2007-08 Front Cover.Pub
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The Conversion of Holloway Sanatorium
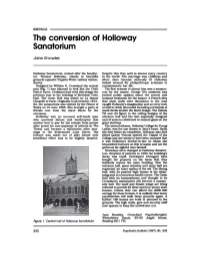
BRIEFINGS The conversion of Holloway Sanatorium Jane Knowles Holloway Sanatorium, named after the benefac Despite this they sold in almost every country tor, Thomas Holloway, stands in beautiful in the world. The marriage was childless and grounds opposite Virginia Water railway station, when Jane became seriously ill Holloway Surrey. looked around for philanthropic schemes to Designed by William H. Grassland the central commemorate her life. part (Fig. 1) was planned to look like the Cloth The first scheme to attract him was a sanator Hall at Ypres. Grassland had tried this design the ium for the insane. George Ill's madness had previous year in the building of Rochdale Town excited public opinion about the correct and Hall. The Great Hall was based on La Sainte humane treatment for the insane. A French idea Chapelle in Paris. Originally built between 1873- that plain walls were obnoxious to the mad 84, the sanatorium was opened by the Prince of caught Holloway's imagination and so every inch Wales on 15 June 1885, who brought a party of of wall is richly decorated including portrayals of friends over from the Ascot Races for the small devils amidst the florid design. The initials ceremony. TH and JH figure in the ceiling designs of the Holloway was an unusual self-made man entrance hall and his own especially designed who survived failure and bankruptcy (his coat of arms is celebrated in stained glass on the mother had to pay for his release from prison great stairway. after arrest for non-payment of adverts in The The second scheme, Holloway College for Young Times) and became a millionaire after niar- Ladies, was the one closest to Jane's heart. -

A the Grange Virginia Park, Virginia Water, Surrey, GU25 4ST 12 a the Grange Virginia Park, Virginia Water, Surrey, GU25 4ST
12 A THE GRANGE Virginia Park, Virginia Water, Surrey, GU25 4ST 12 A THE GRANGE Virginia Park, Virginia Water, Surrey, GU25 4ST Spacious elegance at the top of the building Windsor 7 miles, Ascot 5 miles, Central London 28 miles, M25 (J13) 3 miles (distances approximate) Reception hall ◆ Sitting room ◆ Kitchen/breakfast room Master bedroom with luxury en-suite bathroom ◆ Guest bedroom with en-suite bathroom ◆ Bedroom three/study ◆ Family shower room ◆ Secure underground parking for three cars ◆ Secure underground storage unit ◆ 24 Hour security ◆ Leisure facility Situation room beautifully bright and light. The guest bedroom has a good range of Virginia Park is a prestigious private gated estate built around the former built in wardrobes with hanging and shelving and an en-suite bathroom. Holloway Sanatorium, a magnificent Gothic building, now Grade I listed, Bedroom three is currently configured as a study with a range of custom in the heart of Virginia Water. The walled estate boasts 24 hour manned built furniture, ideal for use as a home office. Adjacent to this room is security, extensive leisure facilities including a fantastic indoor swimming a shower room. There are two very useful storage cupboards within the pool with Jacuzzi and sauna, well equipped gym and tennis court. apartment and a very large walk in airing cupboard. Within easy walking distance of Virginia Water Village Centre with its Immaculately presented throughout and featuring quality wood excellent shops for day to day needs, restaurants and mainline railway flooring, the apartment is ready for immediate occupation. station with fast service of trains to Waterloo in 42 minutes. -
Object-Index.Pdf
MC1 RHC operating table. ? date 7 during 1939-1945 war - RHC part used as war hospital MC2 Cooper recording on tape. ? contents MC3 Alf Turner recording on tape 1977 MC4 Alf Turner recording on tape 1977 MC5 Alf Turner recording on tape 1977 MC6 Roy Selfe recording on tape, from EBRHS Christmas Social ? Date MC7 RHC Chapel recording on tape. Sunday Half hour, radio programme 1984 MC8 Simmonds Inn Sign. Used as ‘temporary’ sign c 1936-1950 MC9 Burgords, Egham High Street. Vehicle oil lamp from horse drawn vehicle MC10 Sunningdale. St Agnes Church Communion Rail MC11 Egham. Bag of assorted nails. Pre 1979 MC12 Epsom Air Raid Whistle. Blown in short blasts for air raid warning MC13 Tittenhurst, Sunningdale. Plaster Moulding ( Thomas Holloway’s house ) MC14 Sunningdale. St Agnes Church: Hassocks MC15 Sunningdale. St Agnes Church: Altar MC16 Sunningdale. St Agnes Church: Collection Bag-leather MC17 Sunningdale. St Agnes Church: Hassock MC18 Egham High Street. C\1llens_ String container MC19 Children’s Rag Book. ‘What is this?, What is that? MC20 . Handcuffs. No keys! MC21 Tailors shears MC22 Virginia Water. Christchurch. Church pew MC23 Tin of malted slippery elm food for invalids ? date MC24 Holloway’s pill box MC25 Holloway Sanatorium wall plaque 1951 MC26 Egham Fire Brigade plaque ? plastic MC27 Holloway Sanatorium dessert spoon- engraved on handle MC28 Sunningdale. St Agnes Church: Wafer Box MC29 Sunningdale. St Agnes Church: Pulpit Light MC30 Sunningdale. St Agnes Church: Belfrey Cover MC31 Sunningdale. St Agnes Church: Notice Board MC32 Egham. Manorcrofts field. Clay Pipe MC33 Runnymede Pageant Cine Film 1934 MC34 Perfume Bottle in Box. -

