Amenorrhea: an Approach to Diagnosis and Management DAVID A
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Non Hormonal Management of Menstrual Cylce Irregularities
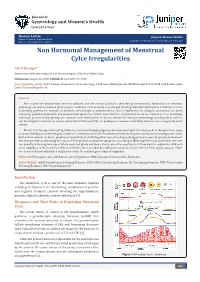
Journal of Gynecology and Women’s Health ISSN 2474-7602 Review Article J Gynecol Women’s Health Volume 11 Issue 4 - September 2018 Copyright © All rights are reserved by Arif A Faruqui DOI: 10.19080/JGWH.2018.11.555818 Non Hormonal Management of Menstrual Cylce Irregularities Arif A Faruqui* Department of Pharmacology, Clinical Pharmacologist, A 504, Rizvi Mahal, India Submission: August 16, 2018; Published: September 07, 2018 *Corresponding author: Email: Arif A Faruqui, Department of Pharmacology, A 504, Rizvi Mahal Opp. K.B. Bhabha Hospital, Waterfield road Bandra, India, Abstract of bleedingEach month patterns, the endometriumfor example, amenorrhea, becomes inflamed, menorrhagia and the or luminalpolymenorrhea; portion ovarianis shed dysfunctionduring menstruation. for example, Aberrations anovulation in menstrualand luteal physiology can lead to common gynecological conditions, such as heavy or prolonged bleeding. Menstrual dysfunction is defined in terms pathologic process or may predispose a woman to the development of chronic disease. For example, metrorrhagia predisposes to anemia, anddeficiency; the irregular painful menstrual menstruation cycles and associated premenstrual with PCOS syndrome. (see PCOS) Certain can characteristics predispose a woman of menstruation to infertility, can diabetes be a reflection and consequently, of an underlying heart disease. What is it, in this age of life-saving antibiotics, hormonal therapy, surgeries and other seemingly miraculous medical therapies that causes so many individuals to seek therapies outside of conventional medicine? Conventional medicine may be at its best when treating acute crises, but for the treatment of chronic problems it may fall short of offering either cure or healing, leading patients to seek out systems of treatment that they perceive as addressing the causes of their problem, not just the symptoms. -

The Prevalence of and Attitudes Toward Oligomenorrhea and Amenorrhea in Division I Female Athletes
POPULATION-SPECIFIC CONCERNS The Prevalence of and Attitudes Toward Oligomenorrhea and Amenorrhea in Division I Female Athletes Karen Myrick, DNP, APRN, FNP-BC, Richard Feinn, PhD, and Meaghan Harkins, MS, BSN, RN • Quinnipiac University Research has demonstrated that amenor- hormone and follicle-stimulating hormone rhea and oligomenorrhea may be common shut down stimulation to the ovary, ceasing occurrences among female athletes.1 Due production of estradiol.2 to normalization of menstrual dysfunction The effect of oral contraceptives on the within the sport environment, amenorrhea menstrual cycle include ovulation inhibi- and oligomenorrhea tion, changes in cervical mucus, thinning may be underreported. of the uterine endometrium, and motility Key PointsPoints There are many underly- and secretion in the fallopian tubes, which Lean sport athletes are more likely to per- ing causes of menstrual decrease the likelihood of conception and 3 ceive missed menstrual cycles as normal. dysfunction. However, implantation. Oral contraceptives contain a a similar hypothalamic combination of estrogen and progesterone, Menstrual dysfunction is one prong of the amenorrhea profile is or progesterone only; thus, oral contracep- female athlete triad. frequently seen in ath- tives do not stop the production of estrogen. letes, and hypothalamic Menstrual dysfunction is one prong of the Menstrual dysfunction is often associated dysfunction is com- female athlete triad (triad). The triad is a with musculoskeletal and endothelial monly the root of ath- syndrome of linking low energy availability compromise. lete’s menstrual abnor- (EA) with or without disordered eating, men- malities.2 The common strual disturbances, and low bone mineral Education and awareness of the accultur- hormone pattern for density, across a continuum. -

