Our 20-Year Institutional Experience with Surgical Approach for Breast Hamartomas
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

35 Cyproterone Acetate and Ethinyl Estradiol Tablets 2 Mg/0
PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION PrCYESTRA®-35 cyproterone acetate and ethinyl estradiol tablets 2 mg/0.035 mg THERAPEUTIC CLASSIFICATION Acne Therapy Paladin Labs Inc. Date of Preparation: 100 Alexis Nihon Blvd, Suite 600 January 17, 2019 St-Laurent, Quebec H4M 2P2 Version: 6.0 Control # 223341 _____________________________________________________________________________________________ CYESTRA-35 Product Monograph Page 1 of 48 Table of Contents PART I: HEALTH PROFESSIONAL INFORMATION ....................................................................... 3 SUMMARY PRODUCT INFORMATION ............................................................................................. 3 INDICATION AND CLINICAL USE ..................................................................................................... 3 CONTRAINDICATIONS ........................................................................................................................ 3 WARNINGS AND PRECAUTIONS ....................................................................................................... 4 ADVERSE REACTIONS ....................................................................................................................... 13 DRUG INTERACTIONS ....................................................................................................................... 16 DOSAGE AND ADMINISTRATION ................................................................................................ 20 OVERDOSAGE .................................................................................................................................... -

A Study on Tumor Suppressor Genes Mutations Associated with Different Pppathologicalpathological Cccolorectalcolorectal Lllesions.Lesions
A Study on Tumor Suppressor Genes Mutations Associated with Different PPPathologicalPathological CCColorectalColorectal LLLesions.Lesions. Thesis Submitted for partial fulfillment of the requirements for the Ph.D. degree of Science in Biochemistry By Salwa Naeim Abd ElEl----KaderKader Mater M.Sc. in Biochemistry, 2002 Biological Applications Department Nuclear Research Center Atomic Energy Authority Under the supervision of Prof. Dr. Amani F.H Nour El ---Deen Prof. Dr. Abdel Hady Ali Abdel Wahab Professor of Biochemistry Professor of Biochemistry Biochemistry Department and Molecular Biology Faculty of Science Cancer Biology Department Ain Shams University National Cancer Institute Cairo University Prof. DrDr.MohsenMohsen Ismail Mohamed Dr. Azza Salah Helmy Professor of Clinical Pathology Biological Assistant Professor of Biochemistry Applications Department Biochemistry Department Nuclear Research Center Faculty of Science Atomic Energy Authority Ain Shams University 2012011111 ﺑﺴﻢ ﺍﷲ ﺍﻟﺮﺣﻤﻦ ﺍﻟﺮﺣﻴﻢ ﺇِﻧﻤﺎ ﺃﹶﻣﺮﻩ ﺇِﺫﹶﺍ ﺃﹶﺭﺍﺩ ﺷﻴﺌﹰﺎ ﺃﹶﹾﻥ ﻳﹸﻘﻮﻝﹶ ﻟﹶﻪ ﻛﹸـﻦ ﻓﹶﻴﻜﹸـﻮ ﻥ ﹸ ””” ٨٢٨٨٢٢٨٢““““ﻓﹶﺴﺒﺤﺎﻥﹶ ﺍﱠﻟﺬِﻱ ﺑِﻴﺪِﻩِ ﻣﻠﹶﻜﹸﻮﺕ ﻛﹸـﻞﱢ ﺷـﻲﺀٍ ﻭﺇِﻟﹶﻴـﻪِ ﺗﺮﺟﻌﻮﻥﹶ ””” ٨٣٨٨٣٣٨٣““““ ﺻﺪﻕ ﺍﷲ ﺍﻟﻌﻈﻴﻢ رة (٨٢-٨٣) I declare that this thesis has been composed by myself and the work there in has not been submitted for a degree at this or any other university. Salwa Naeim Abd El-Kader Matter To my dear husband and family Their love, encouragement and help made my studies possible and to them I owe everything. Thank you Salwa Naeim Abd El-Kader Matter Acknowledgement First of all, thanks to Allah the most merciful for guiding me and giving me the strength to complete this work. It is pleasure to express my deepest thanks and profound respect to Prof. -

