The Dead Are Soon Forgotten, but Man Left Mutilated, Man Paralyzed, Is a Source of Guilt and Shame to Everyone Who Regards Him
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Polio Vaccine Safety Paul Meier's Role in the Discovery And
www.barkerstats.com Polio Vaccine the cutter incident October 1, 2020 Downloaded from www.barkerstats.com/PDFs/Meier/Meier-Cutter-Incident-History.pdf Polio Vaccine Safety Paul Meier’s Role in the Discovery and Evaluation of The Cutter Incident Professor Chris Barker, Ph.D. Adjunct Associate Professor of Biostatistics, UIC SPH. www.barkerstats.com Page 1 of 11 www.barkerstats.com Polio Vaccine the cutter incident October 1, 2020 Contents Background .................................................................................................................................................................................................................... 3 Brief Polio Vaccine Overview ......................................................................................................................................................................................... 3 Polio Vaccine Manufacturing Data Suppression ............................................................................................................................................................ 4 Biological Disaster? How Serious was the vaccine manufacturing problem? ............................................................................................................... 5 Near Elimination of Vaccine development by lawsuits ................................................................................................................................................. 6 Meier’s evaluation of the safety recommendations following The Cutter Incident .................................................................................................... -
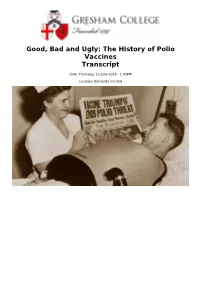
Good, Bad and Ugly: the History of Polio Vaccines Transcript
Good, Bad and Ugly: The History of Polio Vaccines Transcript Date: Thursday, 12 June 2014 - 1:00PM Location: Barnard's Inn Hall 12 June 2014 Good, Bad and Ugly: The History of Polio Vaccines Professor Gareth Williams The main villain of the piece is the poliovirus, one of the smallest and simplest viruses. It is usually spread by the faecal-oral route (dirty fingers!) and in most cases is confined to the gut. As travels down the intestine, it induces antibodies (immunity) against itself, which will protect the person against future attacks by the virus. In about 1% of cases, the virus floods into the bloodstream and infects the nerve cells in the spinal cord which drive the muscles. This causes the characteristic paralysis, which can affect one or more limbs and/or the muscles of respiration – in which case artificial ventilation (e.g. with the iron lung) may be needed to keep the patient breathing and alive. Polio originally caused sporadic clusters of paralysis, especially in children. For some reason, this pattern changed during the late 19th century into explosive epidemics which swept through many countries each summer. The first major outbreak, on the East Coast of the USA in the summer of 1916, caused 25,000 cases of paralysis and 6,000 deaths. Draconian public health measures were powerless to prevent the spread of polio, resulting in widespread panic across America. Each year, panic resurfaced as the polio season approached, with the wealthy leaving towns and cities in droves. During the early 1950s, Americans feared polio almost as much as the atom bomb. -

Jonas Salk at the National Press Club, April 12, 1965
Jonas Salk at the National Press Club, April 12, 1965 Jonas Salk, May 1962. A.F.P. – D.P.A. Photos. National Press Club Archives On the tenth anniversary of the licensing of the polio vaccine he developed, Dr. Jonas E. Salk (1914-1995) visited Washington to accept a joint congressional resolution that hailed the vaccine as “one of the most significant medical achievements of our time.” At the White House, President Johnson offered Salk his congratulations. The day also marked the twentieth anniversary of the death of former President Franklin D. Roosevelt, who, having suffered from paralytic polio since 1921, had established the foundation that funded Salk’s efforts. Following his meetings with Congress and the President, Salk gave a talk and answered reporters’ questions at a National Press Club luncheon. In the title of its lead editorial ten years earlier celebrating the successful testing of the new vaccine, the New York Times proclaimed the “Dawn of a New Medical Day.” Testing of the vaccine, like the funding for its development, had engaged the participation of millions of ordinary American citizens. Through March of Dimes campaigns, hundreds of thousands of volunteers went door-to-door raising $41 million in 1952 alone from average donations of 27 cents. The tests involved 1.8 million school children, 200,000 volunteers, 64,000 teachers, and 60,000 physicians, nurses, and health officials, making it the largest clinical trial in history. Interpreting the jubilant 1 reaction to news that the vaccine had been proven safe and effective, the Times commented, “Gone are the old helplessness, the fear of an invisible enemy, the frustration of physicians.” Poliomyelitis, also known as infantile paralysis, is an extremely contagious viral infection caused by any of three types of poliovirus. -
Our Global Initiative
2021 OUR GLOBAL INITIATIVE AN ASSESSMENT OF COVID-19 & THE FAILED GLOBAL HEALTH POLICIES OF THE WHO OUR GLOBAL INITIATIVE In early 2020, Australia, and indeed the world, collapsed into a lockdown prompted by the World Health Organisation in its designation of Covid 19 as a pandemic. What began as “2 weeks to flatten the curve” quickly morphed into a year of intermittent lockdowns, a loss of freedoms and liberties, the decimations of SME’s, irrational restrictions, unadulterated government surveillance, an endless state of emergencies, the rise of the police state a totalitarian grand stride towards medical fascism and a technocratic dictatorship as well as the end of civil society as we know it. What happened? How did we get here? Where are we going? What does this world of the “New Normal” hold for not only Australia, but the human civilisation? How do we navigate this reality and not only survive but thrive? The Global Health Organisation, in collaboration with the Australian Patriots Alliance, the World Solutions Foundation, the QuantumPrism Foundation, Ikighais Pty Ltd and other concerned institutions (the Initiative) have commissioned this report in effort to gain an insight into what is going on; the why, they how and the WHO! Further, the report will offer solutions to current concerns, as well as ways for interested parties to position themselves to thrive and win in the new society bound to emerge from the ashes of this dying world. 2 TIPS TO HELP READ THIS REPORT This report contains a lot of information and we appreciate SUMMARY POINTS that time is scarce. -

