Palpable Breast Masses
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Common Breast Problems Guideline Team Team Leader Patient Population: Adults Age 18 and Older (Non-Pregnant)
Guidelines for Clinical Care Quality Department Ambulatory Breast Care Common Breast Problems Guideline Team Team leader Patient population: Adults age 18 and older (non-pregnant). Monica M Dimagno, MD Objectives: Identify appropriate evaluation and management strategies for common breast problems. General Medicine Identify appropriate indications for referral to a breast specialist. Team members Assumptions R Van Harrison, PhD Appropriate mammographic screening per NCCN, ACS, USPSTF and UMHS screening guidelines. Medical Education Generally mammogram is not indicated for women age <30 because of low sensitivity and specificity. Lisa A Newman, MD, MPH “Diagnostic breast imaging” refers to diagnostic mammogram and/or ultrasound. At most ages the Surgical Oncology combination of both imaging techniques yields the most accurate results and is recommended based on Ebony C Parker- patient age and the radiologist’s judgment. Featherstone, MD Key Aspects and Recommendations Family Medicine Palpable Mass or Asymmetric Thickening/Nodularity on Physical Exam (Figure 1) Mark D Pearlman, MD Obstetrics & Gynecology Discrete masses elevate the index of suspicion. Physical exam cannot reliably rule out malignancy. • Mark A Helvie, MD Breast imaging is the next diagnostic approach to aid in diagnosis [I C*]. Radiology/Breast Imaging • Initial imaging evaluation: if age ≥ 30 years then mammogram followed by breast ultrasound; if age < 30 years then breast ultrasound [I C*]. Follow-up depends on results (see Figure 1). Asymmetrical thickening / nodularity has a lower index of suspicion, but should be assessed with breast Initial Release imaging based on age as for patients with a discrete mass. If imaging is: November, 1996 • Suspicious or highly suggestive (BIRADS category 4 or 5) or if the area is assessed on clinical exam as Most Recent Major Update suspicious, then biopsy after imaging [I C*]. -

Approach to Breast Mass
APPROACH TO BREAST MASS Resident Author: Kathleen Doukas, MD, CCFP Faculty Advisor: Thea Weisdorf, MD, CCFP Creation Date: January 2010, Last updated: August 2013 Overview In primary care, breast lumps are a common complaint among women. In one study, 16% of women age 40-69y presented to their physician with a breast lesion over a 10-year period.1 Approximately 90% of these lesions will be benign, with fibroadenomas and cysts being the most common.2 Breast cancer must be ruled out, as one in ten woman who present with a new lump will have cancer.1 Diagnostic Considerations6 Benign: • Fibroadenoma: most common breast mass; a smooth, round, rubbery mobile mass, which is often found in young women; identifiable on US and mammogram • Breast cyst: mobile, often tender masses, which can fluctuate with the menstrual cycle; most common in premenopausal women; presence in a postmenopausal woman should raise suspicion for malignancy; ultrasound is the best method for differentiating between a cystic vs solid structure; a complex cyst is one with septations or solid components, and requires biopsy • Less common causes: Fat necrosis, intraductal papilloma, phyllodes tumor, breast abscess Premalignant: • Atypical Ductal Hyperplasia, Atypical Lobular Hyperplasia: Premalignant breast lesions with 4-6 times relative risk of developing subsequent breast cancer;8 often found incidentally on biopsy and require full excision • Carcinoma in Situ: o Ductal Carcinoma in Situ (DCIS): ~85% of in-situ breast cancers; defined as cancer confined to the duct that -
C O N F E R E N C E 22 27 April 2016
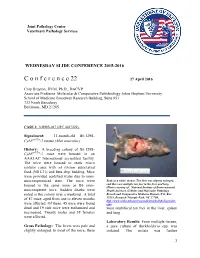
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2015-2016 C o n f e r e n c e 22 27 April 2016 Cory Brayton, DVM, Ph.D., DACVP Associate Professor, Molecular & Comparative Pathobiology Johns Hopkins University School of Medicine Broadway Research Building, Suite 851 733 North Broadway Baltimore, MD 21205 CASE I: NIEHS-087 (JPC 4017222). Signalment: 11-month-old B6.129S- Cybbtm1Din/J mouse (Mus musculus) History: A breeding colony of B6.129S- Cybbtm1Din/J mice were housed in an AAALAC International accredited facility. The mice were housed in static micro isolator cases with ad libitum autoclaved food (NIH-31) and beta chip bedding. Mice were provided acidified water due to imm- unocompromised state. The mice were Body as a while, mouse. The liver was slightly enlarged, housed in the same room as B6 imm- and there are multiple tan foci in the liver and lung. (Photo courtesy of: National Institute of Environmental unocompetent mice. Sudden deaths were Health Sciences, Cellular and Molecular Pathology noted in the colony over a weekend. A total Branch and Comparative Medicine Branch, P.O. Box of 87 mice, aged from one to eleven months 12233, Research Triangle Park, NC 27709, http://www.niehs.nih.gov/research/atniehs/labs/lep/index. were affected. Of these, 45 mice were found cfm) dead and 19 sick mice were euthanized and were multifocal tan foci in the liver, spleen necropsied. Twenty males and 38 females and lung. were affected. Laboratory Results: From multiple tissues, Gross Pathology: The livers were pale and a pure culture of Burkholderia spp. -