Brain Tumors
Neuro-Pathology P a g e | 8 Brain Tumors Pathological finding Tumor Pseudorosette Ependymoma, SEGA Rosenthal fibers Pilocytic astrocytoma Rosettes Medulloblastoma Wet Keratin Craniopharyngioma Psammoma bodies Meningioma Fried egg Oligodendroglioma Medulloblastoma - Kids, midline, Cerebellum, diffuse contrast enhancement - Can seed in CSF (drop mets) but rarely involve meninges - On MRS, there is a choline and taurine peak Stains positive for Synaptophysin Rosettes formation Pilocytic astrocytoma: - Kids, cystic with an enhancing mural nodule. - Can occur in optic tract in patients with NF1 - Associated with BRAF gene mutation Pathology: Cells with long processes - Rosenthal fibers (intense red deposits formed of hyaline) Hair like processes arranged in Rosenthal fiber Smear of pilocytic cells bundles, resemble mats of hair Ahmed Koriesh, MD Neuro-Pathology P a g e | 9 SEGA: - In patients with TS (TSC1 in ch 9q34 and TSC2 in ch 16) Pathology: large polygonal cells with abundant eosinophilic cytoplasm, perivascular pseudo- rosettes GFAP H&E Oligodendroglioma: - Adults, lobar, associated with IDH mutation - Anaplastic (Grade III) associated with allelic loss at ch 1p and 19q Pathology shows rounded nuclei, prominent cytoplasm with clear halo (Fried egg) GFAB stain H&E Colloid cyst: - Usually arise in the 3rd ventricle close to the foramen of Monroe - MRI: isointense on T1, hyperintnse in T2 Pathology shows simple cuboidal or columnar epithelium, full of proteinaceous material Ahmed Koriesh, MD Neuro-Pathology P a g e | 10 Ependymoma: - Usually -
C O N F E R E N C E 22 27 April 2016
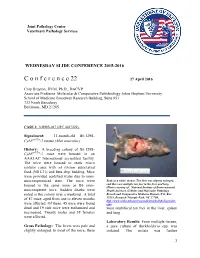
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2015-2016 C o n f e r e n c e 22 27 April 2016 Cory Brayton, DVM, Ph.D., DACVP Associate Professor, Molecular & Comparative Pathobiology Johns Hopkins University School of Medicine Broadway Research Building, Suite 851 733 North Broadway Baltimore, MD 21205 CASE I: NIEHS-087 (JPC 4017222). Signalment: 11-month-old B6.129S- Cybbtm1Din/J mouse (Mus musculus) History: A breeding colony of B6.129S- Cybbtm1Din/J mice were housed in an AAALAC International accredited facility. The mice were housed in static micro isolator cases with ad libitum autoclaved food (NIH-31) and beta chip bedding. Mice were provided acidified water due to imm- unocompromised state. The mice were Body as a while, mouse. The liver was slightly enlarged, housed in the same room as B6 imm- and there are multiple tan foci in the liver and lung. (Photo courtesy of: National Institute of Environmental unocompetent mice. Sudden deaths were Health Sciences, Cellular and Molecular Pathology noted in the colony over a weekend. A total Branch and Comparative Medicine Branch, P.O. Box of 87 mice, aged from one to eleven months 12233, Research Triangle Park, NC 27709, http://www.niehs.nih.gov/research/atniehs/labs/lep/index. were affected. Of these, 45 mice were found cfm) dead and 19 sick mice were euthanized and were multifocal tan foci in the liver, spleen necropsied. Twenty males and 38 females and lung. were affected. Laboratory Results: From multiple tissues, Gross Pathology: The livers were pale and a pure culture of Burkholderia spp. -

Understanding Your Pathology Report: Benign Breast Conditions
cancer.org | 1.800.227.2345 Understanding Your Pathology Report: Benign Breast Conditions When your breast was biopsied, the samples taken were studied under the microscope by a specialized doctor with many years of training called a pathologist. The pathologist sends your doctor a report that gives a diagnosis for each sample taken. Information in this report will be used to help manage your care. The questions and answers that follow are meant to help you understand medical language you might find in the pathology report from a breast biopsy1, such as a needle biopsy or an excision biopsy. In a needle biopsy, a hollow needle is used to remove a sample of an abnormal area. An excision biopsy removes the entire abnormal area, often with some of the surrounding normal tissue. An excision biopsy is much like a type of breast-conserving surgery2 called a lumpectomy. What does it mean if my report uses any of the following terms: adenosis, sclerosing adenosis, apocrine metaplasia, cysts, columnar cell change, columnar cell hyperplasia, collagenous spherulosis, duct ectasia, columnar alteration with prominent apical snouts and secretions (CAPSS), papillomatosis, or fibrocystic changes? All of these are terms that describe benign (non-cancerous) changes that the pathologist might see under the microscope. They do not need to be treated. They are of no concern when found along with cancer. More information about many of these can be found in Non-Cancerous Breast Conditions3. What does it mean if my report says fat necrosis? Fat necrosis is a benign condition that is not linked to cancer risk. -

