Inside Knowledge: Get the Facts About Gynecologic Cancer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Reference Sheet 1
MALE SEXUAL SYSTEM 8 7 8 OJ 7 .£l"00\.....• ;:; ::>0\~ <Il '"~IQ)I"->. ~cru::>s ~ 6 5 bladder penis prostate gland 4 scrotum seminal vesicle testicle urethra vas deferens FEMALE SEXUAL SYSTEM 2 1 8 " \ 5 ... - ... j 4 labia \ ""\ bladderFallopian"k. "'"f"";".'''¥'&.tube\'WIT / I cervixt r r' \ \ clitorisurethrauterus 7 \ ~~ ;~f4f~ ~:iJ 3 ovaryvagina / ~ 2 / \ \\"- 9 6 adapted from F.L.A.S.H. Reproductive System Reference Sheet 3: GLOSSARY Anus – The opening in the buttocks from which bowel movements come when a person goes to the bathroom. It is part of the digestive system; it gets rid of body wastes. Buttocks – The medical word for a person’s “bottom” or “rear end.” Cervix – The opening of the uterus into the vagina. Circumcision – An operation to remove the foreskin from the penis. Cowper’s Glands – Glands on either side of the urethra that make a discharge which lines the urethra when a man gets an erection, making it less acid-like to protect the sperm. Clitoris – The part of the female genitals that’s full of nerves and becomes erect. It has a glans and a shaft like the penis, but only its glans is on the out side of the body, and it’s much smaller. Discharge – Liquid. Urine and semen are kinds of discharge, but the word is usually used to describe either the normal wetness of the vagina or the abnormal wetness that may come from an infection in the penis or vagina. Duct – Tube, the fallopian tubes may be called oviducts, because they are the path for an ovum. -

Ovarian Cancer and Cervical Cancer
What Every Woman Should Know About Gynecologic Cancer R. Kevin Reynolds, MD The George W. Morley Professor & Chief, Division of Gyn Oncology University of Michigan Ann Arbor, MI What is gynecologic cancer? Cancer is a disease where cells grow and spread without control. Gynecologic cancers begin in the female reproductive organs. The most common gynecologic cancers are endometrial cancer, ovarian cancer and cervical cancer. Less common gynecologic cancers involve vulva, Fallopian tube, uterine wall (sarcoma), vagina, and placenta (pregnancy tissue: molar pregnancy). Ovary Uterus Endometrium Cervix Vagina Vulva What causes endometrial cancer? Endometrial cancer is the most common gynecologic cancer: one out of every 40 women will develop endometrial cancer. It is caused by too much estrogen, a hormone normally present in women. The most common cause of the excess estrogen is being overweight: fat cells actually produce estrogen. Another cause of excess estrogen is medication such as tamoxifen (often prescribed for breast cancer treatment) or some forms of prescribed estrogen hormone therapy (unopposed estrogen). How is endometrial cancer detected? Almost all endometrial cancer is detected when a woman notices vaginal bleeding after her menopause or irregular bleeding before her menopause. If bleeding occurs, a woman should contact her doctor so that appropriate testing can be performed. This usually includes an endometrial biopsy, a brief, slightly crampy test, performed in the office. Fortunately, most endometrial cancers are detected before spread to other parts of the body occurs Is endometrial cancer treatable? Yes! Most women with endometrial cancer will undergo surgery including hysterectomy (removal of the uterus) in addition to removal of ovaries and lymph nodes. -

Updates in Uterine and Vulvar Cancer
Management of GYN Malignancies Junzo Chino MD Duke Cancer Center ASTRO Refresher 2015 Disclosures • None Learning Objectives • Review the diagnosis, workup, and management of: – Cervical Cancers – Uterine Cancers – Vulvar Cancers Cervical Cancer Cervical Cancer • 3rd most common malignancy in the World • 2nd most common malignancy in women • The Leading cause of cancer deaths in women for the developing world • In the US however… – 12th most common malignancy in women – Underserved populations disproportionately affected > 6 million lives saved by the Pap Test “Diagnosis of Uterine Cancer by the Vaginal Smear” Published Pap Test • Start screening within 3 years of onset of sexual activity, or at age 21 • Annual testing till age 30 • If no history of abnormal paps, risk factors, reduce screening to Q2-3 years. • Stop at 65-70 years • 5-7% of all pap tests are abnormal – Majority are ASCUS Pap-test Interpretation • ASCUS or LSIL –> reflex HPV -> If HPV + then Colposcopy, If – Repeat in 1 year • HSIL -> Colposcopy • Cannot diagnose cancer on Pap test alone CIN • CIN 1 – low grade dysplasia confined to the basal 1/3 of epithelium – HPV negative: repeat cytology at 12 months – HPV positive: Colposcopy • CIN 2-3 – 2/3 or greater of the epithelial thickness – Cold Knife Cone or LEEP • CIS – full thickness involvement. – Cold Knife Cone or LEEP Epidemiology • 12,900 women expected to be diagnosed in 2015 – 4,100 deaths due to disease • Median Age at diagnosis 48 years Cancer Statistics, ACS 2015 Risk Factors: Cervical Cancer • Early onset sexual activity • Multiple sexual partners • Hx of STDs • Multiple pregnancy • Immune suppression (s/p transplant, HIV) • Tobacco HPV • The human papilloma virus is a double stranded DNA virus • The most common oncogenic strains are 16, 18, 31, 33 and 45. -