Scrrey. Egham
D1REGTORY .J SCRREY. EGHAM. 171 TERRITORIAL FORCE. Wesleyan, Egham (Chertsey & \Valton-on-1 Thames Circuit), ll a.m. & 6.30 p.m.; 6th Battalion, East Sarrey Regiment (H Co. ), The In.~titute, tues. 8.15 p.m. 2nd Lieut. J. C. Eales-\Vhite; Sergt. Frederirk H. O:lker, Rev. J. Simpson" Wesleyan, Englefield Green (Chertsey & Hall drill instructor • Walton-on-Thames Circuit), ll a.m. & PrBLIC OFFICERS. 6.30 p.m. ; wed. 7 p.m. Salvation Army (The), Station road., U a.m. 3 & 6.45 p.:rn. ~ Assessor of Income & Property Tax, Henry Rowland, 44 mon. & thurs. 8 p.m Strode street The Brethren, Hummer road., 6.30 p.m Collector of Taxes & Clerk to Egha.m Sub-Committee of Surrey SCHOOLS. Local Pension O:lmmittRe, Arthur George Hutchins,Station rd Deputy Coroner for Guildford District, A. Dallas Brett, 23 Surrey County O:luncil Technical Institute, Egha.m HiJJ; ' Stati0n road erected 1905 Medical Officer & Public Vaccinator, Egham District, Windsor Public Elementary Schools. Union & No. 6 District, Chertsey Union, William \Vadham The schools are controlled by 9 manager&; A. Dallas Brett,. Floyer M. B. High street solicitor, Egham, clerk to the managers; Thomas Henry Registrar of Births, Deaths & Marriages for the Egham Peck, Lit~ra.ry Institute, Egham, attendance officer Sub-District, William Henry Gardener, High street; deputy,) Hythe, built in 1886, eniarged in 1890 & agajn in 1900 &. George Gardener, \Voolston house, Manor Crofts road 1912, for 900 children; average attendanc<>, 275 boys, 256 Relieving Officer for the Egha.m & part of Windsor Union, g4ls & 170 infants; L. H. -
What's on 2015-16
What’s On 2015-16 a guide to events at Royal Holloway Welcome I am delighted to introduce our programme of events at Royal Holloway for the year 2015-2016. Royal Holloway is one of the UK’s leading research intensive universities, founded by two Victorian social pioneers who understood the importance of education and knowledge, and who were inspired to bring those benefits to everyone. Today the College is a community that continues to be inspired by the egalitarian spirit of our founders; we are passionate about the personal and social values that come from education and knowledge. The College is a powerful force in the region, building partnerships with the business community and playing a major role in economic success. We are proud of the contribution we make to the cultural and social life of our community, by providing a wide range of events that cover the arts and humanities, science and social sciences. The new academic year sees the School of Law welcoming our first cohort of students on the LLB qualifying law degree, as well as our MSc in Forensic Psychology. Building on existing strength in criminology, social policy, sociology and forensic psychology, the new School of Law is home to a multidisciplinary team of research-active academics. On 29 February, the lecture on the 'Good Prison' Redefined – the Mandela Rules by Nick Hardwick, Her Majesty’s Chief Inspector of Prisons, will launch the School of Law. You are warmly invited to this event. Our impressive keynote lecture series provides an opportunity to hear directly from outstanding speakers, both internal and external. -