The March of Dimes and Polio: Lessons in Vaccine Advocacy for Health Educators
Feature Article The March of Dimes and Polio: Lessons in Vaccine Advocacy for Health Educators Dawn Larsen ABSTRACT The polio vaccine became available in 1955, due almost entirely to the efforts of the March of Dimes. In 1921, Franklin Roosevelt gave a public face to polio and mounted a campaign to prevent it, establishing the National Foundation for Infantile Paralysis in 1938. During the Depression, U.S. citizens were asked to contribute one dime. Entertainer Eddie Cantor suggested the name the March of Dimes, paraphrasing the popular newsreel “The March of Time.” Jonas Salk advocated a killed-virus vaccine while Albert Sabin proposed a live-virus vaccine. Both competed for both recognition and funding from the March of Dimes. In 1955 Salk’s vaccine was adopted, nationwide vaccination programs were implemented, and polio rates dropped by 80 percent. In 1961, Sabin’s vaccine, endorsed by the American Medical Association, became the vaccine of choice. The World Health Assembly advocated polio eradication by the year 2000. By 2004 eradication efforts were threatened by allegations linking vaccines to chronic diseases. Immunization dropped and polio resurfaced in the U.S., Australia, Africa and Russia. Research linking vaccines to chronic disease was dis- credited, but vaccine opponents remain active. Health educators are well positioned to mitigate damage caused by the anti-vaccine movement and address barriers to immunization efforts. Larsen D. The March of Dimes and polio: lessons in vaccine advocacy for health educators. Am J Health Educ. 2012;43(1):47-54. Submitted May 30, 2011. Accepted July 9, 2011. In 2008, The March of Dimes cel- prenatal health promotion programs, and of the virus that has been ranked second ebrated its 70th anniversary. -

Polio in Italy
Polio in Italy Bernardino Fantini (*) (*) Institute for the History of Medicine and Health, University of Geneva. [email protected] Dynamis Fecha de recepción: 23 de enero de 2012 [0211-9536] 2012; 32 (2): 329-359 Fecha de aceptación: 5 de marzo de 2012 SUMMARY: 1.—Introduction. 2.—The epidemiology of polio in Italy. 3.—The social and scientific reactions to the polio epidemics. 4.—The 1958 epidemics. 5.—The different actors. 6.—The vaccination campaign and the elimination of the disease. 7.—Changing attitudes in patients and the public. 8.—The origins of patient’s associations. 9.—The post-epidemic problems. The post-polio syndrome. 10.—Concluding remarks. ABSTRACT: The history of polio in Italy is relatively short because the particular social and demographic history of the country has actually compressed the most dramatic history of the polio epidemic into only 40 years, from the first severe epidemic just before World War II to the early 1980s, when the epidemic vanished thanks to an effective and country-wide vaccination campaign. The epidemic, however, had a formidable impact on medicine, public health, social attitudes and culture. An analysis of this case study can illustrate the impact of an epidemic of a severe disease on individual and collective life, and at the same time the efficacy of public health measures against it, and the importance of the social structure, state and private, in coping with the consequences of the epidemics. In this period, the attitude towards the handicapped changed from stigma and isolation to social integration, thanks especially to the changes in health legislation, social action and the initiatives of the patient’ associations. -

