Camp Lejeune Drinking Water U.S
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

North Carolina Department of Natural and Cultural Resources State Historic Preservation Office Ramona M
North Carolina Department of Natural and Cultural Resources State Historic Preservation Office Ramona M. Bartos, Administrator Governor Roy Cooper Office of Archives and History Secretary Susi H. Hamilton Deputy Secretary Kevin Cherry August 10, 2018 Rick Richardson [email protected] Cultural Resources Program, USMC Camp Lejeune 12 Post Lane MCIEast-MCB Camp Lejeune Camp Lejeune, NC 28547 Re: Historic Resource Re-evaluation Report, Stone Bay Rifle Range Historic District, Camp Lejeune, Onslow County, ER 07-2777 Dear Mr. Richardson: Thank you for your email of July 19, 2018, transmitting the above-referenced report. We have reviewed the materials submitted regarding the Stone Bay Rifle Range Historic District (ON1030), which was determined eligible for the National Register of Historic Places (NRHP) in 2000. We concur that a boundary decrease is warranted. However, we recommend that the boundary continue to include the remaining contributing structures of the “village.” The revised south boundary would run east with Powder Lane across Rifle Range Road to the eastern district boundary as shown on the enclosed map. We concur that the district remains eligible for listing under Criterion A for military history. Furthermore, we believe the district to be eligible under Criterion C as the entirety of the complex, village and ranges, represents a “significant and distinguished entity” of military design and construction. The above comments are made pursuant to Section 106 of the National Historic Preservation Act and the Advisory Council on Historic Preservation’s Regulations for Compliance with Section 106 codified at 36 CFR Part 800. Thank you for your cooperation and consideration. -
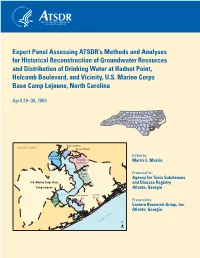
Expert Panel Assessing ATSDR's Methods and Analyses for Historical
Expert Panel Assessing ATSDR’s Methods and Analyses for Historical Reconstruction of Groundwater Resources and Distribution of Drinking Water at Hadnot Point, Holcomb Boulevard, and Vicinity, U.S. Marine Corps Base Camp Lejeune, North Carolina April 29 –30, 2009 NORTH CAROLINA Montford Point ONSLOW COUNTY Tarawa Terrace New River Edited by: Air Station Holcomb Boulevard Morris L. Maslia New Hadnot Prepared for: Point Agency for Toxic Substances U.S. Marine Corps Base and Disease Registry Camp Lejeune Atlanta, Georgia River Courthouse Onslow Rifle Bay Beach Range Prepared by: Eastern Research Group, Inc. Atlanta, Georgia Atlantic Ocean N Cover. Location of U.S. Marine Corps Base Camp Lejeune, North Carolina, and historical water-supply areas. Expert Panel Assessing ATSDR’s Methods and Analyses for Historical Reconstruction of Groundwater Resources and Distribution of Drinking Water at Hadnot Point, Holcomb Boulevard, and Vicinity, U.S. Marine Corps Base Camp Lejeune, North Carolina April 29–30, 2009 Edited by: Morris L. Maslia Prepared for: Agency for Toxic Substances and Disease Registry Atlanta, Georgia Prepared by: Eastern Research Group, Inc. Atlanta, Georgia Atlanta, Georgia December 2009 ii Suggested citation: Maslia ML, editor, 2009, Expert Panel Assessing ATSDR’s Methods and Analyses for Historical Reconstruction of Groundwater Resources and Distribution of Drinking Water at Hadnot Point, Holcomb Boulevard, and Vicinity, U.S. Marine Corps Base Camp Lejeune, North Carolina, April 29–30, 2009: Prepared by Eastern Research Group, Inc., -