Photograph Index
PHOTOGRAPHS P 1 Runnymede Pageant - The Beggar Maid and Ladies of the Court - Henry VIII Scene 2 Runnymede Pageant - The Sealing of Magna Carta 3 Egham High Street - View of building : T Warriner - Fly Proprietor - Luxford & Ball - Fruiterers and Florists 1912 4 Staines High Street (Morford & Goodman) original B/W postcard c1906 5 Staines High Street - B/W postcard 6 Staines High Street - Town Hall 7 Staines High Street - St Peters Church 8 Staines High Street - Market Place and Town Hall - Janes & Son advert on Bus 9 Egham Hythe Bungalows 10 Staines High Street c1916 11 Staines High Street c1916 12 Staines High Street 13 Congregation Chapel, Staines 14 Staines Railway Station LSWR - Down steam train entering platform c1912 15 Staines High Street and Windsor Castle 16 Staines Bridge looking upstream by FF&Co (Francis Frith?) 17 Egham Hythe - bungalow cottages and The Swan looking east 18 Englefield Green - RHC - View through gates to clock tower 19 Staines Church Street 20 Three photographs of fallen mulberry tree in Fairhaven, August 1990 21 Great Fosters - view down drive to front 22 Staines - Victoria Gardens 23 Englefield Green - Engraving of Monte Rey by W Alexander from a sketch taken on the spot by J Sykes of EG (Castle Hill) 24 Egham Literary Institute, 1942 (National Monuments Record) 25 Thorpe - Air photograph of floods 1946/7 26 Egham, The Glanty - The Victoria inn on left - The Coach & Horses on right distance - view looking east 27 Egham High Street - View to east - Liberal Club on right - Denham House in background (junction -

Royal Holloway Chapel the Chapel
Royal Holloway Chapel The Chapel The Chapel at Royal Holloway, University of London is one of the highlights of the magnificent Founder’s Building. As you look at the monumental clock tower front from the main gates, the Chapel forms the left hand wing of the Founder’s Building front under the clock tower while the right hand wing contains the Picture Gallery. Thomas Holloway employed William Henry Crossland (1835-1908) to design the Renaissance Revival building, based on the Chateau de Chambord in France. Construction began in 1874 and was finished in 1881 but the College was not formally inaugurated by Queen Victoria until 1886. Something of a puzzle College chapels were a central feature of the Oxford and Cambridge Colleges. Since medieval times, the daily life of the staff and students who were mostly resident, revolved around the chapel, the refectory and the library and were closely connected to the Church of England. However, University College, London and Bedford College for Women, with their strong non- conformist connections had neither chapels nor chaplains. Royal Holloway’s Chapel is usually attributed to the inspiration of Jane Holloway, Thomas’s wife, at whose suggestion first the Holloway Sanatorium and then the College were founded. In the College’s original statutes, the day was to begin with ‘a simple service of readings, prayers and hymns of a Christian household’ that suggest the evangelical piety of Jane. However the size, the grand design and gilded interior of the Chapel are much more reminiscent of the Chapel of the Palace of Versailles than that of an English non-conformist domestic Victorian puginesque decoration on the walls chapel, and with more than a hint of Renaissance Catholic taste. -