Chronological Introduction of Types of Vaccine Products That Are Still Licensed in the United States
Appendix 2.3 CHRONOLOGICAL INTRODUCTION OF TYPES OF VACCINE PRODUCTS THAT ARE STILL LICENSED IN THE UNITED STATES The year of introduction of each of 49 of the 51 shown in table 2.3B, American pharmaceutical com- types of vaccine prducts currently licensed in the panies were issued 37 (89 percent) of the original United States, alolng with the manufacturing estab- licenses for these 42 products. New or improved lishment with the oldest license still in effect for each types of products that are currently licensed have product, is shown in table 2.3 A.] For 42 (86 percent) been introduced at a fairly consistent rate of three to of these 49 products, the establishment that received seven products per each 5-year interval since 1940.2 the original product license still holds this license. As Ten of the currently licensed products were licensed before 1940. Table 2.3A—Chronological Introduction of Types of Vaccine Products Still Licensed in the United States Year Type of vaccine product Establishment with oldest product license still in effecta 1903 Dlphtherla antitoxin Massachusetts Public Health Biologic Laboratories (191 7) 1907 Tetanus antitoxin Parke. Davis and Company (191 5) 1914 Pertussis vaccine Lederle Laboratories Typhoid vaccine Massachusetts Public Health Biologic Laboratories (191 7) Rabies vaccine . Eli Lilly and Company* 1917 Cholera vaccine Eli Lilly and Company* 1926 Diphtheria toxoid Parke, Davis and Company (1927) 1933 Staphylococcus toxoid Lederle Laboratories* Tetanus toxoid Merck Sharp and Dohme 1941 Typhus vaccine Eli Lilly and Company 1942 Plague vaccine .., . Cutter Laboratories* Rocky Mountain Spotted Fever vaccine. Lederle Laboratories* 1945 InfIuenza virus vaccine Lederle Laboratories Merck Sharp and Dohme Parke, Davis and Company * 1946 Parke, Davis and Company ● 1947 Parke, Davis and Company (1949) 1948 Parke, Davis and Company (1952) Parke. -

Poliomyelitis and the Neurologists: the View from England, 1896-1966
Poliomyelitis and the Neurologists: The View from England, 1896-1966 ANNE HARDY The American vs. the European Experience In 1907, following one of the earliest poliomyelitis outbreaks in New York City, the New York Neurological Society set up a poliomyelitis committee with a view to studying and illuminating the behavior of this newly epi- demic disease.' The neurologists7 interest in polio was of long standing, dating from the orthopedic surgeon Jacob von Heine's conclusion, in 1860, that the symptoms of infant paralysis pointed to "an affection of the central nervous system, namely the spinal cord."* Ten years later, Heine7s deduction had been confirmed by the researches ofJean-Martin Charcot (1825-93), who demonstrated the destruction of the grey matter of the anterior horns of the spinal cord (within which the motor impulses arise and are transmitted) in cases of infant paralysk3 This demonstration of the pathology of the disease placed it firmly within the concerns of neurol- ogy, where it remained until polio arrived as a major epidemic problem. In America, according to John R. Paul, the New York Neurological Society's committee marked "almost the last time that neurologists as a professional body were to assume a position of dominance with respect This article was written in memory of Elizabeth Mary Margaret Hardy (1922-52). I am grateful to Michael Neve, who gave me the occasion to write it; to Bill Bynum, for advice; to Irvine Loudon, for generously supplying the graph; and to Tony Gould, Andrew Wear, and the Bulletin's anonymous referees, for constructive criticism. 1.John R. -

The Academic Model for the Prevention and Treatment of HIV
C A S E S I N G L O B A L H E A L T H D ELIVERY GHD-045 JULY 2021 Building the Supply Chain for COVID-19 Vaccines Mid-April 2020 saw a rapid escalation of the COVID-19 pandemic. In the four months after December 2019, when the novel coronavirus that causes COVID-19 was first detected in Wuhan, China, the virus had infected several million people globally, with more than a hundred thousand confirmed deaths (see Exhibit 1 for daily confirmed deaths by country). China and Italy experienced major outbreaks early and saw hospitals flooded with COVID-19 patients, causing major shortages of vital intensive-care materials. To forestall the overburdening of health care resources, more than a dozen major countries imposed strict lockdowns to slow the spread of the disease, or “flatten the curve” (see Exhibit 2 for a map of government responses). Government lockdowns disrupted supply and demand in vital industries including retail, tourism, manufacturing, and services, crippling the global economy. As the massive scale of the crisis became apparent, financial markets began to collapse during February, leading some experts to warn of a potential next Great Depression and governments to announce unprecedented rescue packages to contain the destructive economic impact of the crisis. As governments navigated trade-offs between economic and public health outcomes, a global race had begun for the rapid discovery, production, and distribution of a safe and effective vaccine. The organization of supply chains to manufacture, distribute, and administer a vaccine to a sufficient portion of the 7.6 billion world population to contain the disease, a concept termed “herd immunity,” posed significant challenges. -