Raider Patch Magazine of the Marine Raider Association No
The Raider Patch Magazine of the Marine Raider Association No. 150 1st Qtr 2021 Doc Gleason Essay Contest Winners Cognitive Raider Essay Contest Open The Story of PFC Bruno Oribiletti marineraiderassociation.org A National Non-Profit Organization Supporting: The Marine Raider Museum at Raider Hall, Quantico VA Executive Committee and Directors: President and Director 1st Vice President and Director Pending Col Neil Schuehle, USMC (Ret) MSgt Zach Peters, USMC (Ret) 2nd Vice President and Director (1st MRB, MRTC) (1st MRB) [email protected] [email protected] [email protected] Secretary and Director Membership Secretary and Director Treasurer and Director LtCol Wade Priddy, USMC (Ret) MSgt Micheal Poggi, USMC (Ret) Sigrid Klock McAllister, (Hon 2BN) (Det-1) (2nd MRB, MRTC) 1855 Kanawha Trail [email protected] [email protected] Stone Mountain, GA 30087-2132 (770)-939-3692 Past President and Director [email protected] Col Craig Kozeniesky, USMC (Ret) (Det-1, MARSOC HQ) Directors: MajGen Mark Clark, USMC (Ret) MSgt John Dailey USMC (Ret) MGySgt Corey Nash, USMC (Ret) (MARSOC HQ) (Det-1, MRTC) (3MRB, MRTC, HQ) [email protected] GySgt Oscar Contreras, USMC (Ret) Col J. Darren Duke, USMC LtCol Jack O'Toole, USMC (Ret) (1st MRB, MRTC) (3rd MRB, MARSOC HQ, MRSG) (MARSOC HQ) Officers: Chaplain Legal Counsel Historical and Legacy Preservation John S. Eads IV Paul Tetzloff Bruce N. Burlingham- WWII Historian [email protected] Pete Bartle Doug Bailey Communications Committee Advisor Public Affairs Louie Marsh Membership Committee Bill EuDaly (Hon 4th Bn.) Jenny Ruffini (Hon) Emeritus Board Members: Bob Buerlein (Hon) Jim Johannes (Hon) Robert J. -

Iwo Jima 75 Years on the Big Island’S Role in the Invasion
Vol. 76 No. 2 • SPRING 2020 Iwo Jima 75 Years On The Big Island’s Role in the Invasion SF Interviews Mosul Hero Corporal Sky Barkley Honoring PNC Richard D. Gore, Sr. What Kind of Hearing Aids Do Doctors Use? The same ones they recommend to their patients! Advanced Digital Hearing Aid Technology BUY 1 Reg: $399.98 GET 1 FREE Only $199 99 Each When You Buy a Pair – LIMITED TIME ONLY! Doctors love MDHearingAids® for the same reasons patients do. These Nearly invisible! FDA-registered, medical-grade hearing aids have the same high-tech features found in more expensive hearing aids at a fraction of the cost. “MDHearingAids are better than expensive clinic hearing aids, which cost thousands more,” says retired physician Dr. Robert A. “I have had fi ve pairs of expensive hearing aids and MDHearingAids are just as good,” adds retired neurosurgeon Dr. Brian L. Doctors Are Tired of Watching Their Patients Waste Money on Over-Priced Clinic Hearing Aids MDHearingAids are the best value on the market, says Dr. Clarke: “I’m a physician, and I know how much people spend on health care. SAVE 90% COMPARED TO They should get the best value, and this product is just as effective TRADITIONAL (if not more) than traditional overly-priced hearing aids. I will HEARING AIDS be recommending MDHearingAids to my hearing-impaired patients.” CRISP, CLEAR SOUND STATE-OF-THE-ART FEATURES NO AUDIOLOGIST NEEDED MDHearingAids were created by Behind-the-ear hearing aid with Save time and money, cancel a board-certifi ed otolaryngologist thin tubing for a nearly invisible those audiologist appointments! frustrated that patients couldn’t profi le. -
NPS-LM-20-022.Pdf
NPS-LM-20-022 ACQUISITION RESEARCH PROGRAM SPONSORED REPORT SERIES Maximizing Resources through Secondary Reparable (SECREP) Residual Demand Management December 2019 Maj Alexander Mora, USMC Thesis Advisors: Dr. Kenneth H Doerr, Associate Professor Chad W Seagren, Senior Lecturer Graduate School of Defense Management Naval Postgraduate School Approved for public release; distribution is unlimited. Prepared for the Naval Postgraduate School, Monterey, CA 93943. Acquisition Research Program Graduate School of Defense Management Naval Postgraduate School The research presented in this report was supported by the Acquisition Research Program of the Graduate School of Defense Management at the Naval Postgraduate School. To request defense acquisition research, to become a research sponsor, or to print additional copies of reports, please contact the Acquisition Research Program (ARP) via email, [email protected] or at 831-656-3793. Acquisition Research Program Graduate School of Defense Management Naval Postgraduate School ABSTRACT This research analyzed the practices associated with maintaining a safety stock of secondary reparables (SECREP) to meet United States Marine Corps (USMC) demand. This research found evidence of accelerated spending on SECREPs in the fourth quarter, but no evidence that increased spending improved readiness. Currently, USMC bases its annual SECREP requirement on execution data (expenditures) from previous years, rather than actual demand. We conclude that the RIPs should use actual demand data to estimate future demand, -