Chertsey Division
County of Surrey CHERTSEY DIVISION Register of Electors, 1918 An Alphabetical Index of Naval/Military and/or Absent Voters Surrey History Centre Reference: CC802/27/1 This document contains the names of individuals who were included in the 1918 Electoral Register for the Chertsey Parliamentary Division of Surrey, and who were recorded as being either Naval, Military and/or absent voters. Notes: Not all Naval/Military voters may have been correctly designated “NM” and not all absent voters may have been Naval/Military personnel, in which case their entries are highlighted in orange text. Red text denotes a possible error, or information derived from a different source, such as the 1919 Chertsey Electoral Register. This is particularly the case for the Parish of Bisley (Dii), because parts of the pages for this Parish are missing in the Electoral Register held at the Surrey History Centre. Entry Nos. 547-573, 578-628, 634-660, 794-812 & 825 are affected. Some individuals were killed in action, or otherwise died, in the period between when the Register was compiled and the cessation of hostilities in November 1918. Some voters may appear more than once. This Index is therefore intended only as a guide to further research and no guarantee of accuracy is given. Key to Parishes/Wards: A ............................................................ Byfleet I(ii) ................................................ Egham Hythe B(i) ................................................ West Byfleet J(i) ............................................... Virginia -

Front Cover.Pub
CLEANER, SAFER, GREENER Annual Report and Summary Accounts 2006/07 www.ashfordstpeters.nhs.uk TRUST VALUES PUTTING PEOPLE AT THE HEART OF EVERYTHING WE DO Striving for excellence Being open and honest Treating everyoneProviding with humanity patient andfocused respect care Developing and valuing Ensuring a safe, clean and caring environment teams and individuals Humanity - Respect - Caring Honesty - Safety - Excellence Ashford and St. Peter’s Hospitals NHS Trust n Ashford and St. Peter’s Hospitals NHS Trust Annual Report 2006/07 Cleaner, Safer, Greener - Five years of progress SECTION ONE This section provides an overview of the Trust, the area which it operates in and some key facts. It includes: Chairman’s Review Page 1-2 Chief Executive’s Review Page 1-3 Background to Ashford and St. Peter’s Page 1-4 & 1-5 Catchment Area Map Page 1-6 In 2005 Ashford and St. Peter’s was declared a three star NHS Trust. In 2006 the Healthcare Commission rated our clinical services as good. If you want to stay in touch with events and news from Ashford and St. Peter’s please send an e-mail to [email protected] or write to Communications, The Studio (SDU), St. Peter’s Hospital, Guildford Road, CHERTSEY, Surrey, KT16 0PZ www.ashfordstpeters.nhs.uk Section 1, Page 1-1 Ashford and St. Peter’s Hospitals NHS Trust Annual Report 2006/07 Cleaner, Safer, Greener - Five years of progress Chairman’s Review In 2006, I predicted a difficult year for the Trust. As it turned out the year was a combination of challenge, real achievement and strategic consideration for our future. -