Diagnostic Approach to Soft Tissue Tumour of the Breast and Phyllodes Tumour in Ilorin, North Central with Review of Institutional Experience
World Journal of Medical Case Reports 2021; 2(3): 29-34 http://www.sciencepublishinggroup.com/j/wjmcr doi: 10.11648/j.wjmcr.20210203.11 Diagnostic Approach to Soft Tissue Tumour of the Breast and Phyllodes Tumour in Ilorin, North Central with Review of Institutional Experience Rasheed Mumini Wemimo 1, *, Afolayan Enoch Abiodun 1, Adegboye Adeyemi Taiwo 2 1Department of Pathology, University of Ilorin Teaching Hospital, Ilorin, Nigeria 2Mojitaiwo Data Services and Data Management Executives, Ilorin, Nigeria Email address: *Corresponding author To cite this article: Rasheed Mumini Wemimo, Afolayan Enoch Abiodun, Adegboye Adeyemi Taiwo. Diagnostic Approach to Soft Tissue Tumour of the Breast and Phyllodes Tumour in Ilorin, North Central with review of Institutional Experience. World Journal of Medical Case Reports. Vol. 2, No. 3, 2021, pp. 29-34. doi: 10.11648/j.wjmcr.20210203.11 Received : May 13, 2021; Accepted : June 7, 2021; Published : July 9, 2021 Abstract: Background: Primary soft tissue tumour (primary mesenchymal tumour) of the breast comprised of spectrum of neoplasm that arise from mammary stroma with comparable tumour biology of primary mesenchymal tumour at other sites. There are palpable diagnostic challenges which can be resolved by considering histomorphologic analysis that characterized each tumour entity regardless of the site and the use immunohistochemical markers. Methodology: This is an analytical hospital based retrospective study of patients with primary breast mesenchymal tumour and phyllodes diagnosed during 2014– 2019 at the Department of Pathology, University of Ilorin Teaching Hospital. The histopathological diagnosis of primary mesenchymal tumour of the breast and phyllodes tumours with documented age and other inclusion criteria were used for the study but excluded patients with incomplete information. -

Primary Breast Leiomyosarcoma and Synchronous Homolateral Lung Cancer: a Case Report
1059 Case Report Primary breast leiomyosarcoma and synchronous homolateral lung cancer: a case report Alberto Testori1, Stefano Meroni2, Emanuele Voulaz1, Marco Alloisio1, Rita De Sanctis3,4, Paola Bossi5, Umberto Cariboni1, Matilde De Simone6, Ugo Cioffi6 1General and Thoracic Surgery, Humanitas Research Hospital, Rozzano (Milan), Italy; 2Division of Breast Radiology, European Institute of Oncology, Milan, Italy; 3Department of Medical Oncology and Hematology, Humanitas Research Hospital, Rozzano (Milan), Italy; 4Molecular and Cellular Networks Lab, Department of Anatomy, Histology, Forensic Medicine and Orthopaedics, 'Sapienza' University, Rome, Italy; 5Department of Anatomo-Pathology, Humanitas Research Hospital, Rozzano (Milan), Italy; 6Department of Surgery, University of Milan, Milan, Italy Correspondence to: Alberto Testori, MD. General and Thoracic Surgery, Humanitas Research Hospital, Via Manzoni, 56, 20089 Rozzano (Milan), Italy. Email: [email protected]. Abstract: Radiological and histological features of breast leiomyosarcoma can mimic a wide variety of other breast lesions, such as mesenchymal tumors, breast lymphomas, poorly differentiated carcinomas and metaplastic breast carcinomas. The authors present the case of a 62-year-old woman with a primary breast leiomyosarcoma with synchronous ipsilateral lung adenocarcinoma. The latter was an incidental finding during pre-surgical staging examinations. Clinicopathological, immunophenotypic and imaging features cancer are described. A brief review of the literature on imaging findings and management of breast leiomyosarcoma is presented. The authors discuss the differential diagnoses in breast imaging and of the extra-mammary incidental findings. Surgical resection remains the cornerstone of treatment, while radiation therapy and chemotherapy remain to be defined on a single-patient basis. Keywords: Breast leiomyosarcoma; lung cancer; synchronous tumors Submitted May 14, 2017. -

