Multiple Levels of Immunological Memory and Their Association with Vaccination
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Antibody-Dependent Cellular Cytotoxicity Riiia and Mediate Γ
Effector Memory αβ T Lymphocytes Can Express Fc γRIIIa and Mediate Antibody-Dependent Cellular Cytotoxicity This information is current as Béatrice Clémenceau, Régine Vivien, Mathilde Berthomé, of September 27, 2021. Nelly Robillard, Richard Garand, Géraldine Gallot, Solène Vollant and Henri Vié J Immunol 2008; 180:5327-5334; ; doi: 10.4049/jimmunol.180.8.5327 http://www.jimmunol.org/content/180/8/5327 Downloaded from References This article cites 43 articles, 21 of which you can access for free at: http://www.jimmunol.org/content/180/8/5327.full#ref-list-1 http://www.jimmunol.org/ Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication by guest on September 27, 2021 *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2008 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Effector Memory ␣ T Lymphocytes Can Express Fc␥RIIIa and Mediate Antibody-Dependent Cellular Cytotoxicity1 Be´atrice Cle´menceau,*† Re´gine Vivien,*† Mathilde Berthome´,*† Nelly Robillard,‡ Richard Garand,‡ Ge´raldine Gallot,*† Sole`ne Vollant,*† and Henri Vie´2*† Human memory T cells are comprised of distinct populations with different homing potential and effector functions: central memory T cells that mount recall responses to Ags in secondary lymphoid organs, and effector memory T cells that confer immediate protection in peripheral tissues. -

CLINICAL TRIALS Safety and Immunogenicity of a Nicotine Conjugate Vaccine in Current Smokers
CLINICAL TRIALS Safety and immunogenicity of a nicotine conjugate vaccine in current smokers Immunotherapy is a novel potential treatment for nicotine addiction. The aim of this study was to assess the safety and immunogenicity of a nicotine conjugate vaccine, NicVAX, and its effects on smoking behavior. were recruited for a noncessation treatment study and assigned to 1 of 3 doses of the (68 ؍ Smokers (N nicotine vaccine (50, 100, or 200 g) or placebo. They were injected on days 0, 28, 56, and 182 and monitored for a period of 38 weeks. Results showed that the nicotine vaccine was safe and well tolerated. Vaccine immunogenicity was dose-related (P < .001), with the highest dose eliciting antibody concentrations within the anticipated range of efficacy. There was no evidence of compensatory smoking or precipitation of nicotine withdrawal with the nicotine vaccine. The 30-day abstinence rate was significantly different across with the highest rate of abstinence occurring with 200 g. The nicotine vaccine appears ,(02. ؍ the 4 doses (P to be a promising medication for tobacco dependence. (Clin Pharmacol Ther 2005;78:456-67.) Dorothy K. Hatsukami, PhD, Stephen Rennard, MD, Douglas Jorenby, PhD, Michael Fiore, MD, MPH, Joseph Koopmeiners, Arjen de Vos, MD, PhD, Gary Horwith, MD, and Paul R. Pentel, MD Minneapolis, Minn, Omaha, Neb, Madison, Wis, and Rockville, Md Surveys show that, although about 41% of smokers apy, is about 25% on average.2 Moreover, these per- make a quit attempt each year, less than 5% of smokers centages most likely exaggerate the efficacy of are successful at remaining abstinent for 3 months to a intervention because these trials are typically composed year.1 Smokers seeking available behavioral and phar- of subjects who are highly motivated to quit and who macologic therapies can enhance successful quit rates are free of complicating diagnoses such as depression 2 by 2- to 3-fold over control conditions. -

B Cell Activation and Escape of Tolerance Checkpoints: Recent Insights from Studying Autoreactive B Cells