Olanzapine-Induced Hyperprolactinemia: Two Case Reports
CASE REPORT published: 29 July 2019 doi: 10.3389/fphar.2019.00846 Olanzapine-Induced Hyperprolactinemia: Two Case Reports Pedro Cabral Barata *, Mário João Santos, João Carlos Melo and Teresa Maia Departamento de Psiquiatria, Hospital Prof. Dr. Fernando da Fonseca, EPE, Amadora, Portugal Background: Hyperprolactinemia is a common consequence of treatment with antipsychotics. It is usually defined by a sustained prolactin level above the laboratory upper level of normal in conditions other than that where physiologic hyperprolactinemia is expected. Normal prolactin levels vary significantly among different laboratories and studies. Several studies indicate that olanzapine does not significantly affect serum prolactin levels in the long term, although this statement has been challenged. Aims: Our aim is to report two olanzapine-induced hyperprolactinemia cases observed in psychiatric consultations. Methods: Medical records of the patients who developed this clinical situation observed Edited by: in psychiatric consultations in the Psychiatry Department of the Prof. Dr. Fernando Angel L. Montejo, Fonseca Hospital during the year of 2017 were analyzed, complemented with a non- University of Salamanca, Spain systematic review of the literature. Reviewed by: Carlos Spuch, Results: The case reports consider two women who developed prolactin-related Instituto de Investigación Sanitaria symptoms after the initiation of olanzapine. No baseline prolactinemia was obtained, and Galicia Sur (IISGS), Spain Lucio Tremolizzo, prolactin serum levels were only evaluated after prolactin-related symptoms developed: University of Milano-Bicocca, Italy at the time of its measurement, both patients had been taking olanzapine for more *Correspondence: than 24 weeks. Hyperprolactinemia was found to be present in Case 2, whereas Case Pedro Cabral Barata 1 (a 49-year-old woman) had “normal” serum prolactin levels for premenopausal and [email protected] prolactin levels slightly above the maximum levels for postmenopausal women. -

Diagnostic Approach to Soft Tissue Tumour of the Breast and Phyllodes Tumour in Ilorin, North Central with Review of Institutional Experience
World Journal of Medical Case Reports 2021; 2(3): 29-34 http://www.sciencepublishinggroup.com/j/wjmcr doi: 10.11648/j.wjmcr.20210203.11 Diagnostic Approach to Soft Tissue Tumour of the Breast and Phyllodes Tumour in Ilorin, North Central with Review of Institutional Experience Rasheed Mumini Wemimo 1, *, Afolayan Enoch Abiodun 1, Adegboye Adeyemi Taiwo 2 1Department of Pathology, University of Ilorin Teaching Hospital, Ilorin, Nigeria 2Mojitaiwo Data Services and Data Management Executives, Ilorin, Nigeria Email address: *Corresponding author To cite this article: Rasheed Mumini Wemimo, Afolayan Enoch Abiodun, Adegboye Adeyemi Taiwo. Diagnostic Approach to Soft Tissue Tumour of the Breast and Phyllodes Tumour in Ilorin, North Central with review of Institutional Experience. World Journal of Medical Case Reports. Vol. 2, No. 3, 2021, pp. 29-34. doi: 10.11648/j.wjmcr.20210203.11 Received : May 13, 2021; Accepted : June 7, 2021; Published : July 9, 2021 Abstract: Background: Primary soft tissue tumour (primary mesenchymal tumour) of the breast comprised of spectrum of neoplasm that arise from mammary stroma with comparable tumour biology of primary mesenchymal tumour at other sites. There are palpable diagnostic challenges which can be resolved by considering histomorphologic analysis that characterized each tumour entity regardless of the site and the use immunohistochemical markers. Methodology: This is an analytical hospital based retrospective study of patients with primary breast mesenchymal tumour and phyllodes diagnosed during 2014– 2019 at the Department of Pathology, University of Ilorin Teaching Hospital. The histopathological diagnosis of primary mesenchymal tumour of the breast and phyllodes tumours with documented age and other inclusion criteria were used for the study but excluded patients with incomplete information. -