Current Evaluation of Amenorrhea
Current evaluation of amenorrhea The Practice Committee of the American Society for Reproductive Medicine Birmingham, Alabama Amenorrhea is the absence or abnormal cessation of the menses. Primary and secondary amenorrhea describe the occurrence of amenorrhea before and after menarche, respectively. (Fertil Steril 2006;86(Suppl 4):S148–55. © 2006 by American Society for Reproductive Medicine.) Amenorrhea is the absence or abnormal cessation of the menses complaint. The sexual ambiguity or virilization should be (1). Primary and secondary amenorrhea describe the occurrence evaluated as separate disorders, mindful that amenorrhea is of amenorrhea before and after menarche, respectively. The an important component of their presentation (9). majority of the causes of primary and secondary amenorrhea are similar. Timing of the evaluation of primary amenorrhea EVALUATION OF THE PATIENT recognizes the trend to earlier age at menarche and is therefore History, physical examination, and estimation of follicle indicated when there has been a failure to menstruate by age 15 stimulating hormone (FSH), thyroid stimulating hormone in the presence of normal secondary sexual development (two (TSH), and prolactin will identify the most common causes standard deviations above the mean of 13 years), or within five of amenorrhea (Fig. 1). The presence of breast development years after breast development if that occurs before age 10 (2). means there has been previous estrogen action. Excessive Failure to initiate breast development by age 13 (two standard testosterone secretion is suggested most often by hirsutism deviations above the mean of 10 years) also requires investiga- and rarely by increased muscle mass or other signs of viril- tion (2). -

Abnormal Uterine Bleeding: a Management Algorithm
J Am Board Fam Med: first published as 10.3122/jabfm.19.6.590 on 7 November 2006. Downloaded from EVIDENCED-BASED CLINICAL MEDICINE Abnormal Uterine Bleeding: A Management Algorithm John W. Ely, MD, MSPH, Colleen M. Kennedy, MD, MS, Elizabeth C. Clark, MD, MPH, and Noelle C. Bowdler, MD Abnormal uterine bleeding is a common problem, and its management can be complex. Because of this complexity, concise guidelines have been difficult to develop. We constructed a concise but comprehen- sive algorithm for the management of abnormal uterine bleeding between menarche and menopause that was based on a systematic review of the literature as well as the actual management of patients seen in a gynecology clinic. We started by drafting an algorithm that was based on a MEDLINE search for rel- evant reviews and original research. We compared this algorithm to the actual care provided to a ran- dom sample of 100 women with abnormal bleeding who were seen in a university gynecology clinic. Discrepancies between the algorithm and actual care were discussed during audiotaped meetings among the 4 investigators (2 family physicians and 2 gynecologists). The audiotapes were used to revise the algorithm. After 3 iterations of this process (total of 300 patients), we agreed on a final algorithm that generally followed the practices we observed, while maintaining consistency with the evidence. In clinic, the gynecologists categorized the patient’s bleeding pattern into 1 of 4 types: irregular bleeding, heavy but regular bleeding (menorrhagia), severe acute bleeding, and abnormal bleeding associated with a contraceptive method. Subsequent management involved both diagnostic and treatment interven- tions, which often occurred simultaneously. -

Too Much, Too Little, Too Late: Abnormal Uterine Bleeding
Too much, too little, too late: Abnormal uterine bleeding Jody Steinauer, MD, MAS July, 2015 The Questions • Too much (& too early or too late) – Differential and approach to work‐up – Does she need an endometrial biopsy (EMB)? – Does she need an ultrasound? – How do I stop peri‐menopausal bleeding? – Isn’t it due to the fibroids? • Too fast: She’s hemorrhaging—what do I do? • Too little: A quick review of amenorrhea Case 1 A 46 yo G3P2T1 reports her periods have become 1. What term describes increasingly irregular and heavy her symptoms? over the last 6‐8 months. 2. Physiologically, what Sometimes they come 2 times causes this type of per month and sometimes there bleeding pattern? are 2 months between. LMP 2 3. What is the months ago. She bleeds 10 days differential? with clots and frequently bleeds through pads to her clothes. She occasionally has hot flashes. She also has diabetes and is obese. Q1: In addition to a urine pregnancy test and TSH, which of the following is the most appropriate test to obtain at this time? 1. FSH 2. Testosterone & DHEAS 3. Serum beta‐HCG 4. Transvaginal Ultrasound (TVUS) 5. Endometrial Biopsy (EMB) Terminology: What is abnormal? • Normal: Cycle= 28 days +‐ 7 d (21‐35); Length=2‐7 days; Heaviness=self‐defined • Too little bleeding: amenorrhea or oligomenorrhea • Too much bleeding: Menorrhagia (regular timing but heavy (according to patient) OR long flow (>7 days) • Irregular bleeding: Metrorrhagia, intermenstrual or post‐ coital bleeding • Irregular and Excessive: Menometrorrhagia • Preferred term for non‐pregnant bleeding issues= Abnormal Uterine Bleeding (AUB) – Avoid “DUB” ‐ dysfunctional uterine bleeding. -

