Primary Breast Leiomyosarcoma and Synchronous Homolateral Lung Cancer: a Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
C O N F E R E N C E 22 27 April 2016
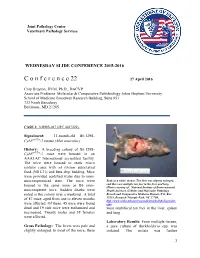
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2015-2016 C o n f e r e n c e 22 27 April 2016 Cory Brayton, DVM, Ph.D., DACVP Associate Professor, Molecular & Comparative Pathobiology Johns Hopkins University School of Medicine Broadway Research Building, Suite 851 733 North Broadway Baltimore, MD 21205 CASE I: NIEHS-087 (JPC 4017222). Signalment: 11-month-old B6.129S- Cybbtm1Din/J mouse (Mus musculus) History: A breeding colony of B6.129S- Cybbtm1Din/J mice were housed in an AAALAC International accredited facility. The mice were housed in static micro isolator cases with ad libitum autoclaved food (NIH-31) and beta chip bedding. Mice were provided acidified water due to imm- unocompromised state. The mice were Body as a while, mouse. The liver was slightly enlarged, housed in the same room as B6 imm- and there are multiple tan foci in the liver and lung. (Photo courtesy of: National Institute of Environmental unocompetent mice. Sudden deaths were Health Sciences, Cellular and Molecular Pathology noted in the colony over a weekend. A total Branch and Comparative Medicine Branch, P.O. Box of 87 mice, aged from one to eleven months 12233, Research Triangle Park, NC 27709, http://www.niehs.nih.gov/research/atniehs/labs/lep/index. were affected. Of these, 45 mice were found cfm) dead and 19 sick mice were euthanized and were multifocal tan foci in the liver, spleen necropsied. Twenty males and 38 females and lung. were affected. Laboratory Results: From multiple tissues, Gross Pathology: The livers were pale and a pure culture of Burkholderia spp. -

Diagnostic Approach to Soft Tissue Tumour of the Breast and Phyllodes Tumour in Ilorin, North Central with Review of Institutional Experience
World Journal of Medical Case Reports 2021; 2(3): 29-34 http://www.sciencepublishinggroup.com/j/wjmcr doi: 10.11648/j.wjmcr.20210203.11 Diagnostic Approach to Soft Tissue Tumour of the Breast and Phyllodes Tumour in Ilorin, North Central with Review of Institutional Experience Rasheed Mumini Wemimo 1, *, Afolayan Enoch Abiodun 1, Adegboye Adeyemi Taiwo 2 1Department of Pathology, University of Ilorin Teaching Hospital, Ilorin, Nigeria 2Mojitaiwo Data Services and Data Management Executives, Ilorin, Nigeria Email address: *Corresponding author To cite this article: Rasheed Mumini Wemimo, Afolayan Enoch Abiodun, Adegboye Adeyemi Taiwo. Diagnostic Approach to Soft Tissue Tumour of the Breast and Phyllodes Tumour in Ilorin, North Central with review of Institutional Experience. World Journal of Medical Case Reports. Vol. 2, No. 3, 2021, pp. 29-34. doi: 10.11648/j.wjmcr.20210203.11 Received : May 13, 2021; Accepted : June 7, 2021; Published : July 9, 2021 Abstract: Background: Primary soft tissue tumour (primary mesenchymal tumour) of the breast comprised of spectrum of neoplasm that arise from mammary stroma with comparable tumour biology of primary mesenchymal tumour at other sites. There are palpable diagnostic challenges which can be resolved by considering histomorphologic analysis that characterized each tumour entity regardless of the site and the use immunohistochemical markers. Methodology: This is an analytical hospital based retrospective study of patients with primary breast mesenchymal tumour and phyllodes diagnosed during 2014– 2019 at the Department of Pathology, University of Ilorin Teaching Hospital. The histopathological diagnosis of primary mesenchymal tumour of the breast and phyllodes tumours with documented age and other inclusion criteria were used for the study but excluded patients with incomplete information. -

