AMENORRHEA I. INTRODUCTION A. Clinical Problems Arise in The
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Non Hormonal Management of Menstrual Cylce Irregularities
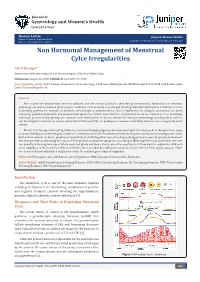
Journal of Gynecology and Women’s Health ISSN 2474-7602 Review Article J Gynecol Women’s Health Volume 11 Issue 4 - September 2018 Copyright © All rights are reserved by Arif A Faruqui DOI: 10.19080/JGWH.2018.11.555818 Non Hormonal Management of Menstrual Cylce Irregularities Arif A Faruqui* Department of Pharmacology, Clinical Pharmacologist, A 504, Rizvi Mahal, India Submission: August 16, 2018; Published: September 07, 2018 *Corresponding author: Email: Arif A Faruqui, Department of Pharmacology, A 504, Rizvi Mahal Opp. K.B. Bhabha Hospital, Waterfield road Bandra, India, Abstract of bleedingEach month patterns, the endometriumfor example, amenorrhea, becomes inflamed, menorrhagia and the or luminalpolymenorrhea; portion ovarianis shed dysfunctionduring menstruation. for example, Aberrations anovulation in menstrualand luteal physiology can lead to common gynecological conditions, such as heavy or prolonged bleeding. Menstrual dysfunction is defined in terms pathologic process or may predispose a woman to the development of chronic disease. For example, metrorrhagia predisposes to anemia, anddeficiency; the irregular painful menstrual menstruation cycles and associated premenstrual with PCOS syndrome. (see PCOS) Certain can characteristics predispose a woman of menstruation to infertility, can diabetes be a reflection and consequently, of an underlying heart disease. What is it, in this age of life-saving antibiotics, hormonal therapy, surgeries and other seemingly miraculous medical therapies that causes so many individuals to seek therapies outside of conventional medicine? Conventional medicine may be at its best when treating acute crises, but for the treatment of chronic problems it may fall short of offering either cure or healing, leading patients to seek out systems of treatment that they perceive as addressing the causes of their problem, not just the symptoms. -

Fungal Infections from Human and Animal Contact
Journal of Patient-Centered Research and Reviews Volume 4 Issue 2 Article 4 4-25-2017 Fungal Infections From Human and Animal Contact Dennis J. Baumgardner Follow this and additional works at: https://aurora.org/jpcrr Part of the Bacterial Infections and Mycoses Commons, Infectious Disease Commons, and the Skin and Connective Tissue Diseases Commons Recommended Citation Baumgardner DJ. Fungal infections from human and animal contact. J Patient Cent Res Rev. 2017;4:78-89. doi: 10.17294/2330-0698.1418 Published quarterly by Midwest-based health system Advocate Aurora Health and indexed in PubMed Central, the Journal of Patient-Centered Research and Reviews (JPCRR) is an open access, peer-reviewed medical journal focused on disseminating scholarly works devoted to improving patient-centered care practices, health outcomes, and the patient experience. REVIEW Fungal Infections From Human and Animal Contact Dennis J. Baumgardner, MD Aurora University of Wisconsin Medical Group, Aurora Health Care, Milwaukee, WI; Department of Family Medicine and Community Health, University of Wisconsin School of Medicine and Public Health, Madison, WI; Center for Urban Population Health, Milwaukee, WI Abstract Fungal infections in humans resulting from human or animal contact are relatively uncommon, but they include a significant proportion of dermatophyte infections. Some of the most commonly encountered diseases of the integument are dermatomycoses. Human or animal contact may be the source of all types of tinea infections, occasional candidal infections, and some other types of superficial or deep fungal infections. This narrative review focuses on the epidemiology, clinical features, diagnosis and treatment of anthropophilic dermatophyte infections primarily found in North America. -