cells Review B Cell Activation and Escape of Tolerance Checkpoints: Recent Insights from Studying Autoreactive B Cells Carlo G. Bonasia 1 , Wayel H. Abdulahad 1,2 , Abraham Rutgers 1, Peter Heeringa 2 and Nicolaas A. Bos 1,* 1 Department of Rheumatology and Clinical Immunology, University Medical Center Groningen, University of Groningen, 9713 Groningen, GZ, The Netherlands; [email protected] (C.G.B.); [email protected] (W.H.A.); [email protected] (A.R.) 2 Department of Pathology and Medical Biology, University Medical Center Groningen, University of Groningen, 9713 Groningen, GZ, The Netherlands; [email protected] * Correspondence: [email protected] Abstract: Autoreactive B cells are key drivers of pathogenic processes in autoimmune diseases by the production of autoantibodies, secretion of cytokines, and presentation of autoantigens to T cells. However, the mechanisms that underlie the development of autoreactive B cells are not well understood. Here, we review recent studies leveraging novel techniques to identify and characterize (auto)antigen-specific B cells. The insights gained from such studies pertaining to the mechanisms involved in the escape of tolerance checkpoints and the activation of autoreactive B cells are discussed. Citation: Bonasia, C.G.; Abdulahad, W.H.; Rutgers, A.; Heeringa, P.; Bos, In addition, we briefly highlight potential therapeutic strategies to target and eliminate autoreactive N.A. B Cell Activation and Escape of B cells in autoimmune diseases. Tolerance Checkpoints: Recent Insights from Studying Autoreactive Keywords: autoimmune diseases; B cells; autoreactive B cells; tolerance B Cells. Cells 2021, 10, 1190. https:// doi.org/10.3390/cells10051190 Academic Editor: Juan Pablo de 1. -

Case of the Anti HIV-1 Antibody, B12
Spectrum of Somatic Hypermutations and Implication on Antibody Function: Case of the anti HIV-1 antibody, b12 Mesfin Mulugeta Gewe A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy University of Washington 2015 Reading Committee: Roland Strong, Chair Nancy Maizels Jessica A. Hamerman Program Authorized to Offer Degree: Molecular and Cellular Biology i ii ©Copyright 2015 Mesfin Mulugeta Gewe iii University of Washington Abstract Spectrum of Somatic Hypermutations and Implication on Antibody Function: Case of the anti HIV-1 antibody, b12 Mesfin Mulugeta Gewe Chair of the Supervisory Committee: Roland Strong, Full Member Fred Hutchinson Cancer Research Center Sequence diversity, ability to evade immune detection and establishment of human immunodeficiency virus type 1 (HIV-1) latent reservoirs present a formidable challenge to the development of an HIV-1 vaccine. Structure based vaccine design stenciled on infection elicited broadly neutralizing antibodies (bNAbs) is a promising approach, in some measure to circumvent existing challenges. Understanding the antibody maturation process and importance of the high frequency mutations observed in anti-HIV-1 broadly neutralizing antibodies are imperative to the success of structure based vaccine immunogen design. Here we report a biochemical and structural characterization for the affinity maturation of infection elicited neutralizing antibodies IgG1 b12 (b12). We investigated the importance of affinity maturation and mutations accumulated therein in overall antibody function and their potential implications to vaccine development. Using a panel of point iv reversions, we examined relevance of individual amino acid mutations acquired during the affinity maturation process to deduce the role of somatic hypermutation in antibody function. -

Our Immune System (Children's Book)
OurOur ImmuneImmune SystemSystem A story for children with primary immunodeficiency diseases Written by IMMUNE DEFICIENCY Sara LeBien FOUNDATION A note from the author The purpose of this book is to help young children who are immune deficient to better understand their immune system. What is a “B-cell,” a “T-cell,” an “immunoglobulin” or “IgG”? They hear doctors use these words, but what do they mean? With cheerful illustrations, Our Immune System explains how a normal immune system works and what treatments may be necessary when the system is deficient. In this second edition, a description of a new treatment has been included. I hope this book will enable these children and their families to explore together the immune system, and that it will help alleviate any confusion or fears they may have. Sara LeBien This book contains general medical information which cannot be applied safely to any individual case. Medical knowledge and practice can change rapidly. Therefore, this