Age and Fertility: a Guide for Patients
Age and Fertility A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive Medicine under the direction of the Patient Education Committee and the Publications Committee. No portion herein may be reproduced in any form without written permission. This booklet is in no way intended to replace, dictate or fully define evaluation and treatment by a qualified physician. It is intended solely as an aid for patients seeking general information on issues in reproductive medicine. Copyright © 2012 by the American Society for Reproductive Medicine AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE Age and Fertility A Guide for Patients Revised 2012 A glossary of italicized words is located at the end of this booklet. INTRODUCTION Fertility changes with age. Both males and females become fertile in their teens following puberty. For girls, the beginning of their reproductive years is marked by the onset of ovulation and menstruation. It is commonly understood that after menopause women are no longer able to become pregnant. Generally, reproductive potential decreases as women get older, and fertility can be expected to end 5 to 10 years before menopause. In today’s society, age-related infertility is becoming more common because, for a variety of reasons, many women wait until their 30s to begin their families. Even though women today are healthier and taking better care of themselves than ever before, improved health in later life does not offset the natural age-related decline in fertility. It is important to understand that fertility declines as a woman ages due to the normal age- related decrease in the number of eggs that remain in her ovaries. -

Understanding Amenorrhea and PCOS
UCSF Essentials of Primary Care August 7, 2015 Squaw Creek, CA Understanding Amenorrhea and PCOS Michael Policar, MD, MPH Professor of Ob, Gyn, and Repro Sciences UCSF School of Medicine [email protected] Disclosure • I am a litigation consultant to a law firm contracted with Bayer Healthcare relating to the Mirena IUD 1 Amenorrhea: Definitions • Primary Amenorrhea – Absence of menarche by • 16 yo with sexual development – ASRM: 15 yo or >5 years after breasts develop • 14 yo without sexual development • Secondary Amenorrhea – No vaginal bleeding for at least • Three cycle lengths OR six months – ASRM: oligomenorrhea with < 9 menses/ year ASRM: American Society of Reproductive Medicine Presentation Approach to Amenorrhea • Most common diagnoses early in workup • Minimize potentially unnecessary tests and office visits • Separate evaluation schemes for – Spontaneous secondary amenorrhea – Post‐surgical amenorrhea – Primary amenorrhea – Progestin‐induced failure to withdraw 2 Reproductive Hormonal Axis HYPOTHALAMUS Hypothalamic GnRH Amenorrhea ANTERIOR PITUITARY Pituitary FSH Amenorrhea LH OVARY Ovarian Estradiol (E2 ) Failure Progesterone (P) ENDOMETRIUM Outflow Failure Amenorrhea: Causes • Hypothalamic amenorrhea • Pituitary amenorrhea • Ovarian failure • Outflow tract failure • Anovulatory amenorrhea • Pregnancy induced amenorrhea 3 2o Amenorrhea: Hypothalamic Amenorrhea • Athlete's amenorrhea – Critical ratio of muscle to body fat exceeded – Despite exercise, risk osteoporosis (and fracture) • Female athlete triad: disordered eating, -