About Ovarian Cancer Overview and Types
cancer.org | 1.800.227.2345 About Ovarian Cancer Overview and Types If you have been diagnosed with ovarian cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to start. ● What Is Ovarian Cancer? Research and Statistics See the latest estimates for new cases of ovarian cancer and deaths in the US and what research is currently being done. ● Key Statistics for Ovarian Cancer ● What's New in Ovarian Cancer Research? What Is Ovarian Cancer? Cancer starts when cells in the body begin to grow out of control. Cells in nearly any part of the body can become cancer and can spread. To learn more about how cancers start and spread, see What Is Cancer?1 Ovarian cancers were previously believed to begin only in the ovaries, but recent evidence suggests that many ovarian cancers may actually start in the cells in the far (distal) end of the fallopian tubes. 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 What are the ovaries? Ovaries are reproductive glands found only in females (women). The ovaries produce eggs (ova) for reproduction. The eggs travel from the ovaries through the fallopian tubes into the uterus where the fertilized egg settles in and develops into a fetus. The ovaries are also the main source of the female hormones estrogen and progesterone. One ovary is on each side of the uterus. The ovaries are mainly made up of 3 kinds of cells. Each type of cell can develop into a different type of tumor: ● Epithelial tumors start from the cells that cover the outer surface of the ovary. -
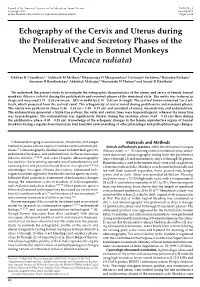
Echography of the Cervix and Uterus During the Proliferative and Secretory Phases of the Menstrual Cycle in Bonnet Monkeys (Macaca Radiata)
Journal of the American Association for Laboratory Animal Science Vol 53, No 1 Copyright 2014 January 2014 by the American Association for Laboratory Animal Science Pages 18–23 Echography of the Cervix and Uterus during the Proliferative and Secretory Phases of the Menstrual Cycle in Bonnet Monkeys (Macaca radiata) Uddhav K Chaudhari,1,* Siddnath M Metkari,2 Dhyananjay D Manjaramkar,2 Geetanjali Sachdeva,1 Rajendra Katkam,1 Atmaram H Bandivdekar,3 Abhishek Mahajan,4 Meenakshi H Thakur,4 and Sanjiv D Kholkute1 We undertook the present study to investigate the echographic characteristics of the uterus and cervix of female bonnet monkeys (Macaca radiata) during the proliferative and secretory phases of the menstrual cycle. The cervix was tortuous in shape and measured 2.74 ± 0.30 cm (mean ± SD) in width by 3.10 ± 0.32 cm in length. The cervical lumen contained 2 or 3 col- liculi, which projected from the cervical canal. The echogenicity of cervix varied during proliferative and secretory phases. The uterus was pyriform in shape (2.46 ± 0.28 cm × 1.45 ± 0.19 cm) and consisted of serosa, myometrium, and endometrium. The endometrium generated a triple-line pattern; the outer and central lines were hyperechogenic, whereas the inner line was hypoechogenic. The endometrium was significantly thicker during the secretory phase (0.69 ± 0.12 cm) than during the proliferative phase (0.43 ± 0.15 cm). Knowledge of the echogenic changes in the female reproductive organs of bonnet monkeys during a regular menstrual cycle may facilitate understanding of other physiologic and pathophysiologic changes. Ultrasound imaging is a noninvasive, atraumatic, and simple Materials and Methods method to assess various organs in humans and nonhuman pri- Animals and husbandry practices. -