book should not be used as a substitute for professional medical advice. SECOND EDITION COPYRIGHT 1990, 2007 IMMUNE DEFICIENCY FOUNDATION Copyright 2007 by Immune Deficiency Foundation, USA. Readers may redistribute this article to other individuals for non-commercial use, provided that the text, html codes, and this notice remain intact and unaltered in any way. Our Immune System may not be resold, reprinted or redistributed for compensation of any kind without prior written permission from Immune Deficiency Foundation. If you have any questions about permission, please contact: Immune Deficiency Foundation, 40 West Chesapeake Avenue, Suite 308, Towson, MD 21204, USA; or by telephone at 1-800-296-4433. -

Focus on Γδ T and NK Cells
cells Review Engineering the Bridge between Innate and Adaptive Immunity for Cancer Immunotherapy: Focus on γδ T and NK Cells 1, 2, 1 2, , Fabio Morandi y , Mahboubeh Yazdanifar y , Claudia Cocco , Alice Bertaina * z and 1, , Irma Airoldi * z 1 Stem Cell Laboratory and Cell Therapy Center, IRCCS Istituto Giannina Gaslini, Via G. Gaslini, 516147 Genova, Italy; [email protected] (F.M.); [email protected] (C.C.) 2 Stem Cell Transplantation and Regenerative Medicine, Department of Pediatrics, Stanford University School of Medicine, Palo Alto, CA 94305, USA; [email protected] * Correspondence: [email protected] (A.B.); [email protected] (I.A.) These authors have contributed equally to this work as first author. y These authors have contributed equally to this work as last author. z Received: 1 June 2020; Accepted: 21 July 2020; Published: 22 July 2020 Abstract: Most studies on genetic engineering technologies for cancer immunotherapy based on allogeneic donors have focused on adaptive immunity. However, the main limitation of such approaches is that they can lead to severe graft-versus-host disease (GvHD). An alternative approach would bolster innate immunity by relying on the natural tropism of some subsets of the innate immune system, such as γδ T and natural killer (NK) cells, for the tumor microenvironment and their ability to kill in a major histocompatibility complex (MHC)-independent manner. γδ T and NK cells have the unique ability to bridge innate and adaptive immunity while responding to a broad range of tumors. Considering these properties, γδ T and NK cells represent ideal sources for developing allogeneic cell therapies. -

Predominant Activation and Expansion of V Gamma 9-Bearing Gamma Delta T Cells in Vivo As Well As in Vitro in Salmonella Infection
Predominant activation and expansion of V gamma 9-bearing gamma delta T cells in vivo as well as in vitro in Salmonella infection. T Hara, … , G Matsuzaki, Y Yoshikai J Clin Invest. 1992;90(1):204-210. https://doi.org/10.1172/JCI115837. Research Article Gamma delta T cell receptor-positive cells (gamma delta T cells) have recently been implicated to play a role in the protection against infectious pathogens. Serial studies on gamma delta T cells in 14 patients with salmonella infection have revealed that the proportions of gamma delta T cells (mean +/- SD: 17.9 +/- 13.2%) in salmonella infection were significantly increased (P less than 0.01) compared with 35 normal controls (5.0 +/- 2.6%) and 13 patients with other bacterial infections (4.0 +/- 1.4%). Expansion of gamma delta T cells was more prominent in the systemic form (28.9 +/- 10.8%) than in the gastroenteritis form (10.5 +/- 7.9%) of salmonella infection (P less than 0.01). Most in vivo-expanded gamma delta T cells expressed V gamma 9 gene product. Increased activated (HLA-DR+) T cells were observed in all the six patients with the systemic form and four of the seven with gastroenteritis form. Especially in the six with systemic form, gamma delta T cell activation was significantly higher than alpha beta T cell activation at the early stage of illness (P less than 0.01). When peripheral blood lymphocytes from normal individuals were cultured with live salmonella, gamma delta T cells were preferentially activated and expanded and most of them expressed V gamma 9. -
Eosinophil Extracellular Traps and Inflammatory Pathologies—Untangling the Web!
