. Although we have not received the offi cial report yet, it was clear that the seven-member team was very impressed with our students, our programs, our dedicated staff and faculty, and our alumni they met. In short, they liked what they saw at Washburn University School of Law. In April, we hosted a very successful Writing to Win Symposium on Plain Language Jury Instructions. This symposium included judges, justices, and practitioners from across the country. Also in April, we had 29 alumni and two professors participate in a U.S. -

Methodist College Fayettevilla, North Carolina for Immediate Release
WECT Methodist College For immediate release Fayettevilla, North Carolina n.,- /-«u-»1-,- w v*~AJ._- ru - • •' i THE WILMINGTON MORNING STAR ; t i SCHOLARSHIP PRESENTATION—Yates Williams, center, Methodist College Junior from Wilmington, receives from Mrs, H. T. Fender, right, a scholarship for $100.00 established last year by the Lulie Biggs McKeithan Chapter of the United Daughters of the Confederacy while Mrs. Fender was president. Mrs. W. B. May, left, current president of/the chapter, observes the presentation which was made during the recent District Meeting of the U.D.C., which met at Methodist Collage. THE WILMINGTON MORNING STAR Methodist College For immediate release Fayetteville, North Carolina By: Charles K. McAdams, Director of Public Relations May 1, 1964 SCHOLARSHIP PRESENTATION--Yates Williams, center, Methodist College junior from Wilfaington, receives a $100.00 scholarship from the Lulie Biggs McKeithan Chapter of the United Daughters of the Confederacy of Fayetteville. Mrs. W, 8. May, left, president of the chapter, observes as Mrs. H. T. Pender, . past president, makes the presentation during the recant District Meeting of the U. D. C,, which was held on the Methodist College campus. Miss Williams, who is the daughter of Mrs. H. Richard , illians of 1512 Market Street, holds . a Merit Scholarship at Methodist College, served as treasurer of the freshman class, was a member of the committee which drew up the Student Government Constitution, and is currently the house manager of the Women's Residence Hall. 4, *v «•—. Methodist Cot lose For Release Tuesday, Hay 5, 1964 Fayettevilie, North Carolina By: Charles K« f-lcAdaos, Director of Public Relations May 4, 1964 The Music Depart niont of Methodist Co I logo will present a concert of chaobor ©uaic this evening at 8 o'clock in the Science Hall Auditorium. -

Thank You for Your Interest in Partnering with Us for the 2018 Service Club Leaders Conference
Thank you for your interest in partnering with us for the 2018 Service Club Leaders Conference. This unique event has one purpose – to provide an educational and knowledge network platform for those organizations that unite citizens to engage in service, advocacy, and the advancement of people. These organizations represent 4,000,000 members throughout the world who spend approximately USD12 billion dollars annually in meetings and events business, and conduct countless business service transactions in areas such as technology, finance, marketing, and more. The Service Club Leaders Conference (SCLC) is a not only a great vehicle to showcase your business or destination, it’s also a way to give back to these remarkable organizations that do so much to make our world a better place. The conference is a small and intimate event. Participation is exclusive to the top executive leaders from approximately 20 service organizations. Typically, 80-100 individuals attend representing the top levels of leadership, both volunteer and employed, who hold the most significant influence in purchasing decisions. This means your sponsorship dollars can be best leveraged at this event, compared to similar opportunities. Thank you for your interest in supporting this event, and for helping the service club organizations of the world train their leadership. If you are interested in learning more and to sign up for a sponsorship, please contact Gail Weller at [email protected]. On behalf of the entire SCLC Steering Committee, we look forward to working with you. Tracey Edwards CEO The National Exchange Club www.sclconference.org 1 SERVICE CLUB LEADERS CONFERENCE SPONSORSHIP PROSPECTUS Event November 15-17, 2018 at the Nugget Casino Resort, Reno, Nevada, USA. -