Functional Hypothalamic Amenorrhea: a Stress-Based Disease
Review Functional Hypothalamic Amenorrhea: A Stress-Based Disease Agnieszka Podfigurna and Blazej Meczekalski * Department of Gynecological Endocrinology, Poznan University of Medical Sciences, 60-701 Poznan, Poland; agnieszkapodfi[email protected] * Correspondence: [email protected]; Tel.: +0048-6184-1933 Abstract: The aim of the study is to present the problem of functional hypothalamic amenorrhea, taking into account any disease and treatment, diagnosis, and consequences of this disease. We searched PubMed (MEDLINE) and included 38 original and review articles concerning functional hypothalamic amenorrhea. Functional hypothalamic amenorrhea is the most common cause of secondary amenorrhea in women of childbearing age. It is a reversible disorder caused by stress related to weight loss, excessive exercise and/or traumatic mental experiences. The basis of functional hypothalamic amenorrhea is hormonal, based on impaired pulsatile GnRH secretion in the hypotha- lamus, then decreased secretion of gonadotropins, and, consequently, impaired hormonal function of the ovaries. This disorder leads to hypoestrogenism, manifested by a disturbance of the menstrual cycle in the form of amenorrhea, leading to anovulation. Prolonged state of hypoestrogenism can be very detrimental to general health, leading to many harmful short- and long-term consequences. Treatment of functional hypothalamic amenorrhea should be started as soon as possible, and it should primarily involve lifestyle modification. Only then should pharmacological treatment be applied. Importantly, treatment is most often long-term, but it results in recovery for the majority of patients. Effective therapy, based on multidirectional action, can protect patients from numerous negative impacts on fertility, cardiovascular system and bone health, as well as reducing mental morbidity. Citation: Podfigurna, A.; Meczekalski, B. -

Abnormal Uterine Bleeding
Abnormal Uterine Bleeding in Premenopausal Women Noah Wouk, MD, Piedmont Health Services, Prospect Hill, North Carolina Margaret Helton, MD, University of North Carolina School of Medicine, Chapel Hill, North Carolina Abnormal uterine bleeding is a common symptom in women. The acronym PALM-COEIN facilitates classification, with PALM referring to structural etiologies (polyp, adenomyosis, leiomyoma, malignancy and hyperplasia), and COEIN referring to non- structural etiologies (coagulopathy, ovulatory dysfunction, endometrial, iatrogenic, not otherwise classified). Evaluation involves a detailed history and pelvic examination, as well as laboratory testing that includes a pregnancy test and complete blood count. Endometrial sampling should be performed in patients 45 years and older, and in younger patients with a sig- nificant history of unopposed estrogen exposure. Transvaginal ultrasonography is the preferred imaging modality and is indicated if a structural etiology is suspected or if symptoms persist despite appropriate initial treatment. Medical and surgical treatment options are available. Emergency interventions for severe bleeding that causes hemodynamic instability include uterine tamponade, intravenous estrogen, dilation and curettage, and uterine artery embolization. To avoid surgical risks and preserve fertility, medical management is the preferred initial approach for hemodynamically stable patients. Patients with severe bleeding can be treated initially with oral estrogen, high-dose estrogen-progestin oral contraceptives, -
Common Reproductive Issues
CHAPTER4 Izzy, a 27-year-old, presents to COMMON REPRODUCTIVE ISSUES her health care provider complain- ing of progressive severe pelvic KEY TERMS pain associated with her monthly abortion diaphragm menopause abstinence dysfunctional uterine oral contraceptives periods. She has to take off work amenorrhea bleeding (DUB) premenstrual syndrome basal body temperature dysmenorrhea (PMS) and “dope myself up” with pills to (BBT) emergency contraception Standard Days Method cervical cap (EC) (SDM) endure the pain. In addition, she cervical mucus ovulation endometriosis sterilization method fertility awareness symptothermal method has been trying to conceive for over coitus interruptus implant transdermal patch condoms infertility tubal ligation a year without any luck. contraception lactational amenorrhea vaginal ring contraceptive sponge method (LAM) vasectomy Depo-Provera Lunelle injection LEARNING OBJECTIVES Upon completion of the chapter the learner will be able to: 1. Define the key terms used in this chapter. 2. Examine common reproductive concerns in terms of symptoms, diag- nostic tests, and appropriate interventions. 3. Identify risk factors and outline appropriate client education needed in common reproductive disorders. 4. Compare and contrast the various contraceptive methods available and their overall effectiveness. 5. Explain the physiologic and psychological aspects of menopause. 6. Delineate the nursing management needed for women experiencing common reproductive disorders. When women bare their souls to us, we must respond without judgment. 2 CHAPTER 4 COMMON REPRODUCTIVE ISSUES 3 Good health throughout the life cycle begins with the BOX 4.1 Menstrual Disorder Vocabulary individual. Women today can expect to live well into their 80s and need to be proactive in maintaining their own • Meno = menstrual-related quality of life. -