REVIEW published: 26 November 2018 doi: 10.3389/fimmu.2018.02763 Eosinophil Extracellular Traps and Inflammatory Pathologies—Untangling the Web! Manali Mukherjee 1*, Paige Lacy 2 and Shigeharu Ueki 3 1 Department of Medicine, McMaster University and St Joseph’s Healthcare, Hamilton, ON, Canada, 2 Department of Medicine, Alberta Respiratory Centre, University of Alberta, Edmonton, AB, Canada, 3 Department of General Internal Medicine and Clinical Laboratory Medicine, Akita University Graduate School of Medicine, Akita, Japan Eosinophils are an enigmatic white blood cell, whose immune functions are still under intense investigation. Classically, the eosinophil was considered to fulfill a protective role against parasitic infections, primarily large multicellular helminths. Although eosinophils are predominantly associated with parasite infections, evidence of a role for eosinophils in mediating immunity against bacterial, viral, and fungal infections has been recently reported. Among the mechanisms by which eosinophils are proposed to exert their protective effects is the production of DNA-based extracellular traps (ETs). Remarkably, Edited by: DNA serves a role that extends beyond its biochemical function in encoding RNA and Moncef Zouali, protein sequences; it is also a highly effective substance for entrapment of bacteria Institut National de la Santé et de la and other extracellular pathogens, and serves as valuable scaffolding for antimicrobial Recherche Médicale (INSERM), France mediators such as granule proteins from immune cells. Extracellular -
Of T Cell Tolerance
cells Review Strength and Numbers: The Role of Affinity and Avidity in the ‘Quality’ of T Cell Tolerance Sébastien This 1,2,† , Stefanie F. Valbon 1,2,†, Marie-Ève Lebel 1 and Heather J. Melichar 1,3,* 1 Centre de Recherche de l’Hôpital Maisonneuve-Rosemont, Montréal, QC H1T 2M4, Canada; [email protected] (S.T.); [email protected] (S.F.V.); [email protected] (M.-È.L.) 2 Département de Microbiologie, Immunologie et Infectiologie, Université de Montréal, Montréal, QC H3C 3J7, Canada 3 Département de Médecine, Université de Montréal, Montréal, QC H3T 1J4, Canada * Correspondence: [email protected] † These authors contributed equally to this work. Abstract: The ability of T cells to identify foreign antigens and mount an efficient immune response while limiting activation upon recognition of self and self-associated peptides is critical. Multiple tolerance mechanisms work in concert to prevent the generation and activation of self-reactive T cells. T cell tolerance is tightly regulated, as defects in these processes can lead to devastating disease; a wide variety of autoimmune diseases and, more recently, adverse immune-related events associated with checkpoint blockade immunotherapy have been linked to a breakdown in T cell tolerance. The quantity and quality of antigen receptor signaling depend on a variety of parameters that include T cell receptor affinity and avidity for peptide. Autoreactive T cell fate choices (e.g., deletion, anergy, regulatory T cell development) are highly dependent on the strength of T cell receptor interactions with self-peptide. However, less is known about how differences in the strength Citation: This, S.; Valbon, S.F.; Lebel, of T cell receptor signaling during differentiation influences the ‘function’ and persistence of anergic M.-È.; Melichar, H.J. -

Defining Natural Antibodies
PERSPECTIVE published: 26 July 2017 doi: 10.3389/fimmu.2017.00872 Defining Natural Antibodies Nichol E. Holodick1*, Nely Rodríguez-Zhurbenko2 and Ana María Hernández2* 1 Department of Biomedical Sciences, Center for Immunobiology, Western Michigan University Homer Stryker M.D. School of Medicine, Kalamazoo, MI, United States, 2 Natural Antibodies Group, Tumor Immunology Division, Center of Molecular Immunology, Havana, Cuba The traditional definition of natural antibodies (NAbs) states that these antibodies are present prior to the body encountering cognate antigen, providing a first line of defense against infection thereby, allowing time for a specific antibody response to be mounted. The literature has a seemingly common definition of NAbs; however, as our knowledge