The Friends of Chertsey Museum
The Friends of Chertsey Museum Registered Charity No 1075200 Annual Report and Accounts for the year ended 31 August 2018 Member of the British Association of Member Friends of Museums The Friends of Chertsey Museum Registered Charity No 107520 President Ian Pickford Honorary Life Members Amanda Toth née Devonshire (1998) Jocelyn Barker (1999) Victor Spink (1999) Helen Nelson-Jones (2003) Valerie Cumming (2004) Bob Greenland (2004) Carl Veakins (2004) Ronnie Fleming (2005) Andrew Pearson (2011) Sybil Leaver (2014) Lorna Dalgleish (2017) Christopher Norman (2017) The Friends of Chertsey Museum are a support group formed in 1994 to foster interest in Chertsey Museum and to provide the Curators with practical help. The Friends are governed by their constitution adopted at the inaugural meeting, as subsequently amended. General management and direction of the funds and affairs of The Friends are in the hands of the Committee elected at the annual general meeting. There were regular meetings of the Commit- tee during the year and the members of the Committee were as follows: Heather Graham Chair from 19 October 2017 Victor Spink Vice Chairman Richard Mason Treasurer Ron Bathurst Minutes Secretary Victoria Johnstone Membership Secretary Emma Warren Curator (ex officio) Carol Botterill Valerie Clark (from 19 October 2017) Christine Dunster Chair until 19 October 2017 Norma Kent Jim Knight Mags Thomas Richard Williams Heidi Dawley and Sally Turner (Assistant Curators and Education Officers) are Emma Warren alternates Bankers Barclays Bank plc, Chertsey Branch COIF Charities Deposit Fund Contact address: Chertsey Museum,The Cedars, 33 Windsor Street, Chertsey, Surrey KT16 8AT e-mail: [email protected] tel: 01932 565764 Cover photograpgh: Friends at Tunbridge Wells September 2017 Annual Report The year 2018 marks a number of anniversaries, notably the centenary of the end of the First World War and the centenary of the Representation of the People Act 1918 when some women were given the vote for the first time. -

Runnymede's Village Garden
Runnymede 2035 Locally-Led Garden Villages, Towns and Cities Longcross Garden Village Expression of Interest Bid Document July 2016 With support of Left Intentionally Blank Contents 1. Background & Local Context ...................................................................................... 1 2. Expression of Interest – Information Required .......................................................... 5 Project Objectives, Scale and Planning Status ............................................................... 5 Governance Proposals..................................................................................................23 Delivery .........................................................................................................................25 Appendix 1 – Letter of Support from Surrey Heath ........................................................30 Appendix 2 – Letter of Support to Surrey Heath ............................................................32 Appendix 3 – Response to Highways England on M25 SW Quadrant Study .................34 Appendix 4 – Local Growth Fund Bid for A320 ..............................................................37 Plan 2-1: Longcross North Green Infrastructure Plan ..................................................... 8 Plan 2-2: Longcross North Landscaping Plan................................................................. 9 Plan 2-3: Longcross North Access Plan ........................................................................10 Plan 2-4: Longcross North Land Use Plan.....................................................................11 -

Issue 48 Newsletter November 2011
Issue 48 Newsletter November 2011 The clocks have gone back, the fireworks have all been lit and now thoughts turn to Christmas. Well, fear not! We have tried to solve at least some of your present buying problems. Our 2012 calendar will soon be available and will make both an attractive and useful gift. See the back page for further details. As detailed on the back page, you may find a subscription renewal reminder in this issue. We hope that you will decide to continue to join us, but if we have sent a reminder in error, please let us know so we can amend our records. We hope you enjoy this latest copy of our newsletter and that we will see you very soon at one of our meetings. FORTHCOMING EVENTS 2011 2011 2012 The new year is fast approaching and Jeff is busy Thursday 17th November: Come and hear setting up our calendar with lots of interesting topics. The Peter Duplock from the London Bus dates to note in your diaries are : 19th January, 16th February, 15th March, 19th April, 17th May, 14th June, 12th Preservation Trust speak about the history of July, 6th September, 11th October, 8th November, and 6th the former Cobham Bus Museum and their December. Topics planned are: recent move to Brooklands Museum. St Mary’s a continuation of our exploration of Byfleet shops and a Day Centre, Stream Close, 8.15pm. possible extension up the road into West Byfleet. Byfleet Boat Club Thursday 8th December : Christmas Social. Nibbles and drinks, together with Mike Chatley Heath Semaphore Tower Webber's annual collection of new photographs St John’s church in West Byfleet will be celebrating its that the Society has come by.