Polygenic Evidence and Overlapped Brain Functional Connectivities For
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Imaging Genetic Strategies for Predicting the Quality of Sleep Using Depression-Specific Biomarkers
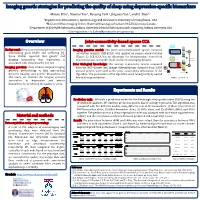
Imaging genetic strategies for predicting the quality of sleep using depression-specific biomarkers Mansu Kim 1, Xiaohui Yao 1, Bo-yong Park 2, Jingwen Yan 3, and Li Shen1,* 1Department of Biostatistics, Epidemiology and Informatics, University of Pennsylvania, USA 2McConnell Brain Imaging Centre, Montreal Neurological Institute, McGill University, Canada 3Department of BioHealth Informatics, Indiana University School of Informatics and Computing, Indiana University, USA * Correspondence to [email protected] Overview Joint-connectivity-based sparse CCA Background: Sleep is an essential phenomenon for SNP connectivity Imaging genetics model: The joint-connectivity-based sparse canonical ··· X* samples × maintaining good health and wellbeing [1]. correlation analysis (JCB-SCCA) was applied on preprocessed features n Some studies reported that genetic and p SNPs (Figure 1). JCB-SCCA has an advantage for incorporating connectivity Loading vector u Maximum imaging biomarkers that depression is information and can handle multi-modal neuroimaging datasets. correlation Brain associated with sleep disorder [2]–[4]. connectivity ··· Prior biological knowledge: The average connectivity matrix computed ··· K samples Y* modalitiesn × Imaging genetics: Many studies adopted imaging from the HCP dataset and linkage disequilibrium obtained from 1,000 q voxels genetics methodology to find associations genome project were used as the prior connectivity information of the K = 2 Loading vector V between imaging and genetic biomarkers. In algorithm. The parameters of the algorithm were tuned jointly by nested K = 1 this study, we examine the imaging genetics five-fold cross-validation. Figure 1. JCB-SCCA association in depression and extract biomarkers for predicting the quality of sleep. Experiments and Results Prediction task: We built a prediction model for the Pittsburgh sleep quality index (PSQI) using the identified biomarkers. -

Conservation and Divergence of Related Neuronal Lineages in The
RESEARCH ARTICLE Conservation and divergence of related neuronal lineages in the Drosophila central brain Ying-Jou Lee, Ching-Po Yang, Rosa L Miyares, Yu-Fen Huang, Yisheng He, Qingzhong Ren, Hui-Min Chen, Takashi Kawase, Masayoshi Ito, Hideo Otsuna, Ken Sugino, Yoshi Aso, Kei Ito, Tzumin Lee* Janelia Research Campus, Howard Hughes Medical Institute, Ashburn, United States Abstract Wiring a complex brain requires many neurons with intricate cell specificity, generated by a limited number of neural stem cells. Drosophila central brain lineages are a predetermined series of neurons, born in a specific order. To understand how lineage identity translates to neuron morphology, we mapped 18 Drosophila central brain lineages. While we found large aggregate differences between lineages, we also discovered shared patterns of morphological diversification. Lineage identity plus Notch-mediated sister fate govern primary neuron trajectories, whereas temporal fate diversifies terminal elaborations. Further, morphological neuron types may arise repeatedly, interspersed with other types. Despite the complexity, related lineages produce similar neuron types in comparable temporal patterns. Different stem cells even yield two identical series of dopaminergic neuron types, but with unrelated sister neurons. Together, these phenomena suggest that straightforward rules drive incredible neuronal complexity, and that large changes in morphology can result from relatively simple fating mechanisms. *For correspondence: Introduction [email protected] In order to understand how the genome encodes behavior, we need to study the developmental mechanisms that build and wire complex centers in the brain. The fruit fly is an ideal model system Competing interests: The to research these mechanisms. The Drosophila field has extensive genetic tools. -