Republican Senate and House Members Who Will Decide If SC Should Expand Medicaid
Republican Senate and House members who will decide if SC should expand Medicaid ABBEVILLE Senate: William H. O’Dell, District 4, CEO, O'Dell Corporation, Inc. residing at 144 Devon Park, Greenwood; Deacon, Mt. Gallagher Baptist Church, 1977-81; Champion for Access to Healthcare, South Carolina Primary Healthcare Association, 2007 and 2009; Honorary Doctorate Degree from the Medical University of South Carolina, 2008; Home Phone (803) 252-0845, Office Phone (803) 212-6350, Home Phone (864) 943-0905, Business Phone (864) 861-2222 House: Craig A. Gagnon, District 11, Chiropractor residing at 161 Colony E., Abbeville; Deacon, First Baptist Church, Abbeville; Office Phone (803) 212-6934, Home (864) 459-4591, Bus. (864) 366-2024 Michael W. "Mike" Gambrell, District 7, Self-employed, M&R Enterprises, residing at 400 Filter Plant Rd., Honea Path; Clemson University, B.S., 1980; Office Phone (803) 734-2947, Home Phone (864) 369-0613, Business Phone (864) 844-3614 AIKEN Senate: A. Shane Massey, Attorney residing in Edgefield; Providence Baptist Church, Deacon and Sunday School Teacher; Office Phone (803) 212-6024, Home (803) 480-0419, Bus. (803) 649-6200 Thomas R. "Tom" Young, Jr., District 24, Attorney residing in Aiken; Member, St. John’s United Methodist Church; Office Phone (803) 212-6124, Home (803) 215-3631, Business (803) 649-0000 House: William M. "Bill" Hixon, District 83, President/Owner, Hixon Realty Co., President, Hixon Insurance Inc., residing at 770 Murrah Rd., N. Augusta; Member, First Baptist Church of North Augusta; Volunteer Fireman, North Augusta, 1973-; Office Phone (803) 212-6898, Home Phone (803) 278-0892, Business Phone (803) 279-8855 J. -

Sertoma's 4Th of July Celebration
SERTOMA’S 4TH OF JULY News Release Contact: Kevin King FOR IMMEDIATE RELEASE Volunteer, Sertoma’s 4th of July June 25, 2021 Personal Cell Phone: (704) 607-2111 (not for publication) SERTOMA’S 4TH OF JULY CELEBRATION 2021 PENSACOLA, FL. For the 32nd year, area Sertoma organizations are again coordinating and hosting the largest Fireworks display on the Gulf Coast over Pensacola Bay on Sunday, July 4th, 2021, at 9:00pm. This event has frequently been named one of the Southeast Tourism Society’s Top 20 Events for the month of July. The festivities are going to be different this year. While planning the event and unsure of how Covid would affect the day, it was decided to focus on the fireworks, making this year’s event not only the largest fireworks show on the Gulf Coast, but the largest ever! The celebration will return to the full day of festivities for 2022. Live Music on the Main Stage on Bayfront Parkway at Bartram Park: (Bayfront Parkway closed to traffic at 3:00pm) NOT QUITE FAB 4:30-6:00p The Beatles are back! Dance to the Fab Four’s music! STILL STANDING - A Tribute to Elton John 6:30-9:00p The Rocketman takes the stage! The festivities will culminate with the Largest Fireworks Show on the Gulf Coast launched at 9p over Pensacola Bay. Fireworks can be seen all along Bayfront Parkway so it will be easy to social distance. The fireworks show will be synchronized with music broadcast on CatCountry 98.7 radio. BRING YOUR RADIO. If you are accustomed to listening to radio on a device or app, please note that those have a built-in delay and the effect will not be the same, so, bring that radio! Thank you to our major sponsors: Escambia County, Cat Country 98.7, WEAR-ABC3, SKANSKA ~ MORE ~ Sertoma’s 4th of July Celebration Page 2 Sparks & Stars performance There will also be a free performance from the Pensacola Symphony Orchestra at the Hunter Amphitheater in Vince Whibbs Community Maritime Park is at 7:00 pm. -

Sertoma Club of Dayton Records
MS-106 The Sertoma Club of Dayton Records Collection Number: MS-106 Title: The Sertoma Club of Dayton Records Dates: 1925-1997 Creator: The Sertoma Club of Dayton Summary/Abstract: The Dayton Sertoma Club traces its origins to the founding of the first Cooperative Club of Kansas City, MO, founded on April 13, 1912, by Dr. George W. Smith. Smith, in conjunction with Dr. Charles E. Allen and newspaper editor W.R. Rowe, conceived the idea of another civic service club to aid society aside from the existing Rotary clubs. Smith believed that the Cooperative Club should not just utter principles toward mankind's betterment, it should selflessly take an active, non-political role in improving society. In 1950, it was determined that the name "Cooperative" was too confusing to the public, owing to the over usage of the term. The name "Sertoma" was adopted, an acronym for "Service to Mankind." The Sertoma records consist of material relating to the affairs of the Dayton Sertoma Club as well as its activities in conjunction with various regional Sertoma clubs and Sertoma International, the top governing body in the club hierarchy. These records contain information dealing with the Dayton Sertoma Club's finances, civic programs, annual events, and the political view of some members, notably past presidents William W. Owen and Rev. Harvey Hahn. Letters, memos, news clippings, pamphlets and other documents are present in the collection. Much of the material is of a mundane nature, although this does not preclude its significance to the researcher, as it gives a fair view of the nature of Sertoma, particularly the period 1954-1975. -