33 CFR Ch. II (7–1–20 Edition)
Pt. 334 33 CFR Ch. II (7–1–20 Edition) (2) For in-lieu fee project sites, real land bank) must be consistent with the estate instruments, management plans, terms of this part. or other long-term protection mecha- (2) In-lieu fee program instruments. All nisms used for site protection must be in-lieu fee program instruments ap- finalized before advance credits can be- proved on or after July 9, 2008 must come released credits. meet the requirements of this part. In- (u) Long-term management. (1) The lieu fee programs operating under in- legal mechanisms and the party re- struments approved prior to July 9, sponsible for the long-term manage- 2008 may continue to operate under ment and the protection of the mitiga- those instruments for two years after tion bank site must be documented in the effective date of this rule, after the instrument or, in the case of um- which time they must meet the re- brella mitigation banking instruments quirements of this part, unless the dis- and in-lieu fee programs, the approved trict engineer determines that cir- mitigation plans. The responsible party cumstances warrant an extension of up should make adequate provisions for to three additional years. The district the operation, maintenance, and long- engineer must consult with the IRT be- term management of the compensatory fore approving such extensions. Any re- mitigation project site. The long-term visions made to the in-lieu fee program management plan should include a de- instrument on or after July 9, 2008 scription of long-term management must be consistent with the terms of needs and identify the funding mecha- this part. -

Marine Corps Base Camp Lejeune and Marine Corps Air Station, New River 2020 Telephone Directory
MARINE CORPS BASE CAMP LEJEUNE AND MARINE CORPS AIR STATION, NEW RIVER 2020 TELEPHONE DIRECTORY DO NOT DISCUSS CLASSIFIED INFORMATION ON NONSECURE TELEPHONES. OFFICIAL DOD TELEPHONES ARE SUBJECT TO MONITORING FOR COMMUNICATIONS SECURITY PURPOSES AT ALL TIMES. FIRE/CRASH AMBULANCE PMO EOD COMMAND DUTY OFFICERS 9-1-1 9-1-1 9-1-1 9-1-1 II MEF ...................................... 451-8138 Hearing 2D MARDIV ................................... 451-8319 Impaired 451-3004 2D MLG ...................................... 451-0850 Emergency 451-3005 MCIEAST / MCB CLNC .......................... 451-2414 Number MARSOC ...................................... 440-0938 451-4444 MCAS, New River ............................. 449-5411 451-2889 Supv AIRCRAFT RESCUE & FIREFIGHTING (NON-EMERGENCY) 24 HOUR DISPATCH ........... 449-5177/6629/6624 ON DUTY STATION CAPTAIN .............. 449-7641 HAZARDOUS CHEMICAL SPILLAGE ................................................................. 9 - 1 - 1 FAMILY HOUSING Atlantic Marine Corps Communities (AMCC) Maintenance (24 Hour) .......... 1-877-509-2424 FAMILY HOUSING LINCOLN MILITARY MAINTENANCE (24 HOURS) ................................. 1-888-578-4141 EMERGENCY MAINTENANCE (24 Hour Service) ...................................................... 451-3001 INFORMATION TECHNOLOGY CUSTOMER SERVICE CENTER ........................................ 1-855--624-3278 ............................................................................................. 451-1019 TELEPHONE CABLE LOCATER SERVICE ........................................................ -