Data Mining in Genomics, Metagenomics and Connectomics
Csaba Kerepesi DATA MINING IN GENOMICS, METAGENOMICS AND CONNECTOMICS PhD Thesis Supervisor: Dr. Vince Grolmusz Department of Computer Science E¨otv¨osLor´andUniversity, Hungary PhD School of Computer Science E¨otv¨osLor´andUniversity, Hungary Dr. Erzs´ebet Csuhaj-Varj´u PhD Program of Information Systems Dr. Andr´as Bencz´ur Budapest, 2017 Acknowledgements I would like to thank my supervisor Dr. Vince Grolmusz for his tireless support with which he started my scientific career. I am very grateful to the PhD School of Computer Science and the Faculty of Informatics, ELTE for their inexhaustible support. I would like to thank my co-authors for their precious work and I also would like to thank all my colleagues, who helped me anything in my re- searches. Finally, I would like to thank my family for their everlasting support. 2 Contents 1 Introduction 6 2 Data Mining in Genomics and Metagenomics 14 2.1 AmphoraNet: The Webserver Implementation of the AM- PHORA2 Metagenomic Workflow Suite . 14 2.1.1 Introduction . 14 2.1.2 Results and Discussion . 15 2.2 Visual Analysis of the Quantitative Composition of Metage- nomic Communities: the AmphoraVizu Webserver . 17 2.2.1 Introduction . 17 2.2.2 Results and Discussion . 19 2.3 Evaluating the Quantitative Capabilities of Metagenomic Analysis Software . 21 2.3.1 Introduction . 21 2.3.2 Results and discussion . 22 2.3.3 Methods . 25 2.3.4 Availability . 29 2.4 The \Giant Virus Finder" Discovers an Abundance of Giant Viruses in the Antarctic Dry Valleys . 30 2.4.1 Introduction . 30 3 2.4.2 Results and discussion . -

Local Connectome Phenotypes Predict Social, Health, and Cognitive Factors
RESEARCH Local connectome phenotypes predict social, health, and cognitive factors 1 2,3 4,5 Michael A. Powell , Javier O. Garcia , Fang-Cheng Yeh , 2,3,6 7 Jean M. Vettel , and Timothy Verstynen 1Department of Mathematical Sciences, United States Military Academy, West Point, NY, USA 2U.S. Army Research Laboratory, Aberdeen Proving Ground, MD, USA 3Department of Bioengineering, University of Pennsylvania, Philadelphia, PA, USA 4Department of Neurological Surgery, University of Pittsburgh Medical Center, Pittsburgh, PA, USA 5Department of Bioengineering, University of Pittsburgh, Pittsburgh, PA, USA 6Department of Psychological and Brain Sciences, University of California, Santa Barbara, CA, USA 7 an open access journal Department of Psychology and Center for the Neural Basis of Cognition, Carnegie Mellon University, Pittsburgh, PA, USA Keywords: Local connectome, White matter, Individual differences, Behavior prediction, Structural connectivity ABSTRACT The unique architecture of the human connectome is defined initially by genetics and subsequently sculpted over time with experience. Thus, similarities in predisposition and experience that lead to similarities in social, biological, and cognitive attributes should also be reflected in the local architecture of white matter fascicles. Here we employ a method known as local connectome fingerprinting that uses diffusion MRI to measure the fiber-wise characteristics of macroscopic white matter pathways throughout the brain. This Citation: Powell, M. A., Garcia, J. O., fingerprinting approach was applied to a large sample (N = 841) of subjects from the Yeh, F.-C., Vettel, J. M., & Verstynen, T. (2017). Local connectome phenotypes Human Connectome Project, revealing a reliable degree of between-subject correlation in predict social, health, and cognitive factors. -

