Annual Analytical Report Fy 2017-2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Conflict Uganda
Health workers’ career paths, livelihoods and coping strategies in conflict and post- conflict Uganda Justine Namakula, Sophie Witter, Freddie Ssengooba and Sarah Ssali (2013) Acknowledgement This work was supported by UK Department for International Development (DFID) through the ReBUILD Consortium. The authors are deeply grateful for the financial support to carry out this work. This work draws on the life histories and experiences of health workers at different levels of the health system in Gulu, Amuru, Kitgum and Pader. We thank health workers for their patience, time, cooperation, insights and experiences shared during the research process without which this work would not have been possible. We also appreciate the contribution Ms. Adongo Jennifer, Mrs Sarah Auma Ssempebwa, Mr. Deo Tumusange, Mr. Tenywa Ronald, Ms. Resty Nakayima and Ms Eunice Kyomugisha for their hard work and contribution to the data collection and transcription of the interviews. We pray and hope that these research findings make a concrete contribution towards improving subsequent incentive interventions that can make a difference to the lives of health workers in Northern Uganda and other post conflict areas. 2 | P a g e Contents Acknowledgement ..................................................................................................................... 2 Contents ..................................................................................................................................... 3 Executive summary ................................................................................................................... -

Ministry of Health
UGANDA PROTECTORATE Annual Report of the MINISTRY OF HEALTH For the Year from 1st July, 1960 to 30th June, 1961 Published by Command of His Excellency the Governor CONTENTS Page I. ... ... General ... Review ... 1 Staff ... ... ... ... ... 3 ... ... Visitors ... ... ... 4 ... ... Finance ... ... ... 4 II. Vital ... ... Statistics ... ... 5 III. Public Health— A. General ... ... ... ... 7 B. Food and nutrition ... ... ... 7 C. Communicable diseases ... ... ... 8 (1) Arthropod-borne diseases ... ... 8 (2) Helminthic diseases ... ... ... 10 (3) Direct infections ... ... ... 11 D. Health education ... ... ... 16 E. ... Maternal and child welfare ... 17 F. School hygiene ... ... ... ... 18 G. Environmental hygiene ... ... ... 18 H. Health and welfare of employed persons ... 21 I. International and port hygiene ... ... 21 J. Health of prisoners ... ... ... 22 K. African local governments and municipalities 23 L. Relations with the Buganda Government ... 23 M. Statutory boards and committees ... ... 23 N. Registration of professional persons ... 24 IV. Curative Services— A. Hospitals ... ... ... ... 24 B. Rural medical and health services ... ... 31 C. Ambulances and transport ... ... 33 á UGANDA PROTECTORATE MINISTRY OF HEALTH Annual Report For the year from 1st July, 1960 to 30th June, 1961 I.—GENERAL REVIEW The last report for the Ministry of Health was for an 18-month period. This report, for the first time, coincides with the Government financial year. 2. From the financial point of view the year has again been one of considerable difficulty since, as a result of the Economy Commission Report, it was necessary to restrict the money available for recurrent expenditure to the same level as the previous year. Although an additional sum was available to cover normal increases in salaries, the general effect was that many economies had to in all be made grades of staff; some important vacancies could not be filled, and expansion was out of the question. -