Photodynamic Therapy for Gynecological Diseases and Breast Cancer
CancCancerer Biol Med 2012;2012 /9: Vol. 9-17 9 /doi: No. 10.3969/j.issn.2095-3941.2012.1 01.002 9 Review Photodynamic Therapy for Gynecological Diseases and Breast Cancer Natashis Shishkova, Olga Kuznetsova, Temirbolat Berezov Department of Biochemistry, School of Medicine, People’s Friendship University of Russia, Moscow 117198, Russia ABSTRACT Photodynamic therapy (PDT) is a minimally invasive and promising new method in cancer treatment. Cytotoxic reactive oxygen species (ROS) are generated by the tissue-localized non-toxic sensitizer upon illumination and in the presence of oxygen. Thus, selective destruction of a targeted tumor may be achieved. Compared with traditional cancer treatment, PDI has advantages including higher selectivity and lower rate of toxicity. The high degree of selectivity of the proposed method was applied to cancer diagnosis using fluorescence. This article reviews previous studies done on PDT treatment and photodetection of cervical intraepithelial neoplasia, vulvar intraepithelial neoplasia, ovarian and breast cancer, and PDT application in treating non-cancer lesions. The article also highlights the clinical responses to PDT, and discusses the possibility of enhancing treatment efficacy by combination with immunotherapy and targeted therapy. KEY WORDS: photodynamic therapy, photosensitizers, cervical/vulvar intraepithelial neoplasia, ovarian neoplasms, breast neoplasms Introduction frequently used drug in PDT is 5-aminolaevulinic acid (ALA). However, 5-ALA is not a photosensitizer, but a precursor of Photodynamic therapy (PDT) is a mode of therapy used in the endogenous photosensitizer protoporphyrin IX, which is cancer treatment where drug activity is locally controlled by a member of the heme synthesis pathway that occurs in the light (Figure 1). -

Vaginal and Vulvar Cancer 10.1136/Ijgc-2020-ESGO.178
Int J Gynecol Cancer: first published as 10.1136/ijgc-2020-ESGO.177 on 4 December 2020. Downloaded from Abstracts 520 LONG TERM FOLLOW UP AFTER DIAGNOSIS OF Introduction/Background Since the introduction of the S2K GESTATIONAL TROPHOBLASTIC DISEASE AWMF guideline-based sentinel node biopsy technique in uni- focal vulvar cancer (diameter of <4 cm) and unsuspicious Pedro Corvelo Freitas, Beatriz Mira, António Guimarães, Ana Opinião, Hugo Nunes, Ana Francisca Jorge, Fátima Vaz, António Moreira. Instituto Português de Oncologia de Lisboa groin lymph nodes, the morbidity rate of patients has signifi- Francisco Gentil cantly decreased in Germany. The groin recurrence rate after IFL is vary from 0% to 5.8%, in contrast to 2.3% (95% CI, 10.1136/ijgc-2020-ESGO.176 0.6% to 5%) in unifocal vulvar cancer vs 3% (95% CI, 1% to 6%) in multifocal vulvar cancer after SLNB only, as sug- Introduction/Background The spectrum of Gestational tropho- gested in the GRoningen INternational Study on Sentinel blastic disease (GTD) ranges from pre-malignant conditions of node in Vulvar cancer (GROINSS-V-I) in 2008. Current guide- complete (CHM) and partial (PHM) hydatidiform moles to the lines suggest that in cases of metastasis of unilateral sentinel malignant invasive mole, choriocarcinoma (CC) and very rare lymph node (SLN) biopsy (B), groin node dissection, namely placental site trophoblastic tumour/epithelioid trophoblastic inguinofemoral lymphadenectomy (IFL), should be performed tumour (PSTT/ETT). Gestational trophoblastic neoplasia (GTN) bilaterally. However, a publication by Woelber et al. in Ger- are highly responsive to chemotherapy (CT) and with appropri- many and and Nica et al. -