Giant Juvenile Fibroadenoma of Breast
Journal of Surgical Sciences (2013) Vol. 17 (2) : 99-102 © 2012 Society of Surgeons of Bangladesh JOURNAL OF SURGICAL SCIENCES Case Report GIANT JUVENILE FIBROADENOMA OF BREAST 2 2 3 5 KABM Taiful Alam1, Toufiqul Haque , Shamim Hossain , Kuntal Das , Tazul lslam4, Helena Ahmed Abstract: Giant juvenile fibroadenoma occurs in adolescent girls. These tumours become enormous in size and grow rapidly, though these tumours are mostly benign. These patients are almost always treated by breast conserving surgery. Here we present a case having unilateral giant juvenile fibroadenoma with bilateral multiple small fibroadenomas in an adolescent female aged 16years. The diagnosis of the patient was made on clinical examination, USG & FNAC. Confirmatory diagnosis was made by histopathology. We removed the giant one with "Swiss-Roll" procedure and others by simple enucleation. The aesthatic appearence of the breasts were preserved. Key words: Fibroadenoma, Giant fibroadenoma, Juvenile fibroadenoma, Swiss-roll operation. Introduction: can grow to immense proportions, compressing and Fibroadenoma is the most common benign tumour of displacing normal breast tissue and stretching the 4 female breast.It usually arises in the fully developed overlying skin and nipple areola complex . breast during the 15-25 years age period. They arise from hyperplasia of both fibrous & glandular tissue of Case report: a single lobule & usually grow upto 2-3 cm in size. A 16 year old girl presented with bilateral breast lumps Juvenile fibroadenoma is a benign tumour which occurs for 1 year. There were multiple lumps in the both during puberty1. It is a rare clinical condition and forms breasts among them one lump in the left breast was 4% of the total fibroadenomes--'. -

Investigations of Breast Tumors Withfluorine
10. Pacini F, Gasperi M, Fugazzola L, et al. Testicular thyroid cancer: potential risks and recommendations. dent: temporal correlation or casual relation? Br MedJ function in patients with differentiated thyroid carci Ear J Nuc! Med I993:20:192—194. 1994:309:158—162. noma treated with radioiodine. J Nucl Med 1994:35: 23. Dottorini ME, Lomuscio G, Mazzucchelli L, Vignati 34. Harjuletho T, Aro T, Rita H. Rytomaa T, SaxénL. The 1418 —1422. A, Colombo L. Assessment of female fertility and accident at Chernobyl and outcome of pregnancy in 11. Brincker H, Hansen HS, Andersen AP. Induction of carcinogenesis after iodine-I 3 1 therapy for differenti Finland. Br Med J I989:288:995—997. leukaemia by ‘@‘Itreatment ofthyroid carcinoma. BrJ ated thyroid carcinoma. J Nod Med 1995:36:21—27. 35. Bertollini R, Di Lallo D. Mastroiacovo P. Perucci CA. Cancer 1973:28:232—237. 24. Schlumberger M, Dc Vathaire F. Ceccarelli C, et al. Reduction of births in Italy after the Chemobyl acci 12. Hall P. HoIm LE, Lundell G. et al. Cancer risks in Exposure to radioactive iodine for scintigraphy or dent. Scandi Work Environ Health 1990:16:96—101. thyroid cancer patients. Br J Cancer 1991:64:159—163. therapy does not preclude pregnancy in thyroid cancer 36. Hawkins MM, Draper Gi, Winter DL. Cancer in the patients. J Nucl Med 1996:37:606—612. 13. Sobels FH. Estimation of the genetic risk resulting offspring of survivors of childhood leukemia and 25. Izembart M, Chavaudra J, Aubert B, ValléeG. Retro @ from the treatment of women with ‘I. -

Management of Fibroadenomas of the Breast
- Official Statement - Management of Fibroadenomas of the Breast Fibroadenoma of the breast is a common benign lesion affecting women during their reproductive years. Despite their benignity, fibroadenomas can cause physical deformity due to large size and may produce discomfort or emotional distress in affected individuals. The traditional management options available to women diagnosed with a fibroadenoma include observation or surgical excision. Two newer approaches, percutaneous excision and in situ cryoablation, have been developed and are less invasive than surgical excision. The purpose of this consensus statement is to put these four management options into perspective for our members and their patients. In most patients with fibroadenoma(s), the ideal approach is confirmation with percutaneous core biopsy and conservative follow-up. Because the malignant potential of fibroadenomas is extremely low, treatment is not required on an oncologic basis. This conservative approach is the least costly in terms of dollars and morbidity. A significant minority of fibroadenomas will disappear without treatment; with the remaining lesions either increasing in size or remaining unchanged. Because fibroadenomas can be bothersome to some patients, causing physical deformity, discomfort or emotional distress, most breast surgeons will respect an informed patient's preference for treatment. Traditional open excisional biopsy is effective treatment in such cases but it is the most costly option because of the operating room charges and time off from work. Open excision may still be the best option in some cases based on large size of the fibroadenoma or the judgment of the surgeon or patient preference. Studies have shown that ultrasound guided percutaneous excision of fibroadenomas is safe, effective and well tolerated by patients. -