Breast Concerns
Section 12.0: Preventive Health Services for Women Clinical Protocol Manual 12.2 BREAST CONCERNS TITLE DESCRIPTION DEFINITION: Breast concerns in women of all ages are often the source of significant fear and anxiety. These concerns can take the form of palpable masses or changes in breast contours, skin or nipple changes, congenital malformation, nipple discharge, or breast pain (cyclical and non-cyclical). 1. Palpable breast masses may represent cysts, fibroadenomas or cancer. a. Cysts are fluid-filled masses that can be found in women of all ages, and frequently develop due to hormonal fluctuation. They often change in relation to the menstrual cycle. b. Fibroadenomas are benign sold tumors that are caused by abnormal growth of the fibrous and ductal tissue of the breast. More common in adolescence or early twenties but can occur at any age. A fibroadenoma may grow progressively, remain the same, or regress. c. Masses that are due to cancer are generally distinct solid masses. They may also be merely thickened areas of the breast or exaggerated lumpiness or nodularity. It is impossible to diagnose the etiology of a breast mass based on physical exam alone. Failure to diagnose breast cancer in a timely manner is the most common reason for malpractice litigation in the U.S. Skin or nipple changes may be visible signs of an underlying breast cancer. These are danger signs and require MD referral. 2. Non-spontaneous or physiological discharge is fluid that may be expressed from the breast and is not unusual in healthy women. 3. Galactorrhea is a spontaneous, multiple duct, milky discharge most commonly found in non-lactating women during childbearing years. -

Giant Juvenile Fibroadenoma of Breast
Journal of Surgical Sciences (2013) Vol. 17 (2) : 99-102 © 2012 Society of Surgeons of Bangladesh JOURNAL OF SURGICAL SCIENCES Case Report GIANT JUVENILE FIBROADENOMA OF BREAST 2 2 3 5 KABM Taiful Alam1, Toufiqul Haque , Shamim Hossain , Kuntal Das , Tazul lslam4, Helena Ahmed Abstract: Giant juvenile fibroadenoma occurs in adolescent girls. These tumours become enormous in size and grow rapidly, though these tumours are mostly benign. These patients are almost always treated by breast conserving surgery. Here we present a case having unilateral giant juvenile fibroadenoma with bilateral multiple small fibroadenomas in an adolescent female aged 16years. The diagnosis of the patient was made on clinical examination, USG & FNAC. Confirmatory diagnosis was made by histopathology. We removed the giant one with "Swiss-Roll" procedure and others by simple enucleation. The aesthatic appearence of the breasts were preserved. Key words: Fibroadenoma, Giant fibroadenoma, Juvenile fibroadenoma, Swiss-roll operation. Introduction: can grow to immense proportions, compressing and Fibroadenoma is the most common benign tumour of displacing normal breast tissue and stretching the 4 female breast.It usually arises in the fully developed overlying skin and nipple areola complex . breast during the 15-25 years age period. They arise from hyperplasia of both fibrous & glandular tissue of Case report: a single lobule & usually grow upto 2-3 cm in size. A 16 year old girl presented with bilateral breast lumps Juvenile fibroadenoma is a benign tumour which occurs for 1 year. There were multiple lumps in the both during puberty1. It is a rare clinical condition and forms breasts among them one lump in the left breast was 4% of the total fibroadenomes--'. -