Marine Corps Base Camp Lejeune and Marine Corps Air Station, New River 2017 Telephone Directory
MARINE CORPS BASE CAMP LEJEUNE AND MARINE CORPS AIR STATION, NEW RIVER 2017 TELEPHONE DIRECTORY DO NOT DISCUSS CLASSIFIED INFORMATION ON NONSECURE TELEPHONES. OFFICIAL DOD TELEPHONES ARE SUBJECT TO MONITORING FOR COMMUNICATIONS SECURITY PURPOSES AT ALL TIMES. FIRE AMBULANCE PMO EOD COMMAND DUTY OFFICERS 9-1-1 9-1-1 9-1-1 9-1-1 lI MEF…………………………………………………………451-8138 Hearing Impaired 2D MARDIV………………………………………………….451-8319 Emergency 451-3004 2D MLG……………………………………………………....451-0850 Number 3005 MCIEAST / MCB CLNC……………………………………451-2414 451-4444 MARSOC………………………………………………….....440-0938 MCAS, New River………………………………449-6305/449-5411 451-2889 supv. AIRCRAFT CRASH CREW . 449-6629 . 449-6224 HAZARDOUS CHEMICAL SPILLAGE………………………………………………………………………………….………………..9 - 1 - 1 FAMILY HOUSING Atlantic Marine Corps Communities (AMCC) Maintenance (24 Hour)……………………….……..1-877-509-2424 FAMILY HOUSING LINCOLN MILITARY MAINTENANCE (24 HOURS)…………………………………………...……..1-888-578-4141 EMERGENCY MAINTENANCE (24 Hour Service)…………………………………………………………………………………..451-3001 INFORMATION TECHNOLOGY CUSTOMER SERVICE CENTER………… 1-855--624-3278……………………………….451-1019 TELEPHONE CABLE LOCATER SERVICE…………………………………………………………………………………………..451-3100 TELEPHONE TROUBLE CALLS/REPAIR…………………………………………………………………………………………….451-1114 OPERATOR ASSISTANCE…………………………………………………………………………………………………………….451-1113 DIRECTORY ASSISTANCE……………………………………………………………………………………………………………451-1113 TIME AND TEMPERATURE……………………………………………………………………………………………………………451-3000 DSN PREFIXES…………………………………………………………………………………………………..750 (450 Commercial Prefix) -

Onslow County, North Carolina Data Center
January ‘17 ONSLOW COUNTY, NORTH CAROLINA DATA CENTER JANUARY 2017 QUARTERLY UPDATE ONSLOW COUNTY PLANNING & DEVELOPMENT DEPARTMENT 604 COLLEGE STREET JACKSONVILLE, N.C. 28540 MATT STUART, COMMUNITY DEVELOPMENT PLANNER (910) 989-3081 WWW.ONSLOWCOUNTYNC.GOV January ‘17 TABLE OF CONTENTS HISTORICAL OVERVIEW OF ONSLOW COUNTY…………………………………3 OPERATING INDICATORS BY FUNCTION/PROGRAM……………………………4 DEMOGRAPHIC DATA………………………………………………………………...5 POPULATION BY MUNICIPALITY & TOWNSHIP………………………………….6 NORTH CAROLINA’S TOP 10 CITIES AND COUNTIES IN POPULATION………7 BUSINESS DATA……………………………………………………………………….8 ESTABLISHMENTS…………………………………………………………………….9 TOP 25 EMPLOYERS…………………………………………………………………..10 TEN LARGEST TAXPAYERS…………………………………………………………11 AGRICULTURAL DATA………………………………………………………………12 ONSLOW COUNTY EMPLOYMENT & WAGES BY SECTOR…………………….13 MARINE CORPS BASE CAMP LEJEUNE, SIGNIFICANT FACTS…………...........14 MARINE CORPS BASE CAMP LEJEUNE, QUARTERLY AREA POPULATION REPORT…………………………………………………………………………………15 HOUSING UNITS BY TIME PERIOD BUILT………………………………………...17 LABOR FORCE STATISTICS………………………………………………………….18 TOURISM REVENUE…………………………………………………………………..19 PROPERTY TAX RATES………………………………………………………………20 SELECTED VITAL STATISTICS……………………………………………………...21 STRUCTURES BY TAX LISTING………………………………….............................22 REAL ESTATE MARKET DATA………………………………………………………23 ONSLOW COUNTY PERMIT DATA………………………………………………….24 HOUSEHOLDS & FAMILIES BY INCOME RANGE………………………………...25 2 January ‘17 HISTORICAL OVERVIEW OF ONSLOW COUNTY Attracted by the waterways and longleaf pine forests, -
2020 Newsletter
ENGINEERS UP! 2020 Newsletter Engineers Up! - 1 MARINE CORPS ENGINEER ASSOCIATION What is it? The MCEA is a HQMC sanctioned, tax-exempt, nonprofit organization (IRS 501 (c) (19)), incorporated in NC, in 1991. MCEA Purpose/Bylaw highlights: - Promote Marine Corps engineering in combat engineer, engineer equipment, utilities, landing support (shore party), bulk fuel, topographic and construction engineering, drafting, and Explosive Ordnance Disposal (EOD) - Renew and perpetuate fellowship of retired, former and current US Marines who served with Marine Corps Engineer units and sister service members who served in support of Marine-Air-Ground Task Force (MAGTF) Units - Preserve the memory of those who served - Promote an accurate historical record of the contributions of Marine Corps engineers - Foster solidarity of Marine Corps engineers - Keep members current with the Marine Corps engineer community - Annually recognize superior achievement of active duty and reserve establishment Marine Corps EOD and engineer individuals & organizations, as well as Naval Construction Force Units MCEA Eligibility. All former and current Armed Forces personnel who served with Marine Corps Air Ground Task Force (MAGTF) Units or in support of Marine Corps Engineer Units or US Marine Corps Base and Station billets. Membership Benefits: - Very affordable dues for yearly, multi-year & lifetime membership! 100% of dues and all contributions are tax deductible. - Contributions to MCEA, Unit brick program and school sponsorship qualify for the Fellows Program. - -