Vote: 611 Agago District 2012/13 Quarter 2 Structure of Quarterly Performance Report Summary
Local Government Quarterly Performance Report Vote: 611 Agago District 2012/13 Quarter 2 Structure of Quarterly Performance Report Summary Quarterly Department Workplan Performance Cumulative Department Workplan Performance Location of Transfers to Lower Local Services and Capital Investments Submission checklist I hereby submit _________________________________________________________________________. This is in accordance with Paragraph 8 of the letter appointing me as an Accounting Officer for Vote:611 Agago District for FY 2012/13. I confirm that the information provided in this report represents the actual performance achieved by the Local Government for the period under review. Name and Signature: Chief Administrative Officer, Agago District Date: 6/6/2013 cc. The LCV Chairperson (District)/ The Mayor (Municipality) Page 1 Local Government Quarterly Performance Report Vote: 611 Agago District 2012/13 Quarter 2 Summary: Overview of Revenues and Expenditures Overall Revenue Performance Cumulative Receipts Performance Approved Budget Cumulative % Receipts Budget UShs 000's Received 1. Locally Raised Revenues 194,861 107,000 55% 2a. Discretionary Government Transfers 3,402,834 1,349,642 40% 2b. Conditional Government Transfers 13,006,953 6,266,062 48% 2c. Other Government Transfers 1,627,157 389,240 24% 3. Local Development Grant 934,301 443,793 48% 4. Donor Funding 789,893 160,548 20% Total Revenues 19,955,999 8,716,286 44% Overall Expenditure Performance Cumulative Releases and Expenditure Perfromance Approved Budget Cumulative Cumulative -

Agago District HRV Profile.Pdf
THE REPUBLIC OF UGANDA Agago District Hazard, Risk and Vulnerability Profi le 2016 Contents Maps ............................................................................................................................ ii Tables .......................................................................................................................... ii Acknowledgments ...................................................................................................... iii Executive Summary.................................................................................................... iv Acronyms.....................................................................................................................v Defi nition of Terms ..................................................................................................... vii Introduction ..................................................................................................................1 Objectives ................................................................................................................1 Methodology .............................................................................................................1 Overview of the Agago .............................................................................................4 Hazards .......................................................................................................................9 Hazard Risks .............................................................................................................13 -

AGAGO Q1.Pdf
Local Government Quarterly Performance Report Vote: 611 Agago District 2014/15 Quarter 1 Structure of Quarterly Performance Report Summary Quarterly Department Workplan Performance Cumulative Department Workplan Performance Location of Transfers to Lower Local Services and Capital Investments Submission checklist I hereby submit _________________________________________________________________________. This is in accordance with Paragraph 8 of the letter appointing me as an Accounting Officer for Vote:611 Agago District for FY 2014/15. I confirm that the information provided in this report represents the actual performance achieved by the Local Government for the period under review. Name and Signature: Chief Administrative Officer, Agago District Date: 16/03/2015 cc. The LCV Chairperson (District)/ The Mayor (Municipality) Page 1 Local Government Quarterly Performance Report Vote: 611 Agago District 2014/15 Quarter 1 Summary: Overview of Revenues and Expenditures Overall Revenue Performance Cumulative Receipts Performance Approved Budget Cumulative % Receipts Budget UShs 000's Received 1. Locally Raised Revenues 458,200 42,871 9% 2a. Discretionary Government Transfers 3,945,141 986,284 25% 2b. Conditional Government Transfers 14,961,741 3,712,616 25% 2c. Other Government Transfers 2,197,992 1,370,610 62% 3. Local Development Grant 848,714 212,179 25% 4. Donor Funding 806,000 56,000 7% Total Revenues 23,217,789 6,380,560 27% Overall Expenditure Performance Cumulative Releases and Expenditure Perfromance Approved Budget Cumulative Cumulative -