Pleomorphic Liposarcoma of the Male Breast: Lessons from a Rare
Case report BMJ Case Rep: first published as 10.1136/bcr-2021-244056 on 20 July 2021. Downloaded from Pleomorphic liposarcoma of the male breast: lessons from a rare malignancy during COVID-19 pandemic Brijesh Kumar Singh ,1 Manjunath Maruti Pol ,1 Toshib G A,1 Adarsh Wamanrao Barwad2 1Surgery, All India Institute of SUMMARY mobility over the chest wall. The nipple, areola and Medical Sciences, New Delhi, A 52-year -old man presented with a recurrent right side overlying skin were not involved. The contralateral India breast examination was unremarkable. There was 2 breast lump. He had undergone excision of a lump on Department of Pathology, the right breast followed by adjuvant chemoradiotherapy no clinically palpable axillary and supraclavicular All India Institute of Medical 1 year ago for a diagnosis of pleomorphic liposarcoma. lymph nodes. Sciences, New Delhi, India Imaging revealed a 47×36 mm lesion on the right side of the chest wall involving the pectoralis muscle. The Correspondence to INVESTIGATIONS patient underwent right radical mastectomy. Histology of Dr Manjunath Maruti Pol; Biopsy of the lump yielded focal chronic inflamma- manjunath. pol@ gmail. com the specimen showed an undifferentiated pleomorphic tion with few foamy macrophages. In view of high sarcoma infiltrating into the underlying skeletal muscle. suspicion of recurrence, contrast- enhanced CT Accepted 21 June 2021 Therefore, he was planned for chemoradiotherapy. But of thorax and positron emission tomography and due to lockdown during the COVID-19 pandemic, he CT (PET- CT) were performed to stage the tumour was lost to follow-up and later presented with malignant and assess resectability. -

Non-Cancerous Breast Conditions Fibrosis and Simple Cysts in The
cancer.org | 1.800.227.2345 Non-cancerous Breast Conditions ● Fibrosis and Simple Cysts ● Ductal or Lobular Hyperplasia ● Lobular Carcinoma in Situ (LCIS) ● Adenosis ● Fibroadenomas ● Phyllodes Tumors ● Intraductal Papillomas ● Granular Cell Tumors ● Fat Necrosis and Oil Cysts ● Mastitis ● Duct Ectasia ● Other Non-cancerous Breast Conditions Fibrosis and Simple Cysts in the Breast Many breast lumps turn out to be caused by fibrosis and/or cysts, which are non- cancerous (benign) changes in breast tissue that many women get at some time in their lives. These changes are sometimes called fibrocystic changes, and used to be called fibrocystic disease. 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 Fibrosis and cysts are most common in women of child-bearing age, but they can affect women of any age. They may be found in different parts of the breast and in both breasts at the same time. Fibrosis Fibrosis refers to a large amount of fibrous tissue, the same tissue that ligaments and scar tissue are made of. Areas of fibrosis feel rubbery, firm, or hard to the touch. Cysts Cysts are fluid-filled, round or oval sacs within the breasts. They are often felt as a round, movable lump, which might also be tender to the touch. They are most often found in women in their 40s, but they can occur in women of any age. Monthly hormone changes often cause cysts to get bigger and become painful and sometimes more noticeable just before the menstrual period. Cysts begin when fluid starts to build up inside the breast glands. Microcysts (tiny, microscopic cysts) are too small to feel and are found only when tissue is looked at under a microscope. -