Proteomic Analysis of Postsynaptic Proteins in Regions of the Human Neocortex
Proteomic analysis of postsynaptic proteins in regions of the human neocortex Marcia Roy1*, Oksana Sorokina2*, Nathan Skene1, Clemence Simonnet1, Francesca Mazzo3, Ruud Zwart3, Emanuele Sher3, Colin Smith1, J Douglas Armstrong2 and Seth GN Grant1. * equal contribution Author Affiliations: 1. Genes to Cognition Program, Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh EH16 4SB, United Kingdom 2. School of Informatics, University of Edinburgh, Edinburgh, EH8 9AB, United Kingdom 3. Lilly Research Centre, Eli Lilly & Company, Erl Wood Manor, Windlesham, GU20 6PH, United Kingdom 1 Abstract: The postsynaptic proteome of excitatory synapses comprises ~1,000 highly conserved proteins that control the behavioral repertoire and mutations disrupting their function cause >130 brain diseases. Here, we document the composition of postsynaptic proteomes in human neocortical regions and integrate it with genetic, functional and structural magnetic resonance imaging, positron emission tomography imaging, and behavioral data. Neocortical regions show signatures of expression of individual proteins, protein complexes, biochemical and metabolic pathways. The compositional signatures in brain regions involved with language, emotion and memory functions were characterized. Integrating large-scale GWAS with regional proteome data identifies the same cortical region for smoking behavior as found with fMRI data. The neocortical postsynaptic proteome data resource can be used to link genetics to brain imaging and behavior, and to study the role of postsynaptic proteins in localization of brain functions. 2 Introduction: For almost two centuries, scientists have pursued the study of localization of function in the human cerebral neocortex using diverse methods including neuroanatomy, electrophysiology, imaging and gene expression studies. The frontal, parietal, temporal and occipital lobes of the neocortex have been commonly subdivided into Brodmann areas (BA)1 based on cytoarchitectural features, and specific behavioral functions have been ascribed to these regions. -

A Critical Look at Connectomics
EDITORIAL A critical look at connectomics There is a public perception that connectomics will translate directly into insights for disease. It is essential that scientists and funding institutions avoid misrepresentation and accurately communicate the scope of their work. onnectomes are generating interest and excitement, both among nervous system, dubbed the classic connectome because it is currently neuroscientists and the public. This September, the first grants the only wiring diagram for an animal’s entire nervous system at the level Cunder the Human Connectome Project, totaling $40 million of the synapse. Although major neurobiological insights have been made over 5 years, were awarded by the US National Institutes of Health using C. elegans and its known connectivity and genome, there are still (NIH). In the public arena, striking, colorful pictures of human brains many questions remaining that can only be answered by hypothesis-driven have accompanied claims that imply that understanding the complete experiments. For example, we still don’t completely understand the process connectivity of the human brain’s billions of neurons by a trillion synapses of axon regeneration, relevant to spinal cord injury in humans, in this is not only possible, but that this will also directly translate into insights comparatively simple system. Thus, a connectome, at any resolution, is for neurological and psychiatric disorders. Even a press release from only one of several complementary tools necessary to understand nervous the NIH touted that the Human Connectome Project would map the system disease and injury. wiring diagram of the entire living human brain and would link these There are substantial efforts aimed at generating connectomes for circuits to the full spectrum of brain function in health and disease. -

Download Download
NEUROSCIENCE RESEARCH NOTES OPEN ACCESS | EDITORIAL ISSN: 2576-828X From online resources to collaborative global neuroscience research: where are we heading? Pike See Cheah 1,2, King-Hwa Ling 2,3 and Eric Tatt Wei Ho 4,* 1 Department of Human Anatomy, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia. 2 NeuroBiology & Genetics Group, Genetics and Regenerative Medicine Research Centre, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia. 3 Department of Biomedical Sciences, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia. 4 Center for Intelligent Signal and Imaging Research, Universiti Teknologi PETRONAS, Perak, Malaysia. *Corresponding authors: [email protected]; Tel.: +60-5-368-7899 Published: 21 July 2020 https://doi.org/10.31117/neuroscirn.v3i3.51 Keywords: neuroinformatics; machine learning; bioinformatics; brain project; online resources; databases ©2020 by Cheah et al. for use and distribution in accord with the Creative Commons Attribution (CC BY-NC 4.0) license (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited. 1.0 INTRODUCTION The most visible contributions from neuroinformatics Neuroscience has emerged as a richly transdisciplinary include the myriad reference atlases of brain anatomy field, poised to leverage potential synergies with (human and other mammals such as rodents, primates information technology. To investigate the complex and pig), gene and protein sequences and the nervous system in its normal function and the disease bioinformatics software tools for alignment, matching state, researchers in the field are increasingly reliant and identification. Other neuroinformatics initiatives on generating, sharing and analyzing diverse data from include the various open-source preprocessing and multiple experimental paradigms at multiple spatial processing software and workflows for data analysis as and temporal scales (Frackowiak & Markram, 2015). -