Primary Breast Leiomyosarcoma and Synchronous Homolateral Lung Cancer: a Case Report
1059 Case Report Primary breast leiomyosarcoma and synchronous homolateral lung cancer: a case report Alberto Testori1, Stefano Meroni2, Emanuele Voulaz1, Marco Alloisio1, Rita De Sanctis3,4, Paola Bossi5, Umberto Cariboni1, Matilde De Simone6, Ugo Cioffi6 1General and Thoracic Surgery, Humanitas Research Hospital, Rozzano (Milan), Italy; 2Division of Breast Radiology, European Institute of Oncology, Milan, Italy; 3Department of Medical Oncology and Hematology, Humanitas Research Hospital, Rozzano (Milan), Italy; 4Molecular and Cellular Networks Lab, Department of Anatomy, Histology, Forensic Medicine and Orthopaedics, 'Sapienza' University, Rome, Italy; 5Department of Anatomo-Pathology, Humanitas Research Hospital, Rozzano (Milan), Italy; 6Department of Surgery, University of Milan, Milan, Italy Correspondence to: Alberto Testori, MD. General and Thoracic Surgery, Humanitas Research Hospital, Via Manzoni, 56, 20089 Rozzano (Milan), Italy. Email: [email protected]. Abstract: Radiological and histological features of breast leiomyosarcoma can mimic a wide variety of other breast lesions, such as mesenchymal tumors, breast lymphomas, poorly differentiated carcinomas and metaplastic breast carcinomas. The authors present the case of a 62-year-old woman with a primary breast leiomyosarcoma with synchronous ipsilateral lung adenocarcinoma. The latter was an incidental finding during pre-surgical staging examinations. Clinicopathological, immunophenotypic and imaging features cancer are described. A brief review of the literature on imaging findings and management of breast leiomyosarcoma is presented. The authors discuss the differential diagnoses in breast imaging and of the extra-mammary incidental findings. Surgical resection remains the cornerstone of treatment, while radiation therapy and chemotherapy remain to be defined on a single-patient basis. Keywords: Breast leiomyosarcoma; lung cancer; synchronous tumors Submitted May 14, 2017. -

Mesenchymoma of the Lung (So Called Hamartoma): a Review of 154 Parenchymal and Endobronchial Cases
Thorax: first published as 10.1136/thx.42.10.790 on 1 October 1987. Downloaded from Thorax 1987;42:790-793 Mesenchymoma of the lung (so called hamartoma): a review of 154 parenchymal and endobronchial cases J M M VAN DEN BOSCH, Sj Sc WAGENAAR, B CORRIN, J R J ELBERS, P J KNAEPEN, C JJ WESTERMANN From the Department ofPulmonary Disease, Pathology, and Cardiothoracic Surgery, St Antonius Hospital, Nieuwegein, The Netherlands, and the Department of Thoracic Pathology, Cardiothoracic Institute and Brompton Hospital, London ABSTRACT In a series of 154 patients (116 male and 38 female) with so called pulmonary hamartoma the peak incidence was in the sixth decade, with only three patients less than 20 years of age. Sequential radiographs showed that in 55 patients the tumour first appeared in adult life and that in 53 it progressively increased in size. The age incidence and progressive growth leads to the conclusion that the tumour is a benign neoplasm rather than a hamartoma, consisting of various connective tissues intersected by clefts lined by respiratory epithelium. The epithelial elements are regarded as entrapped non-neoplastic inclusions and the tumour as a purely mesenchymal neo- plasm: the name mesenchymoma therefore seems the most appropriate. There were two recurrences after simple enucleation, 10 and 12 years later. A total of 142 tumours were parenchymal, and only 12 were endobronchial. All lobes were affected but there was a slight preponderance in the left uppercopyright. lobe. Four patients had two (synchronous) mesenchymomas. There was an associated bronchial carcinoma in 11 patients, synchronous in six and metachronous in five. -

Case Presentation
Open Access Case Report DOI: 10.7759/cureus.2892 Nasal Chondromesenchymal Hamartoma with Skull Base and Orbital Involvement: Case Presentation Denis A. Golbin 1 , Anastasia P. Ektova 2 , Maxim O. Demin 3 , Nikolay Lasunin 4 , Vasily A. Cherekaev 1 1. Skull Base and Craniofacial Surgery, N.N. Burdenko National Medical Research Center for Neurosurgery, Moscow, RUS 2. Pathology, Russian Children's Clinical Hospital, Moscow, RUS 3. Pediatric Neurosurgery, N.N. Burdenko, Moscow, RUS 4. Neuro-Oncology, N.N. Burdenko National Medical Research Center for Neurosurgery, Moscow, RUS Corresponding author: Denis A. Golbin, [email protected] Abstract Nasal chondromesenchymal hamartoma (NCMH) is a rare benign tumor of the sinonasal tract in children with possible orbit and skull base involvement. We present the 57th published observation of this kind of tumor. A 25-month-old female patient presented with recurrent mass lesion of the sinonasal tract. According to her history, she had feeding difficulties and nasal obstruction since birth. She underwent partial resection at eight months of age via transfacial approach in the local hospital. Due to progression of tumor remnants, a second surgery was performed using an endoscopic endonasal approach resulting in subtotal resection. At 12 months of follow-up, a good postoperative result was observed with no signs of tumor progression despite incomplete resection. Histological and immunohistochemical examination of the biopsy specimens is presented. Comparison of specimens obtained from each of the two surgeries showed a difference in histological patterns. Endoscopic endonasal approach is the mainstay of surgical management. In case of incomplete resection, careful follow-up MRI studies should be recommended. -