of antibodies and B cells is refined, re-evaluation of the common definition of NAbs may be required. Defining NAbs becomes important as the function of NAb production is used to define B cell subsets (1) and as these important molecules are shown to play numerous roles in the immune system (Figure 1). Herein, we aim to briefly summarize our current knowledge of NAbs in the context of initiating a discussion within the field of how such an important and multifaceted group of molecules should be defined. Edited by: Keywords: natural antibody, antibodies, natural antibody repertoire, B-1 cells, B cell subsets, B cells Harry W. Schroeder, University of Alabama at Birmingham, United States NATURAL ANTIBODY (NAb) PRODUCING CELLS Reviewed by: Andre M. Vale, Both murine and human NAbs have been discussed in detail since the late 1960s (2, 3); however, Federal University of Rio cells producing NAbs were not identified until 1983 in the murine system (4, 5). -
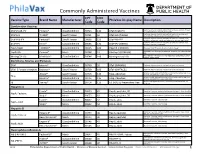
Commonly Administered Vaccines
Commonly Administered Vaccines CPT CVX Vaccine Type Brand Name Manufacturer PhilaVax Display Name Description Code Code Combination Vaccines Diptheria, tetanus toxoids and acellular pertussis vaccine, Hepati- DTaP-HepB-IPV Pediarix® GlaxoSmithKline 90723 110 DTaP-HepB-IPV tis B and poliovirus vaccine, inactivated Diptheria, tetanus toxoids and acellular pertussis vaccine and DTaP-Hib TriHIBit® Sanofi Pasteur 90721 50 DTaP-Hib (TriHIBit) Haemophilus influenzae type b conjugate vaccine Diptheria, tetanus toxoids and acellular pertussis vaccine, Hae- DTaP-Hib-IPV Pentacel® Sanofi Pasteur 90698 120 DTaP-Hib-IPV mophilus influenzae type b, and poliovirus vaccine, inactivated Diptheria, tetanus toxoids and acellular pertussis vaccine, and DTaP-IPV Kinrix® GlaxoSmithKline 90696 130 DTaP-IPV (KINRIX) poliovirus vaccine, inactivated HepA-HepB TWINRIX® GlaxoSmithKline 90636 104 HepA/B (TWINRIX) Hepatisis A and Hepatitis B vaccine, adult dosage Hepatitis B and Hemophilus influenza b vaccine, for intramuscular HepB-Hib Comvax® Merck 90748 51 Hib-Hep B (COMVAX) use Haemophilus influenza b and meningococcal sero groups C and Y MeningC/Y-Hib Menhibrix® GlaxoSmithKline 90644 148 Meningococcal-Hib vaccine, 4 dose series Diphtheria, Tetanus and Pertussis DTaP Infanrix® GlaxoSmithKline 90700 20 DTaP (INFANRIX) Diptheria, tetanus toxoids and acellular pertussis vaccine DTaP, 5 Pertussis Antigens Daptacel® Sanofi Pasteur 90700 106 DTaP (DAPTACEL) Diptheria, tetanus toxoids and acellular pertussis vaccine Tetanus toxoid, reduced diphtheria toxoid, and acellular -

B Cell Checkpoints in Autoimmune Rheumatic Diseases
REVIEWS B cell checkpoints in autoimmune rheumatic diseases Samuel J. S. Rubin1,2,3, Michelle S. Bloom1,2,3 and William H. Robinson1,2,3* Abstract | B cells have important functions in the pathogenesis of autoimmune diseases, including autoimmune rheumatic diseases. In addition to producing autoantibodies, B cells contribute to autoimmunity by serving as professional antigen- presenting cells (APCs), producing cytokines, and through additional mechanisms. B cell activation and effector functions are regulated by immune checkpoints, including both activating and inhibitory checkpoint receptors that contribute to the regulation of B cell tolerance, activation, antigen presentation, T cell help, class switching, antibody production and cytokine production. The various activating checkpoint receptors include B cell activating receptors that engage with cognate receptors on T cells or other cells, as well as Toll-like receptors that can provide dual stimulation to B cells via co- engagement with the B cell receptor. Furthermore, various inhibitory checkpoint receptors, including B cell inhibitory receptors, have important functions in regulating B cell development, activation and effector functions. Therapeutically targeting B cell checkpoints represents a promising strategy for the treatment of a variety of autoimmune rheumatic diseases. Antibody- dependent B cells are multifunctional lymphocytes that contribute that serve as precursors to and thereby give rise to acti- cell- mediated cytotoxicity to the pathogenesis of autoimmune diseases