What Is New on Ovarian Carcinoma
diagnostics Review What Is New on Ovarian Carcinoma: Integrated Morphologic and Molecular Analysis Following the New 2020 World Health Organization Classification of Female Genital Tumors Antonio De Leo 1,2,3,*,† , Donatella Santini 3,4,† , Claudio Ceccarelli 1,3, Giacomo Santandrea 5 , Andrea Palicelli 5 , Giorgia Acquaviva 1,2, Federico Chiarucci 1,2 , Francesca Rosini 4, Gloria Ravegnini 3,6 , Annalisa Pession 2,6, Daniela Turchetti 3,7, Claudio Zamagni 8, Anna Myriam Perrone 3,9 , Pierandrea De Iaco 3,9, Giovanni Tallini 1,2,3,‡ and Dario de Biase 2,3,6,‡ 1 Department of Experimental, Diagnostic and Specialty Medicine, Alma Mater Studiorum—University of Bologna, Via Massarenti 9, 40138 Bologna, Italy; [email protected] (C.C.); [email protected] (G.A.); [email protected] (F.C.); [email protected] (G.T.) 2 Molecular Pathology Laboratory, IRCCS Azienda Ospedaliero—Universitaria di Bologna/Azienda USL di Bologna, 40138 Bologna, Italy; [email protected] (A.P.); [email protected] (D.d.B.) 3 Centro di Studio e Ricerca delle Neoplasie Ginecologiche, Alma Mater Studiorum—University of Bologna, 40138 Bologna, Italy; [email protected] (D.S.); [email protected] (G.R.); [email protected] (D.T.); [email protected] (A.M.P.); [email protected] (P.D.I.) 4 Pathology Unit, IRCCS Azienda Ospedaliero—Universitaria di Bologna, Via Massarenti 9, 40138 Bologna, Italy; [email protected] 5 Citation: De Leo, A.; Santini, D.; Pathology Unit, AUSL-IRCCS di Reggio Emilia, 42122 Reggio Emilia, Italy; Ceccarelli, C.; Santandrea, G.; [email protected] (G.S.); [email protected] (A.P.) 6 Palicelli, A.; Acquaviva, G.; Chiarucci, Department of Pharmacy and Biotechnology, University of Bologna, 40126 Bologna, Italy 7 Unit of Medical Genetics, IRCCS Azienda Ospedaliero—Universitaria di Bologna, Via Massarenti 9, F.; Rosini, F.; Ravegnini, G.; Pession, 40138 Bologna, Italy A.; et al. -
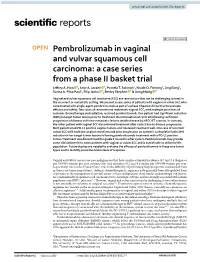
Pembrolizumab in Vaginal and Vulvar Squamous Cell Carcinoma: a Case Series from a Phase II Basket Trial Jefrey A
www.nature.com/scientificreports OPEN Pembrolizumab in vaginal and vulvar squamous cell carcinoma: a case series from a phase II basket trial Jefrey A. How 1, Amir A. Jazaeri 1, Pamela T. Soliman1, Nicole D. Fleming1, Jing Gong2, Sarina A. Piha‑Paul2, Filip Janku 2, Bettzy Stephen 2 & Aung Naing 2* Vaginal and vulvar squamous cell carcinoma (SCC) are rare tumors that can be challenging to treat in the recurrent or metastatic setting. We present a case series of patients with vaginal or vulvar SCC who were treated with single‑agent pembrolizumab as part of a phase II basket clinical trial to evaluate efcacy and safety. Two cases of recurrent and metastatic vaginal SCC, with multiple prior lines of systemic chemotherapy and radiation, received pembrolizumab. One patient had signifcant reduction (81%) in target tumor lesions prior to treatment discontinuation at cycle 10 following confrmed progression of disease with new metastatic lesions (stable disease by irRECIST criteria). In contrast, the other patient with vaginal SCC discontinued treatment after cycle 3 due to disease progression. Both patients had PD‑L1 positive vaginal tumors and tolerated treatment well. One case of recurrent vulvar SCC with multiple surgical resections and prior progression on systemic carboplatin had a 30% reduction in her target tumor lesions following pembrolizumab treatment with a PD‑L1 positive tumor. Treatment was discontinued for grade 3 mucositis after cycle 5. Pembrolizumab may provide some clinical beneft to some patients with vaginal or vulvar SCC and is overall safe to utilize in this population. Future studies are needed to evaluate the efcacy of pembrolizumab in these rare tumor types and to identify predictive biomarkers of response. -

Gynecological Malignancies in Aminu Kano Teaching Hospital Kano: a 3 Year Review
Original Article Gynecological malignancies in Aminu Kano Teaching Hospital Kano: A 3 year review IA Yakasai, EA Ugwa, J Otubu Department of Obstetrics and Gynecology, Aminu Kano Teaching Hospital, Kano and Center for Reproductive Health Research, Abuja, Nigeria Abstract Objective: To study the pattern of gynecological malignancies in Aminu Kano Teaching Hospital. Materials and Methods: This was a retrospective observational study carried out in the Gynecology Department of Aminu Kano Teaching Hospital (AKTH), Kano, Nigeria between October 2008 and September 2011. Case notes of all patients seen with gynecological cancers were studied to determine the pattern, age and parity distribution. Results: A total of 2339 women were seen during the study period, while 249 were found to have gynecological malignancy. Therefore the proportion of gynecological malignancies was 10.7%. Out of the 249 patients with gynecological malignancies, most (48.6%) had cervical cancer, followed by ovarian cancer (30.5%), endometrial cancer (11.25%) and the least was choriocarcinoma (9.24%). The mean age for cervical carcinoma patients (46.25 ± 4.99 years) was higher than that of choriocarcinoma (29 ± 14.5 years) but lower than ovarian (57 ± 4.5years) and endometrial (62.4 ± 8.3 years) cancers. However, the mean parity for cervical cancer (7.0 ± 3) was higher than those of ovarian cancer (3 ± 3), choriocarcinoma (3.5 ± 4) and endometrial cancer (4 ± 3). The mean age at menarche for women with cervical cancer (14.5 ± 0.71 years) was lower than for those with choriocarcinoma (15 ± 0 years), ovarian (15.5 ± 2.1 years) and endometrial (16 ± 0 years) cancers. -