BRAIN TUMORS Info Sheet
ROSWELL PARK COMPREHENSIVE CANCER CENTER BRAIN TUMORS Info Sheet FAST FACTS WHAT YOU SHOULD KNOW When cells in the brain grow and multiply out of control, they can form a tumor which may be malignant (cancerous) or benign (not cancerous). Roswell Park treats both malignant and benign tumors in the brain. Malignant brain tumors contain cancer cells and tend to grow rapidly and invade healthy brain tissue. Many of these are treatable and new therapies can help patients live longer and preserve quality of life. THERE ARE Benign brain tumors do not contain cancer cells. They rarely invade nearby MORE THAN tissue or spread to other parts of the body. Although a benign tumor is not DIFFERENT cancerous, it still needs treatment because it can press on the brain as it 120 TYPES OF grows in the skull. BRAIN TUMORS ARE YOU AT RISK? Brain tumors are relatively rare. They can occur at any age but are most Brain tumors common in children and older adults. You may have an increased risk for occur mostly in developing a brain tumor if you have one of these factors: children younger in adults Prior radiation treatment for other medical conditions such as leukemia. than older than Certain genetic conditions in your family. About 5% of brain tumors are linked to: 15 65 Neurofibromatosis Tuberous sclerosis & Von Hippel-Lindau disease Li-Frameni syndrome SYMPTOMS TO TELL YOUR DOCTOR The chance Persistent daily headaches of developing Changes in speech, vision or hearing a malignant Problems balancing or walking brain Changes in mood, personality or ability to concentrate tumor Confusion or difficulty with memory is LESS Muscle jerking or twitching THAN (seizures or convulsions) Numbness, weakness or 1% tingling in arms or legs 1-800-ROSWELL (1-800-767-9355) | RoswellPark.org If you have a brain tumor, WHY ROSWELL PARK FOR BRAIN TUMORS? you need a second opinion. -

NDA/BLA Multi-Disciplinary Review and Evaluation
NDA/BLA Multi-disciplinary Review and Evaluation NDA 214154 Nextstellis (drospirenone and estetrol tablets) NDA/BLA Multi-Disciplinary Review and Evaluation Application Type NDA Application Number(s) NDA 214154 (IND 110682) Priority or Standard Standard Submit Date(s) April 15, 2020 Received Date(s) April 15, 2020 PDUFA Goal Date April 15, 2021 Division/Office Division of Urology, Obstetrics, and Gynecology (DUOG) / Office of Rare Diseases, Pediatrics, Urologic and Reproductive Medicine (ORPURM) Review Completion Date April 15, 2021 Established/Proper Name drospirenone and estetrol tablets (Proposed) Trade Name Nextstellis Pharmacologic Class Combination hormonal contraceptive Applicant Mayne Pharma LLC Dosage form Tablet Applicant proposed Dosing x Take one tablet by mouth at the same time every day. Regimen x Take tablets in the order directed on the blister pack. Applicant Proposed For use by females of reproductive potential to prevent Indication(s)/Population(s) pregnancy Recommendation on Approval Regulatory Action Recommended For use by females of reproductive potential to prevent Indication(s)/Population(s) pregnancy (if applicable) Recommended Dosing x Take one pink tablet (drospirenone 3 mg, estetrol Regimen anhydrous 14.2 mg) by mouth at the same time every day for 24 days x Take one white inert tablet (placebo) by mouth at the same time every day for 4 days following the pink tablets x Take tablets in the order directed on the blister pack 1 Reference ID: 4778993 NDA/BLA Multi-disciplinary Review and Evaluation NDA 214154 Nextstellis (drospirenone and estetrol tablets) Table of Contents Table of Tables .................................................................................................................... 5 Table of Figures ................................................................................................................... 7 Reviewers of Multi-Disciplinary Review and Evaluation ...................................................