Dr. Ambrosoli Memorial Hospital, Uganda
Migration. Peace and development. New challenges and new faces for Cooperation V CONGRESS of the Italian University Network for Development Cooperation 14-15th of September 2017 | Milan STRATEGIC PLANNING PROCESS IN A GENERAL RURAL HOSPITAL: AN EXPERIENCE AT DR. AMBROSOLI MEMORIAL HOSPITAL, UGANDA Andrea Carlo Lonati°, Ilaria Polloni°, Filippo Ciantia§, Thomas Odong*, Mirella Pontello# ° Postgraduate School in Public Health, Department of Health Sciences, University of Milan § CEO Dr. Ambrosoli Memorial Hospital, Kalongo, Uganda * Institute for Reproductive Health, Georgetown University Field Office, Gulu, Uganda # Department of Health Sciences, University of Milan, Italy THE BACKGROUND Kalongo Town Council currently has a total estimated population of 11,077, with 87.27% of Agago District’s population (that amounts to 230,908) Agago District is one of the poorest areas of the country and a large proportion of the population is living in a condition of poverty . 35.2% of the population lives below the national poverty line, < 1$ per day (Poverty Status Report – November 2014) - against a national average poverty rate of 19.7% . 41.4% are insecure, with very low resilience to external factors (e.g. health issues). DR. AMBROSOLI MEMORIAL HOSPITAL: THE HOSPITAL AND HIS BACKGROUND DR. AMBROSOLI MEMORIAL HOSPITAL . Founded in 1957 by Fr. Dr. Giuseppe Ambrosoli . PNFP, general hospital and training school . Member of Catholic health facilities under the coordination of the UCMB . The owner is the Catholic Diocese of Gulu . The only hospital in Agago District heading the Agago Health SubDistrict. DR. AMBROSOLI MEMORIAL HOSPITAL: THE HOSPITAL AND HIS BACKGROUND DR. AMBROSOLI MEMORIAL HOSPITAL A general rural hospital with 267 bed capacity distributed through 5 wards: Medical, Surgical, TB, Maternity and Paediatric The third in the League Table amongst general hospitals (Annual Health Sector Performance Report 2015-16 by MoH) DR. -

Comboni's Holiness in His Followers
COMBONI’S HOLINESS IN HIS FOLLOWERS Fr. Lorenzo Carraro, MCCJ COMBONI’S HOLINESS IN HIS FOLLOWERS Fr. Lorenzo Carraro, MCCJ Manila, August 2018 1 TABLE OF CONTENTS Opening Essay: Comboni’s Holiness in his followers…………… pag. 3 Patient Vision: Archbishop Agostino Baroni…………………………….8 Blue Eyes: Bro. Vittorio Fanti……………………………………………..11 Fugitive for God: Sr. Lucia Careddu……………………… …………… 14 Double Impact: Fr. Fulvio Cristoforetti …………… ………………… 19 The Wars of a Man of Peace: Fr. Giuseppe Ambrosoli……………….. 24 Mission Accomplished: Bishop Cesare Mazzolari… ………………….29 Fr. Lele’s Legacy: Fr. Ezechiel Ramin………………………………… .. 35 Singing through Life: Bro. Bernard Pratt………………………………….39 Dom Franco’s Bicycle: Bishop Gianfranco Masserdotti… ……………..42 Lifeblood of Africa: Fr. Tarcisio Agostoni………………… …………48 Letters from the dead: Srs. Cesarina Borghesi & Federica Bettari…… …55 A Life for Ethiopia: Bishop Armido Gasparini…………………………….58 Note: The Opening Essay was written on the occasion of Bishop Comboni’s Canonization ((2003). The 13 profiles were published in World Mission or in Friends of the Missions Newsletter (Fr. Lorenzo Carraro, MCCJ). &&&&&& 2 COMBONI’S HOLINESS IN HIS FOLLOWERS Comboni’s canonization is a gift for each one of us, Comboni missionaries, and a challenge to understand the inner logic in this happening that God has prepared for us. What strikes me lately is the quality of witness of the sons and daughters of Comboni as it stands out from the profiles of the confreres and con-sisters who reach the end of their lives on earth and whom I have known. What follows is the presentation of one of them, but in the background of the call of for holiness and in connection with the example of Comboni himself. -