2D MLG MAG MONTHLY AMMO for YOUR MENTORING and LEADERSHIP ARSENALS 2Ndmlg
Volume 1 Issue VII [email protected] INNOVAT CE,, ION,, LEN QU EL AL C IT EX Y 2ndmlg_marines 2 P d U MA O ARI GR INE LOGISTICS @2ndMLG OGIS W S A OR RR RIO IOR AR S SUSTAINING W 2D MLG MAG MONTHLY AMMO FOR YOUR MENTORING AND LEADERSHIP ARSENALS 2ndMLG U.S. Marines with Combat Logistics Regiment (CLR) 27, 2nd Marine Logistics Group, II Marine Expeditionary Force, march on the colors during the 244th Marine Corps Birthday Ball at Geottge Memorial Field House on Camp Lejeune, North Carolina, Nov. 7, 2019. Marines with CLR 27 celebrate the Birthday Ball in compliance with the will of the 13th Commandant of the Marine Corps Lt. Gen. John A. Lejeune to honor the history and traditions of the Marine Corps since Nov. 10, 1775. (U.S. Marine Corps photo by Cpl. Adaezia Chavez) MONTHLY ACTIVITIES: Remember to check this link every week to see the updated list with lots of fun and free activities for you, your friends, and family! We are also including a list of courses designated to help improve lives and enhance your personal and professional relationships, offerered through the prevention and education program at FAP! Tap, Rack, Bang P3 Birthday Meaning P5 Chaplain’s Corner P5 Must read tips exclusively Happy 244th Birthday Taking a moment to reflect from Realwarriors.net Marine Corps on our history Relationship resilience is critical What does the Marine Corps birthday Captain Rob McClellen, CHC, USN, not just to the well-being of service mean to service members at 2D MLG? Group Chaplain, gives his insight on the members and their spouses, but to unit Check out our new section called share history of the Marine Corps Birthday. -

The Emergent1 Psychological Health System at Marine Corps, Base Camp Lejeune 2012-2015: Analysis and Recommendations
The Emergent1 Psychological Health System at Marine Corps, Base Camp Lejeune 2012-2015: Analysis and Recommendations January 12, 2016 Dr. Amy Glasmeier PhD Mr. Eric Schultheis JD Dr. Annette Sassi PhD Dr. Christa Lee Chuvala PhD Mr. Andrew Bell Mr. John Fay Sociotechnical Systems Research Center Massachusetts Institute of Technology 77 Massachusetts Avenue, E38-632 Cambridge, MA 02139 This material is based on research sponsored by the USAMRMC (under the cooperative agreement number W81 XWH 12-2-0016) and a consortium of other government and industry members. The U.S. Government is authorized to reproduce and distribute reprints for Governmental purposes notwithstanding any copyright notation thereon. The views and conclusions contained herein are those of the authors and should not be interpreted as necessarily representing the official policies or endorsements, either expressed or implied, of the USAMRMC, the U.S. Government, or other consortium members. 1 Definition of the term “emergent” is discussed in the preface of the report. Executive Summary The Emergent Psychological Health System at Marine Corps, Base Camp Lejeune 2012-2015: Analysis and Recommendations January 2016 Executive Summary Overview: This report represents a synthesis of research conducted at the Marine Corps Base Camp Lejeune over the period 2012-Fall 2015. Objectives: Recognizing its large scale and history of battlefield innovation, in 2013 General Joseph Dunford offered Marine Corps Base Camp Lejeune as an interesting case to examine the system of care in its then current form and its ability to evolve. MCB Camp Lejeune offers interesting system level insights into the Marine Corps—insights that inform MIT’s research on the Memorandum of Understanding MOU signed in November 2013 by BUMED, MFP and Marine Corps Health Services.