SERTOMA CLUB MANUAL Table of Contents
SERTOMA CLUB MANUAL Table of Contents Sertoma Information for clubs concerning their Sertoma relationship, including tax and insurance issues, protocol and parliamentary procedures Board & Officers Information for current and future leaders on the function, role, and how to fulfill the duties of the board and officers Committee Structure Information on how to establish effective committees, as well as a description of the roles and responsibilities of committees that make a club work, with a focus on the Big-3 – programs, sponsorships, membership Growth & Retention A guide for the membership committee or others working on membership development for the club and Sertoma Mission Activities A guide for Sertomans working on fulfilling our mission of service – includes information on all Sertoma sponsorship programs, how to support your national charity and local options for the club Fundraising A brief overview of key issues as your club develops and implements events or charitable solicitations in support of your sponsorship efforts Public/Media Relations A guide for the PR committee or others who work to increase the awareness of your club in the community Awards & Reports The guidelines and forms for all award programs and required reports to Sertoma Headquarters Governing Documents The Bylaws, Policy Statements and Procedures that determine how Sertoma is to function and make decisions Resources Glossary of Terms 1 2 SERTOMA Table of Contents Introduction to Sertoma We Are Sertoma Visiting Representatives Divisions & Meetings Sertoma Protocol & Ceremony Toast to All Sertoma Nations Sertoma Song Pledge to All Sertoma Nations Sertoma Prayer Meeting Room Layouts Sertoma Ceremonies Sertoma Convention Banquets U.S. -

Joan Phillips Waldron, Who Has Been Deaf Since Birth, Serves As Director of Development and Operations/Foundation Founder
Joan Phillips Waldron, who has been deaf since birth, serves as Director of Development and Operations/Foundation Founder Serves as the Director of Development and Operations as well as Founder of the Able Kids Foundation since 2005. The Foundation is a research-based, solutions-oriented nonprofit that partners with local, national, and international organizations, eliminating barriers and expanding opportunities for individuals with disabilities. Jo Waldron has more than 35 years of experience in executive level, corporate America and is an entrepreneur. She has also served as a liaison with several Presidential Administrations and numerous federal agencies and offices. This self-taught inventor driven by a lifelong quest to know what her children and family sounded like, along with wanting any sound to finally break the vacuum of silence, is an experienced inventor of accessible products for people with disabilities. Her journey has led her to create inventions that benefit all individuals and deliver the full and true impact of sound. Jo has created numerous job fairs; placing more than 6,000 Coloradoan’s with disabilities in the workforce. President Ronald Reagan selected Jo Waldron to receive America’s highest honor, “The President’s Trophy,” and she was appointed “Disabled American for the Nation,” representing the Presidents of the United States and all American’s with disabilities since 1987. Jo is an accomplished public speaker, having done more than 1,500 public speaking engagements nationwide. Since 1987 she has worked closely with several Presidential Administrations and their Cabinet Members, the U.S. Senate, and Congress as well as numerous other elected and Presidential appointed officials, including the Chairman’s and Commissioners of the Federal Communications Commission (FCC), the U.S. -
Agencies Listed May Have Certain Eligibility Criteria for Services and We Cannot Guarantee That All Agencies Will Be Able to Provide Assistance
Agencies listed may have certain eligibility criteria for services and we cannot guarantee that all agencies will be able to provide assistance. This is only a partial list of community agencies. We hope you will use this as a tool to assist you in locating needed resources. Community Resource Guide 06/06 Topic Page No. Child Care 3 Clothing 3 Counseling and Therapy 4 Dentists 5 Directions 8 Domestic Violence Resources 12 Education 13 Employment 15 Family Planning Services 17 Financial Assistance 19 Food 21 Furniture 23 Housing 23 Legal Resources 31 Medical Equipment and Supplies 32 Medical Needs and Medications 34 Miscellaneous 39 Substance Abuse 40 Transportation 41 Community Resource Guide 06/06 2 Child Care Resources, Inc. 704-376-6697 Subsidized Childcare Head Start 704-333-0203 Child development programs for low income children ages 3 and 4. YMCA 704-716-6200 After-school and summer camp Crisis Assistance Ministry 704-371-3001 Call for an appointment C.U.P. Ministry 704-331-4806 Call for an appointment Community Outreach Christian Ministry 704-333-4280 Call for an appointment Jackson Park Ministries 704-392-4981 Clothing closet for children Call for an appointment Berean Seventh Day Adventist Church 704-377-4741 Call for an appointment The Vestibule 704-336-5197 Call for an appointment Charlotte Pregnancy Care Center (Maternity & Baby) 704-372-5981 Assisting women who are clients, participate in our classes And earn vouchers for clothing. Charlotte-Mecklenburg Schools– Contact the principal of your school or your school’s PTA for assistance with purchasing school uniforms or clothing needs for a school age child through Operation School Bell.