Using Life Histories to Explore Gendered Experiences of Conflict in Gulu District, Northern Uganda: Implications for Post-Conflict Health Reconstruction
South African Review of Sociology ISSN: 2152-8586 (Print) 2072-1978 (Online) Journal homepage: http://www.tandfonline.com/loi/rssr20 Using life histories to explore gendered experiences of conflict in Gulu District, northern Uganda: Implications for post-conflict health reconstruction Sarah N. Ssali & Sally Theobald To cite this article: Sarah N. Ssali & Sally Theobald (2016) Using life histories to explore gendered experiences of conflict in Gulu District, northern Uganda: Implications for post- conflict health reconstruction, South African Review of Sociology, 47:1, 81-98, DOI: 10.1080/21528586.2015.1132634 To link to this article: https://doi.org/10.1080/21528586.2015.1132634 © 2016 The Author(s). Published by Unisa Published online: 24 Mar 2016. Press and Informa UK Limited, trading as Taylor & Francis Group Submit your article to this journal Article views: 145 View related articles View Crossmark data Citing articles: 8 View citing articles Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=rssr20 USING LIFE HISTORIES TO EXPLORE GENDERED EXPERIENCES OF CONFLICT IN GULU DISTRICT, NORTHERN UGANDA: IMPLICATIONS FOR POST-CONFLICT HEALTH RECONSTRUCTION Sarah N. Ssali School of Women and Gender Studies Makerere University [email protected]; [email protected] Sally Theobald Department of International Public Health Liverpool School of Tropical Medicine [email protected] ABSTRACT The dearth of knowledge about what life was like for different women and men, communities and institutions during conflict has caused many post-conflict developers to undertake reconstruction using standardised models that may not always reflect the realities of the affected populations. -

Behaviour Change for Improved Hygiene and Sanitation: Not Just a Household Affair!
Behaviour change for improved hygiene and sanitation: not just a household affair! There is common agreement in the WASH sector that household hygiene and sanitation in rural areas in developing countries is, first and foremost, the responsibility of the household. With the Community Led Total Sanitation (CLTS) approach, a stronger role of the community has been introduced in changing the hygiene and sanitation behaviour of the household members. The PILS1 (Performance Improvement through Learning in Sanitation) project in three districts in Northern Uganda2 has focused on strengthening the supporting role to communities of local government and Civil Society Organisations (CSOs) by facilitating district- and sub-county-based learning and action research. Working in a post-war environment, PILS has shown that improvements in coordination and the introduction of a learning process among the decentralised stakeholders can contribute to innovation, better financing and local solutions. The experiences with the PILS project can help the development of hygiene and sanitation policies and their implementation in Uganda. Author: René van Lieshout, International Water and Sanitation centre (IRC), March 2012 Peer review: Valérie Bey, IRC The hygiene and sanitation context in Northern Uganda After more than 20 years of insurgencies, Northern Uganda is going through a transition phase from heavily externally-supported humanitarian aid to peace and sustainable development. Most Internally Displaced People (IDPs) have left the camps and are now either in transition camps or have returned to their villages. At the same time, many humanitarian NGOs and UN agencies have left Northern Uganda and have substantially reduced their programmes there. The returnees are faced with many challenges to develop their livelihoods and get to grips with the routines of daily life. -
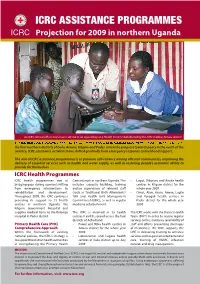
ICRC ASSISTANCE PROGRAMMES Projection for 2009 in Northern Uganda Pascal Jequier /ICRC Pascal
ICRC ASSISTANCE PROGRAMMES Projection for 2009 in northern Uganda Pascal Jequier /ICRC Pascal An ICRC clinical offi cer and a nurse attend to an injured boy at a Health Centre rehabilitated by the ICRC in Bibia, Amuru district the four northern districts of Gulu, Amuru, Kitgum and Pader. Given the progress towards peace in the north of the country, ICRC assistance activities have shifted gradually from emergency response to livelihood support. The aim of ICRC assistance programmes is to promote self-reliance among aff ected communities, improving the delivery of essential services such as health and water supply, as well as restoring people’s economic ability to provide for themselves. ICRC Health Programmes ICRC health programmes aim at Care network in northern Uganda. This • Lagot, Dibolyec and Anaka health bridging gaps during a period shifting includes capacity building, training centres in Kitgum district for the from emergency interventions to and/or supervision of relevant staff whole year 2009 rehabilitation and development. (such as Traditional Birth Attendants/ • Omot, Alim, Arum, Awere, Lagile Throughout 2009, the ICRC continues TBA and Health Unit Management and Porogali health centres in providing its support to 13 health Committees/HUMC), as well as regular Pader district for the whole year centres in northern Uganda, the medicine refurbishment. 2009 Kitgum Government Hospital and supplies medical items to the Kalongo The ICRC is involved in 13 health The ICRC works with the District Health Hospital in Pader district. centres II and III, spread across the four Team (DHT) in order to secure regular districts of Acholiland: services to the structures (availability of Primary Health Care (PHC) • Pawel and Bibia health centres in staff and eff orts preventing shortages Comprehensive Approach Amuru district for the whole year of medicines). -