Investigations of Breast Tumors Withfluorine
10. Pacini F, Gasperi M, Fugazzola L, et al. Testicular thyroid cancer: potential risks and recommendations. dent: temporal correlation or casual relation? Br MedJ function in patients with differentiated thyroid carci Ear J Nuc! Med I993:20:192—194. 1994:309:158—162. noma treated with radioiodine. J Nucl Med 1994:35: 23. Dottorini ME, Lomuscio G, Mazzucchelli L, Vignati 34. Harjuletho T, Aro T, Rita H. Rytomaa T, SaxénL. The 1418 —1422. A, Colombo L. Assessment of female fertility and accident at Chernobyl and outcome of pregnancy in 11. Brincker H, Hansen HS, Andersen AP. Induction of carcinogenesis after iodine-I 3 1 therapy for differenti Finland. Br Med J I989:288:995—997. leukaemia by ‘@‘Itreatment ofthyroid carcinoma. BrJ ated thyroid carcinoma. J Nod Med 1995:36:21—27. 35. Bertollini R, Di Lallo D. Mastroiacovo P. Perucci CA. Cancer 1973:28:232—237. 24. Schlumberger M, Dc Vathaire F. Ceccarelli C, et al. Reduction of births in Italy after the Chemobyl acci 12. Hall P. HoIm LE, Lundell G. et al. Cancer risks in Exposure to radioactive iodine for scintigraphy or dent. Scandi Work Environ Health 1990:16:96—101. thyroid cancer patients. Br J Cancer 1991:64:159—163. therapy does not preclude pregnancy in thyroid cancer 36. Hawkins MM, Draper Gi, Winter DL. Cancer in the patients. J Nucl Med 1996:37:606—612. 13. Sobels FH. Estimation of the genetic risk resulting offspring of survivors of childhood leukemia and 25. Izembart M, Chavaudra J, Aubert B, ValléeG. Retro @ from the treatment of women with ‘I. -

Gynecomastia-Like Hyperplasia of Female Breast
Case Report Annals of Infertility & Reproductive Endocrinology Published: 25 May, 2018 Gynecomastia-Like Hyperplasia of Female Breast Haitham A Torky1*, Anwar A El-Shenawy2 and Ahmed N Eesa3 1Department of Obstetrics-Gynecology, As-Salam International Hospital, Egypt 2Department of Surgical Oncology, As-Salam International Hospital, Egypt 3Department of Pathology, As-Salam International Hospital, Egypt Abstract Introduction: Gynecomastia is defined as abnormal enlargement in the male breast; however, histo-pathologic abnormalities may theoretically occur in female breasts. Case: A 37 years old woman para 2 presented with a right painless breast lump. Bilateral mammographic study revealed right upper quadrant breast mass BIRADS 4b. Wide local excision of the mass pathology revealed fibrocystic disease with focal gynecomastoid hyperplasia. Conclusion: Gynecomastia-like hyperplasia of female breast is a rare entity that resembles malignant lesions clinically and radiological and is only distinguished by careful pathological examination. Keywords: Breast mass; Surgery; Female gynecomastia Introduction Gynecomastia is defined as abnormal enlargement in the male breast; however, the histo- pathologic abnormalities may theoretically occur in female breasts [1]. Rosen [2] was the first to describe the term “gynecomastia-like hyperplasia” as an extremely rare proliferative lesion of the female breast which cannot be distinguished from florid gynecomastia. The aim of the current case is to report one of the rare breast lesions, which is gynecomastia-like hyperplasia in female breast. Case Presentation A 37 years old woman para 2 presented with a right painless breast lump, which was accidentally OPEN ACCESS discovered 3 months ago and of stationary course. There was no history of trauma, constitutional symptoms or nipple discharge. -