Aberrant DNA Methylation of Cancer-Related
Marzese et al. Journal of Medical Case Reports 2011, 5:516 JOURNAL OF MEDICAL http://www.jmedicalcasereports.com/content/5/1/516 CASE REPORTS CASE REPORT Open Access Aberrant DNA methylation of cancer-related genes in giant breast fibroadenoma: a case report Diego M Marzese1,2, Francisco E Gago2,3, Javier I Orozco2,3, Olga M Tello3, María Roqué1 and Laura M Vargas-Roig2,4* Abstract Introduction: Giant fibroadenoma is an uncommon variant of benign breast lesions. Aberrant methylation of CpG islands in promoter regions is known to be involved in the silencing of genes (for example, tumor-suppressor genes) and appears to be an early event in the etiology of breast carcinogenesis. Only hypermethylation of p16INK4a has been reported in non-giant breast fibroadenoma. In this particular case, there are no previously published data on epigenetic alterations in giant fibroadenomas. Our previous results, based on the analysis of 49 cancer-related CpG islands have confirmed that the aberrant methylation is specific to malignant breast tumors and that it is completely absent in normal breast tissue and breast fibroadenomas. Case presentation: A 13-year-old Hispanic girl was referred after she had noted a progressive development of a mass in her left breast. On physical examination, a 10 × 10 cm lump was detected and axillary lymph nodes were not enlarged. After surgical removal the lump was diagnosed as a giant fibroadenoma. Because of the high growth rate of this benign tumor, we decided to analyze the methylation status of 49 CpG islands related to cell growth control. We have identified the methylation of five cancer-related CpG islands in the giant fibroadenoma tissue: ESR1, MGMT, WT-1, BRCA2 and CD44. -

New Jersey State Cancer Registry List of Reportable Diseases and Conditions Effective Date March 10, 2011; Revised March 2019
New Jersey State Cancer Registry List of reportable diseases and conditions Effective date March 10, 2011; Revised March 2019 General Rules for Reportability (a) If a diagnosis includes any of the following words, every New Jersey health care facility, physician, dentist, other health care provider or independent clinical laboratory shall report the case to the Department in accordance with the provisions of N.J.A.C. 8:57A. Cancer; Carcinoma; Adenocarcinoma; Carcinoid tumor; Leukemia; Lymphoma; Malignant; and/or Sarcoma (b) Every New Jersey health care facility, physician, dentist, other health care provider or independent clinical laboratory shall report any case having a diagnosis listed at (g) below and which contains any of the following terms in the final diagnosis to the Department in accordance with the provisions of N.J.A.C. 8:57A. Apparent(ly); Appears; Compatible/Compatible with; Consistent with; Favors; Malignant appearing; Most likely; Presumed; Probable; Suspect(ed); Suspicious (for); and/or Typical (of) (c) Basal cell carcinomas and squamous cell carcinomas of the skin are NOT reportable, except when they are diagnosed in the labia, clitoris, vulva, prepuce, penis or scrotum. (d) Carcinoma in situ of the cervix and/or cervical squamous intraepithelial neoplasia III (CIN III) are NOT reportable. (e) Insofar as soft tissue tumors can arise in almost any body site, the primary site of the soft tissue tumor shall also be examined for any questionable neoplasm. NJSCR REPORTABILITY LIST – 2019 1 (f) If any uncertainty regarding the reporting of a particular case exists, the health care facility, physician, dentist, other health care provider or independent clinical laboratory shall contact the Department for guidance at (609) 633‐0500 or view information on the following website http://www.nj.gov/health/ces/njscr.shtml. -

Sarcomas of the Breast: Findings on Mammography, Ultrasound, And
Matsumoto RAEKPictorial et al. / SarcomasEssay of the breast: imaging findings Sarcomas of the breast: findings on mammography, ultrasound, and magnetic resonance imaging Sarcomas da mama: achados mamográficos, ultrassonográficos e de ressonância magnética Renato Augusto Eidy Kiota Matsumoto1,a, Su Jin Kim Hsieh1,b, Luciano Fernandes Chala2,c, Giselle Guedes Netto de Mello2,d, Nestor de Barros1,e 1. Department of Radiology and Oncology, Faculdade de Medicina da Universidade de São Paulo (FMUSP), São Paulo, SP, Brazil. 2. Grupo Fleury, São Paulo, SP, Brazil. Correspondence: Dr. Renato Augusto Eidy Kiota Matsumoto. Rua Doutor Ovídio Pires de Campos, 75, Cerqueira César. São Paulo, SP, Brazil, 05403-010. Email: [email protected]. a. https://orcid.org/0000-0003-3631-5867; b. https://orcid.org/0000-0002-2645-2844; c. https://orcid.org/0000-0002-4888-5413; d. https://orcid.org/0000-0003-4123-3380; e. https://orcid.org/0000-0001-5806-8145. Received 4 August 2016. Accepted after revision 2 February 2017. How to cite this article: Matsumoto RAEK, Hsieh SJK, Chala LF, Mello GGN, Barros N. Sarcomas of the breast: findings on mammography, ultrasound, and magnetic resonance imaging. Radiol Bras. 2018 Nov/Dez;51(6):401–406. Abstract Sarcomas of the breast belong to a heterogeneous group of breast tumors of mesenchymal origin, without epithelial components. These tumors can be primary or secondary (after previous treatment for breast cancer), are rare, present aggressive behavior, and have a poor prognosis. They occur mainly in women between 45 and 50 years of age, with the exception of angiosarcomas, which can occur in younger patients. -