A Quick Guide to Evaluation and Treatment
BY LINDA D. BRADLEY, MD Abnormal uterine bleeding A QUICK GUIDE TO EVALUATION AND TREATMENT After vaginitis, abnormal bleeding is the main reason women consult a gynecologist. Fortunately, the armamentarium is as broad as the range of etiologies. alf of all hysterectomies in the United systemic disease, or pregnancy. States are performed to treat abnor- Abnormal bleeding is associated with an Hmal uterine bleeding. Of these, array of symptoms. Frequent complaints approximately 20% are performed in women include heavy or prolonged menstrual flow, with a normal uterine size.1 However, when social embarrassment, diminished quality of the uterus appears nor- life, sexual compromise, and the need to Linda D. Bradley, MD mal, without adeno- alter lifestyle. Pain is not a common present- myosis or uterine pathol- ing symptom unless it is associated with the ogy, it is imperative that passage of large blood clots. the clinician perform a The following menstrual patterns are asso- thorough evaluation ciated with DUB: before resorting to hys- •Oligomenorrhea. A cycle length of more terectomy. than 35 days Abnormal uterine •Polymenorrhea. A cycle length of less than bleeding is defined as 21 days The physical must excessive, erratic, or •Amenorrhea. The absence of menses for 6 irregular bleeding in the months or 3 consecutive cycles be comprehensive, presence or absence of •Menorrhagia. Heavy or increased flow even in the intracavitary or uterine occurring at regular intervals, or a loss of pathology. It may be more than 80 mL of blood presence of heavy associated with structural •Metrorrhagia. Irregular episodes of bleeding bleeding. or systemic abnormali- •Menometrorrhagia. -

Menstrual Disorders in the Adolescent Female Donald E
University of Kentucky UKnowledge Pediatrics Faculty Publications Pediatrics 2012 Menstrual Disorders in the Adolescent Female Donald E. Greydanus Michigan State University Shawn Sorrel University of Kentucky Hatim A. Omar University of Kentucky, [email protected] Right click to open a feedback form in a new tab to let us know how this document benefits oy u. Follow this and additional works at: https://uknowledge.uky.edu/pediatrics_facpub Part of the Obstetrics and Gynecology Commons, and the Pediatrics Commons Repository Citation Greydanus, Donald E.; Sorrel, Shawn; and Omar, Hatim A., "Menstrual Disorders in the Adolescent Female" (2012). Pediatrics Faculty Publications. 101. https://uknowledge.uky.edu/pediatrics_facpub/101 This Book Chapter is brought to you for free and open access by the Pediatrics at UKnowledge. It has been accepted for inclusion in Pediatrics Faculty Publications by an authorized administrator of UKnowledge. For more information, please contact [email protected]. Menstrual Disorders in the Adolescent Female Notes/Citation Information Published in Adolescent Medicine: Pharmacotherapeutics in General, Mental and Sexual Health. Donald E. Greydanus, Dilip R. Patel, Hatim A. Omar, Cynthia Feucht, & Joav Merrick, (Eds.). p. 301-330. ©2012 Walter de Greyter GmbH & Co. KG, Berlin, Boston The opc yright holder has granted permission for posting the chapter here. Reprinted as an article in International Journal of Child and Adolescent Health, v. 5, no. 4, p. 357-378. Reprinted as a book chapter in Child and Adolescent Health Yearbook 2012. Joav Merrick, (Ed.). p. 415-442. This book chapter is available at UKnowledge: https://uknowledge.uky.edu/pediatrics_facpub/101 7 Menstrual disorders in the adolescent female Donald E.