Robert J. Desalvo Papers Business Combinations in the Cosmetic and Pharmaceutical Industries 1944
Robert J. DeSalvo Papers Business Combinations in the Cosmetic and Pharmaceutical Industries 1944 - 1990 Collection #107 Abstract Robert J. DeSalvo’s research focused on business combinations (acquisitions, mergers, and joint ventures in the cosmetic and pharmaceutical industries. This topic was the basis for his master’s thesis in pharmacy administration at the University of Pittsburgh and continued as a life-long interest. This collection consists of two series of notebooks that Dr. DeSalvo developed to record relevant business combinations. The first series records acquisitions, proposed acquisitions, mergers, and joint ventures for the period of 1944 –1990 in an alphabetical arrangement. The information on these entries is cumulative so that the history of an organization is collected in one place. The second series of notebooks is arranged in chronological blocks. The information is arranged alphabetically by the name of the acquirer. The name of the acquired (merged), type of combination (acquisition, proposed acquisition, joint venture) and the date is also provided. The information is cross-referenced between the two series so that the researcher can approach the information by the name of the parent company or chronologically. Dr. DeSalvo used this resource for many of his publications as well as his master’s thesis. A copy of these publications and his thesis make up the remainder of the collection. Donor Gift of Barbara DeSalvo, 2000 Biography Robert James DeSalvo was born on July 20, 1933 in Toledo, OH. He died on January 23, 1993 in Cincinnati, OH. DeSalvo graduated from high school in Toledo and attended pharmacy school at the University of Toledo where he received his B.S. -

Polio in Italy
Polio in Italy Bernardino Fantini (*) (*) Institute for the History of Medicine and Health, University of Geneva. [email protected] Dynamis Fecha de recepción: 23 de enero de 2012 [0211-9536] 2012; 32 (2): 329-359 Fecha de aceptación: 5 de marzo de 2012 SUMMARY: 1.—Introduction. 2.—The epidemiology of polio in Italy. 3.—The social and scientific reactions to the polio epidemics. 4.—The 1958 epidemics. 5.—The different actors. 6.—The vaccination campaign and the elimination of the disease. 7.—Changing attitudes in patients and the public. 8.—The origins of patient’s associations. 9.—The post-epidemic problems. The post-polio syndrome. 10.—Concluding remarks. ABSTRACT: The history of polio in Italy is relatively short because the particular social and demographic history of the country has actually compressed the most dramatic history of the polio epidemic into only 40 years, from the first severe epidemic just before World War II to the early 1980s, when the epidemic vanished thanks to an effective and country-wide vaccination campaign. The epidemic, however, had a formidable impact on medicine, public health, social attitudes and culture. An analysis of this case study can illustrate the impact of an epidemic of a severe disease on individual and collective life, and at the same time the efficacy of public health measures against it, and the importance of the social structure, state and private, in coping with the consequences of the epidemics. In this period, the attitude towards the handicapped changed from stigma and isolation to social integration, thanks especially to the changes in health legislation, social action and the initiatives of the patient’ associations. -
![[1] Vaccination Update Table of Contents: 1](https://docslib.b-cdn.net/cover/7215/1-vaccination-update-table-of-contents-1-3097215.webp)
[1] Vaccination Update Table of Contents: 1
EYE ON THE MARKET • MICHAEL CEMBALEST • J.P. MORGAN Last updated 9/23/2021 [1] Vaccination update Table of Contents: 1. US vaccination overview ................................................................................................................................2 2. Vaccination vs infection, mortality, hospitalization and 2020 Trump voting share ............................................3 3. “A pandemic of the unvaccinated” .................................................................................................................4 4. Population shares, vaccine efficacy and the amalgamation paradox ................................................................5 5. Vaccine efficacy tracker ..................................................................................................................................6 6. Vaccination vs previous COVID infection (acquired vs natural immunity) .........................................................7 7. Vaccine risk-benefit data ................................................................................................................................8 8. Variant prevalence by country ........................................................................................................................9 9. Delta variant facts and figures ........................................................................................................................9 10. Vaccine update by country and US state ......................................................................................................