Kitgum District Hazard, Risk, and Vulnerability Profi Le
Kitgum District Hazard, Risk, and Vulnerability Profi le 2016 Kitgum District Hazard, Risk, and Vulnerability Profi le i Contents List of Figures ............................................................................................................. iv List of Tables ............................................................................................................... iv Acronyms.....................................................................................................................v Acknowledgment ........................................................................................................ vi Executive Summary................................................................................................... vii Defi nition of Terms ...................................................................................................... ix Introduction ..................................................................................................................1 Objectives ....................................................................................................................1 Methodology ................................................................................................................1 Overview of the District................................................................................................4 Location and Administration ........................................................................................4 Climate ........................................................................................................................6 -

UG-Plan-61 A3 21Sep10 Uganda Planning Map.Mxd
IMU, UNOCHA Uganda http://www.ugandaclusters.ug http://ochaonline.un.org Uganda Overview " , $ !!#') #*# %! &# ### * + ! # " ! $," ! ! $) ) ! " !, ! , !'$ !!"! % ! Legend ! ! #$ # '),- Lakes/Water Body (! + !)!)# !! " )% ( ! Towns ! !$ " ! ### " Motorable Road '&#*! -# # " ) #+ ! '+$ " District Boundary '!(! #*! #%+ %$! " !%+#') National Boundary )!/ ! $! $ " ! Landuse Type $*!' #')# %$$! ##%# " !(! )! !!&$ $ ! '!!($$($$ Forest Reserve ! " ! ! !+! !$ # ##$ ! , "" !$' $ Game Reserve ! #%!! $" ! $ $ ')#! +++ $ $! %! %$ "#$ ! National Park ) &++' " + +! '!!#')#%! !("#&! $"! *+' + ! &# )" ) " $ (!%%$! Rangeland " ! "! $#'# ! *!'&!'-$ '!!++ $ !%$# !! ! $ " $ '### ) " & !%+ $"" $ !*')! & ) $!!%+ ! %$ ! Data Sources: !%+,! !'!.&! '! ! $#)! $! %&+# " ' $)*# $!! Admin Boundaries - UBOS 2010 %! & ! ! ### % $)!')! Admin Centres - UBOS 2002/2006 ., " *+',#,# !! Road Network - FAO, UNOCHA !!#%+ ! ! " $! ,$',! +' + )$$ *+)+)&! & $*!'! !& $! & " ! (!%! $&+ ! &+')+ ! &!$# Map Disclaimer: )# ! " ! !%! !++ The boundaries and names $ ($)$ * $" shown and the designations #'# + !%+ used on this map do not imply $!' ! !*)+ !%') official endorsement or " # !'$ $ ) acceptance by the $"! %*!' # ' + United Nations. !+++ '& '$$! " '! $*!')# ! '" %&+')# " "+'*$ ! !!! This map is a work in progress. ) !!! !%!')!%! Please contact the IMU/Ocha $$')# $## ! as soon as possible with any )) $ corrections.