Genetic and Environmental Influence on the Human Functional Connectome Andrew E
Cerebral Cortex, 2019;00: 1–15 doi: 10.1093/cercor/bhz225 Original Article Downloaded from https://academic.oup.com/cercor/advance-article-abstract/doi/10.1093/cercor/bhz225/5618752 by guest on 03 March 2020 ORIGINAL ARTICLE Genetic and Environmental Influence on the Human Functional Connectome Andrew E. Reineberg 1, Alexander S. Hatoum2, John K. Hewitt1,2, Marie T. Banich3 and Naomi P. Friedman1,2 1Institute for Behavioral Genetics, University of Colorado Boulder, Boulder, CO, 80309, USA, 2Department of Psychology and Neuroscience, University of Colorado Boulder, Boulder, CO, 80309, USA, and 3Institute of Cognitive Science, University of Colorado Boulder, Boulder, CO, 80309, USA Address correspondence to Andrew E. Reineberg, email: [email protected] http://orcid.org/0000-0002-0806-440X Abstract Detailed mapping of genetic and environmental influences on the functional connectome is a crucial step toward developing intermediate phenotypes between genes and clinical diagnoses or cognitive abilities. We analyzed resting-state functional magnetic resonance imaging data from two adult twin samples (Nos = 446 and 371) to quantify genetic and environmental influence on all pairwise functional connections between 264 brain regions (∼35 000 functional connections). Nonshared environmental influence was high across the whole connectome. Approximately 14–22% of connections had nominally significant genetic influence in each sample, 4.6% were significant in both samples, and 1–2% had heritability estimates greater than 30%. Evidence of shared environmental influence was weak. Genetic influences on connections were distinct from genetic influences on a global summary measure of the connectome, network-based estimates of connectivity, and movement during the resting-state scan, as revealed by a novel connectome-wide bivariate genetic modeling procedure. -

National Institute of Mental Health Strategic Plan for Research
NATIONAL INSTITUTE OF MENTAL HEALTH STRATEGIC PLAN FOR RESEARCH Table of Contents Table of Contents Message from the Director ............................................................................................................................................ 1 Overview of NIMH ......................................................................................................................................................... 3 Serving as an Efficient and Effective Steward of Public Resources ............................................................................... 5 Scientific Stewardship ............................................................................................................................................... 5 Management and Accountability .............................................................................................................................. 7 Accomplishing the Mission ............................................................................................................................................ 9 Challenges and Opportunities ..................................................................................................................................... 10 Suicide Prevention................................................................................................................................................... 10 Early Intervention in Psychosis ............................................................................................................................... -

Connectome Imaging for Mapping Human Brain Pathways
OPEN Molecular Psychiatry (2017) 22, 1230–1240 www.nature.com/mp EXPERT REVIEW Connectome imaging for mapping human brain pathways Y Shi and AW Toga With the fast advance of connectome imaging techniques, we have the opportunity of mapping the human brain pathways in vivo at unprecedented resolution. In this article we review the current developments of diffusion magnetic resonance imaging (MRI) for the reconstruction of anatomical pathways in connectome studies. We first introduce the background of diffusion MRI with an emphasis on the technical advances and challenges in state-of-the-art multi-shell acquisition schemes used in the Human Connectome Project. Characterization of the microstructural environment in the human brain is discussed from the tensor model to the general fiber orientation distribution (FOD) models that can resolve crossing fibers in each voxel of the image. Using FOD-based tractography, we describe novel methods for fiber bundle reconstruction and graph-based connectivity analysis. Building upon these novel developments, there have already been successful applications of connectome imaging techniques in reconstructing challenging brain pathways. Examples including retinofugal and brainstem pathways will be reviewed. Finally, we discuss future directions in connectome imaging and its interaction with other aspects of brain imaging research. Molecular Psychiatry (2017) 22, 1230–1240; doi:10.1038/mp.2017.92; published online 2 May 2017 INTRODUCTION These rich resources in connectome imaging present great Mapping the connectivity of brain circuits is fundamentally opportunities to map human brain pathways at unprecedented 22,23 important for our understanding of the functions of human brain. accuracy. On the other hand, this avalanche of BIG DATA in 24,25 Various neurological and mental disorders have been linked to the connectomics also poses challenges for existing image disruption of brain connectivity in circuits such as the cortico– analysis algorithms. -