CD137 Expression in Tumor Vessel Walls High Correlation with Malignant Tumors
Anatomic Pathology / CD137 EXPRESSION IN TUMOR VESSEL WALLS CD137 Expression in Tumor Vessel Walls High Correlation With Malignant Tumors Karin Broll, Georg Richter, MD, Susanne Pauly, Ferdinand Hofstaedter, MD, and Herbert Schwarz, PhD Key Words: CD137; Blood vessel; Tumor Downloaded from https://academic.oup.com/ajcp/article/115/4/543/1758017 by guest on 28 September 2021 Abstract CD137 (ILA/4-1BB) is a member of the tumor necrosis CD137 (ILA/4-1BB), a member of the tumor factor receptor family.1 It was isolated from activated T necrosis factor receptor family, and its ligand are lymphocytes in mice and humans.2,3 While expression of expressed on activated T lymphocytes and on antigen- CD137 messenger RNA (mRNA) can be detected in all acti- presenting cells, respectively. Via bidirectional signal vated hematopoietic cells, expression of CD137 protein is transduction, this receptor-ligand system regulates the specific for T lymphocytes, implying a stringent posttran- activation, proliferation, and survival of T and B scriptional control for protein expression.4,5 lymphocytes and monocytes. We used Costimulation through CD137 enhances T-lymphocyte immunohistochemical studies on human tissue samples activation, comparable to costimulation through CD28, and to determine in vivo CD137 expression in nonimmune induces rejection of tumors in mice.6-8 The CD137 ligand is tissue samples. Strong CD137 expression was found in expressed by antigen-presenting cells, and bidirectional blood vessel walls, on the endothelial layer, and on the signaling has been demonstrated for CD137.9,10 Cross- vascular smooth muscle cells. But in 32 healthy tissue linking of the membrane-bound CD137 ligand inhibits T- samples examined, none contained CD137-positive lymphocyte proliferation and induces apoptosis.6,11 In mono- vessels. -

Oncoplastic Approach to Giant Benign Breast Tumors Presenting As Unilateral Macromastia
Published online: 2020-08-26 THIEME Case Report 439 Oncoplastic Approach to Giant Benign Breast Tumors Presenting as Unilateral Macromastia Lekshmi Malathi1, 1Department of Plastic Surgery, Government Medical College, Address for correspondence Lekshmi Malathi, MS, MCh, DNB, Kottayam, Kerala, India Department of Plastic Surgery, Government Medical College, Gandhinagar, Kottayam-686008, Kerala, India (e-mail: [email protected]). Indian J Plast Surg:2020;53:439–441 Abstract Benign breast tumors attaining large size constitute an important cause of unilateral macromastia. Their usual treatment involves enucleation or excision with a margin based on pathology and waiting for spontaneous retraction of skin envelope. In very Keywords large tumors, this will leave the residual breast deflated and unaesthetic, with spon- ► giant benign tumors taneous skin retraction giving unpredictable results. Application of the principles of ► oncoplasty oncoplastic surgery are helpful in this situation. Here, we present two cases of benign ► unilateral giant tumors—a giant fibroadenoma and a giant lipoma—managed by reduction mam- macromastia maplasty approach to restore the breast symmetry and aesthetics. Introduction Case Report and Technique Symmetry is of utmost importance in paired organs such as Case 1 breasts. The commonest cause of breast asymmetry or uni- A 34-year-old multiparous lady presented with right-sided lateral hypertrophy is an unequal physiological hypertrophy. macromastia for a period of 2 years. The enlargement was However, a neoplastic etiology should be thought of when gradual and asymptomatic, except for a heavy feeling on the there is marked asymmetry or architectural distortion.1 affected side. On examination, there was significant asym- The commonly encountered benign giant tumors are giant metry and a few dilated veins over the affected breast.