Common Breast Problems BROOKE SALZMAN, MD; STEPHENIE FLEEGLE, MD; and AMBER S
Common Breast Problems BROOKE SALZMAN, MD; STEPHENIE FLEEGLE, MD; and AMBER S. TULLY, MD Thomas Jefferson University Hospital, Philadelphia, Pennsylvania A palpable mass, mastalgia, and nipple discharge are common breast symptoms for which patients seek medical atten- tion. Patients should be evaluated initially with a detailed clinical history and physical examination. Most women pre- senting with a breast mass will require imaging and further workup to exclude cancer. Diagnostic mammography is usually the imaging study of choice, but ultrasonography is more sensitive in women younger than 30 years. Any sus- picious mass that is detected on physical examination, mammography, or ultrasonography should be biopsied. Biopsy options include fine-needle aspiration, core needle biopsy, and excisional biopsy. Mastalgia is usually not an indica- tion of underlying malignancy. Oral contraceptives, hormone therapy, psychotropic drugs, and some cardiovascular agents have been associated with mastalgia. Focal breast pain should be evaluated with diagnostic imaging. Targeted ultrasonography can be used alone to evaluate focal breast pain in women younger than 30 years, and as an adjunct to mammography in women 30 years and older. Treatment options include acetaminophen and nonsteroidal anti- inflammatory drugs. The first step in the diagnostic workup for patients with nipple discharge is classification of the discharge as pathologic or physiologic. Nipple discharge is classified as pathologic if it is spontaneous, bloody, unilat- eral, or associated with a breast mass. Patients with pathologic discharge should be referred to a surgeon. Galactorrhea is the most common cause of physiologic discharge not associated with pregnancy or lactation. Prolactin and thyroid- stimulating hormone levels should be checked in patients with galactorrhea. -

Evaluation of Nipple Discharge
New 2016 American College of Radiology ACR Appropriateness Criteria® Evaluation of Nipple Discharge Variant 1: Physiologic nipple discharge. Female of any age. Initial imaging examination. Radiologic Procedure Rating Comments RRL* Mammography diagnostic 1 See references [2,4-7]. ☢☢ Digital breast tomosynthesis diagnostic 1 See references [2,4-7]. ☢☢ US breast 1 See references [2,4-7]. O MRI breast without and with IV contrast 1 See references [2,4-7]. O MRI breast without IV contrast 1 See references [2,4-7]. O FDG-PEM 1 See references [2,4-7]. ☢☢☢☢ Sestamibi MBI 1 See references [2,4-7]. ☢☢☢ Ductography 1 See references [2,4-7]. ☢☢ Image-guided core biopsy breast 1 See references [2,4-7]. Varies Image-guided fine needle aspiration breast 1 Varies *Relative Rating Scale: 1,2,3 Usually not appropriate; 4,5,6 May be appropriate; 7,8,9 Usually appropriate Radiation Level Variant 2: Pathologic nipple discharge. Male or female 40 years of age or older. Initial imaging examination. Radiologic Procedure Rating Comments RRL* See references [3,6,8,10,13,14,16,25- Mammography diagnostic 9 29,32,34,42-44,71-73]. ☢☢ See references [3,6,8,10,13,14,16,25- Digital breast tomosynthesis diagnostic 9 29,32,34,42-44,71-73]. ☢☢ US is usually complementary to mammography. It can be an alternative to mammography if the patient had a recent US breast 9 mammogram or is pregnant. See O references [3,5,10,12,13,16,25,30,31,45- 49]. MRI breast without and with IV contrast 1 See references [3,8,23,24,35,46,51-55]. -

Management of Fibroadenomas of the Breast
- Official Statement - Management of Fibroadenomas of the Breast Fibroadenoma of the breast is a common benign lesion affecting women during their reproductive years. Despite their benignity, fibroadenomas can cause physical deformity due to large size and may produce discomfort or emotional distress in affected individuals. The traditional management options available to women diagnosed with a fibroadenoma include observation or surgical excision. Two newer approaches, percutaneous excision and in situ cryoablation, have been developed and are less invasive than surgical excision. The purpose of this consensus statement is to put these four management options into perspective for our members and their patients. In most patients with fibroadenoma(s), the ideal approach is confirmation with percutaneous core biopsy and conservative follow-up. Because the malignant potential of fibroadenomas is extremely low, treatment is not required on an oncologic basis. This conservative approach is the least costly in terms of dollars and morbidity. A significant minority of fibroadenomas will disappear without treatment; with the remaining lesions either increasing in size or remaining unchanged. Because fibroadenomas can be bothersome to some patients, causing physical deformity, discomfort or emotional distress, most breast surgeons will respect an informed patient's preference for treatment. Traditional open excisional biopsy is effective treatment in such cases but it is the most costly option because of the operating room charges and time off from work. Open excision may still be the best option in some cases based on large size of the fibroadenoma or the judgment of the surgeon or patient preference. Studies have shown that ultrasound guided percutaneous excision of fibroadenomas is safe, effective and well tolerated by patients.