A Distributed Brain Network Predicts General Intelligence from Resting-State Human Neuroimaging Data
bioRxiv preprint doi: https://doi.org/10.1101/257865; this version posted January 31, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. A distributed brain network predicts general intelligence from resting-state human neuroimaging data 1,4 5 1,3 1,2,3 Julien Dubois , Paola Galdi , Lynn K. Paul , Ralph Adolphs 1 Division of Humanities and Social Sciences, California Institute of Technology, Pasadena CA 91125, USA 2 Division of Biology and Biological Engineering, California Institute of Technology, Pasadena CA 91125, USA 3 Chen Neuroscience Institute, California Institute of Technology, Pasadena CA 91125, USA 4 Department of Neurosurgery, Cedars-Sinai Medical Center, Los Angeles, CA 90048, USA 5 Department of Management and Innovation Systems, University of Salerno, Fisciano, Salerno, Italy Correspondence: Julien Dubois Department of Neurosurgery Cedars-Sinai Medical Center, Los Angeles, CA 90048 [email protected] bioRxiv preprint doi: https://doi.org/10.1101/257865; this version posted January 31, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Abstract Individual people differ in their ability to reason, solve problems, think abstractly, plan and learn. A reliable measure of this general ability, also known as intelligence, can be derived from scores across a diverse set of cognitive tasks. There is great interest in understanding the neural underpinnings of individual differences in intelligence, since it is the single best predictor of long-term life success, and since individual differences in a similar broad ability are found across animal species. -

Ome Sweet Ome: What Can the Genome Tell Us About the Connectome? Jeff W Lichtman and Joshua R Sanes
Available online at www.sciencedirect.com Ome sweet ome: what can the genome tell us about the connectome? Jeff W Lichtman and Joshua R Sanes Some neuroscientists argue that detailed maps of synaptic however, the idea of applying an ‘omics-scale’ approach to connectivity – wiring diagrams – will be needed if we are to neural circuit tracing will require considerable vetting. understand how the brain underlies behavior and how brain Here, in contrast to common practice in this journal, we malfunctions underlie behavioral disorders. Such large-scale take the charge of providing our current opinion seriously. circuit reconstruction, which has been called connectomics, We compare and contrast connectomics with genomics to may soon be possible, owing to numerous advances in ask whether mapping neural connections could ulti- technologies for image acquisition and processing. Yet, the mately have the same kind of value as sequencing genes. community is divided on the feasibility and value of the enterprise. Remarkably similar objections were voiced when A (very) short history of connectomics the Human Genome Project, now widely viewed as a success, As with almost everything in neuroscience, the idea of was first proposed. We revisit that controversy to ask if it holds mapping circuits can be traced back to Cajal. He enun- any lessons for proposals to map the connectome. ciated both the neuron doctrine and the law of dynamic polarization [1]. These two ideas, along with Sherrington’s Address electrophysiological analysis of reflexes, provided the Department of Molecular and Cellular Biology and Center for Brain rationale for thinking about brain mechanisms in terms Science, Harvard University, Cambridge, MA 02138, USA of circuits: Neurons were nodes that were electrically Corresponding author: Lichtman, Jeff W ([email protected]) and connected to each other via two types of wires, axons Sanes, Joshua R ([email protected]) and dendrites.