Clinical Radiation Oncology Review
Clinical Radiation Oncology Review Daniel M. Trifiletti University of Virginia Disclaimer: The following is meant to serve as a brief review of information in preparation for board examinations in Radiation Oncology and allow for an open-access, printable, updatable resource for trainees. Recommendations are briefly summarized, vary by institution, and there may be errors. NCCN guidelines are taken from 2014 and may be out-dated. This should be taken into consideration when reading. 1 Table of Contents 1) Pediatrics 6) Gastrointestinal a) Rhabdomyosarcoma a) Esophageal Cancer b) Ewings Sarcoma b) Gastric Cancer c) Wilms Tumor c) Pancreatic Cancer d) Neuroblastoma d) Hepatocellular Carcinoma e) Retinoblastoma e) Colorectal cancer f) Medulloblastoma f) Anal Cancer g) Epndymoma h) Germ cell, Non-Germ cell tumors, Pineal tumors 7) Genitourinary i) Craniopharyngioma a) Prostate Cancer j) Brainstem Glioma i) Low Risk Prostate Cancer & Brachytherapy ii) Intermediate/High Risk Prostate Cancer 2) Central Nervous System iii) Adjuvant/Salvage & Metastatic Prostate Cancer a) Low Grade Glioma b) Bladder Cancer b) High Grade Glioma c) Renal Cell Cancer c) Primary CNS lymphoma d) Urethral Cancer d) Meningioma e) Testicular Cancer e) Pituitary Tumor f) Penile Cancer 3) Head and Neck 8) Gynecologic a) Ocular Melanoma a) Cervical Cancer b) Nasopharyngeal Cancer b) Endometrial Cancer c) Paranasal Sinus Cancer c) Uterine Sarcoma d) Oral Cavity Cancer d) Vulvar Cancer e) Oropharyngeal Cancer e) Vaginal Cancer f) Salivary Gland Cancer f) Ovarian Cancer & Fallopian -

Incidence and Cost of Anal, Penile, Vaginal and Vulvar Cancer in Denmark Jens Olsen1*, Tine Rikke Jørgensen2, Kristian Kofoed3 and Helle Kiellberg Larsen3
Olsen et al. BMC Public Health 2012, 12:1082 http://www.biomedcentral.com/1471-2458/12/1082 RESEARCH ARTICLE Open Access Incidence and cost of anal, penile, vaginal and vulvar cancer in Denmark Jens Olsen1*, Tine Rikke Jørgensen2, Kristian Kofoed3 and Helle Kiellberg Larsen3 Abstract Background: Besides being a causative agent for genital warts and cervical cancer, human papillomavirus (HPV) contributes to 40-85% of cases of anal, penile, vaginal and vulvar cancer and precancerous lesions. HPV types 16 & 18 in particular contribute to 74-93% of these cases. Overall the number of new cases of these four cancers may be relatively high implying notable health care cost to society. The aim of this study was to estimate the incidence and the health care sector costs of anal, penile, vaginal and vulvar cancer. Methods: New anogenital cancer patients were identified from the Danish National Cancer Register using ICD-10 diagnosis codes. Resource use in the health care sector was estimated for the year prior to diagnosis, and for the first, second and third years after diagnosis. Hospital resource use was defined in terms of registered hospital contacts, using DRG (Diagnosis Related Groups) and DAGS (Danish Outpatient Groups System) charges as cost estimates for inpatient and outpatient contacts, respectively. Health care consumption by cancer patients diagnosed in 2004–2007 was compared with that by an age- and sex-matched cohort without cancer. Hospital costs attributable to four anogenital cancers were estimated using regression analysis. Results: The annual incidence of anal cancer in Denmark is 1.9 per 100,000 persons. The corresponding incidence rates for penile, vaginal and vulvar cancer are 1.7, 0.9 and 3.6 per 100,000 males/females, respectively.