The Prevalence of and Attitudes Toward Oligomenorrhea and Amenorrhea in Division I Female Athletes
POPULATION-SPECIFIC CONCERNS The Prevalence of and Attitudes Toward Oligomenorrhea and Amenorrhea in Division I Female Athletes Karen Myrick, DNP, APRN, FNP-BC, Richard Feinn, PhD, and Meaghan Harkins, MS, BSN, RN • Quinnipiac University Research has demonstrated that amenor- hormone and follicle-stimulating hormone rhea and oligomenorrhea may be common shut down stimulation to the ovary, ceasing occurrences among female athletes.1 Due production of estradiol.2 to normalization of menstrual dysfunction The effect of oral contraceptives on the within the sport environment, amenorrhea menstrual cycle include ovulation inhibi- and oligomenorrhea tion, changes in cervical mucus, thinning may be underreported. of the uterine endometrium, and motility Key PointsPoints There are many underly- and secretion in the fallopian tubes, which Lean sport athletes are more likely to per- ing causes of menstrual decrease the likelihood of conception and 3 ceive missed menstrual cycles as normal. dysfunction. However, implantation. Oral contraceptives contain a a similar hypothalamic combination of estrogen and progesterone, Menstrual dysfunction is one prong of the amenorrhea profile is or progesterone only; thus, oral contracep- female athlete triad. frequently seen in ath- tives do not stop the production of estrogen. letes, and hypothalamic Menstrual dysfunction is one prong of the Menstrual dysfunction is often associated dysfunction is com- female athlete triad (triad). The triad is a with musculoskeletal and endothelial monly the root of ath- syndrome of linking low energy availability compromise. lete’s menstrual abnor- (EA) with or without disordered eating, men- malities.2 The common strual disturbances, and low bone mineral Education and awareness of the accultur- hormone pattern for density, across a continuum. -

Dermatology DDX Deck, 2Nd Edition 65
63. Herpes simplex (cold sores, fever blisters) PREMALIGNANT AND MALIGNANT NON- 64. Varicella (chicken pox) MELANOMA SKIN TUMORS Dermatology DDX Deck, 2nd Edition 65. Herpes zoster (shingles) 126. Basal cell carcinoma 66. Hand, foot, and mouth disease 127. Actinic keratosis TOPICAL THERAPY 128. Squamous cell carcinoma 1. Basic principles of treatment FUNGAL INFECTIONS 129. Bowen disease 2. Topical corticosteroids 67. Candidiasis (moniliasis) 130. Leukoplakia 68. Candidal balanitis 131. Cutaneous T-cell lymphoma ECZEMA 69. Candidiasis (diaper dermatitis) 132. Paget disease of the breast 3. Acute eczematous inflammation 70. Candidiasis of large skin folds (candidal 133. Extramammary Paget disease 4. Rhus dermatitis (poison ivy, poison oak, intertrigo) 134. Cutaneous metastasis poison sumac) 71. Tinea versicolor 5. Subacute eczematous inflammation 72. Tinea of the nails NEVI AND MALIGNANT MELANOMA 6. Chronic eczematous inflammation 73. Angular cheilitis 135. Nevi, melanocytic nevi, moles 7. Lichen simplex chronicus 74. Cutaneous fungal infections (tinea) 136. Atypical mole syndrome (dysplastic nevus 8. Hand eczema 75. Tinea of the foot syndrome) 9. Asteatotic eczema 76. Tinea of the groin 137. Malignant melanoma, lentigo maligna 10. Chapped, fissured feet 77. Tinea of the body 138. Melanoma mimics 11. Allergic contact dermatitis 78. Tinea of the hand 139. Congenital melanocytic nevi 12. Irritant contact dermatitis 79. Tinea incognito 13. Fingertip eczema 80. Tinea of the scalp VASCULAR TUMORS AND MALFORMATIONS 14. Keratolysis exfoliativa 81. Tinea of the beard 140. Hemangiomas of infancy 15. Nummular eczema 141. Vascular malformations 16. Pompholyx EXANTHEMS AND DRUG REACTIONS 142. Cherry angioma 17. Prurigo nodularis 82. Non-specific viral rash 143. Angiokeratoma 18. Stasis dermatitis 83. -

Current Evaluation of Amenorrhea
Current evaluation of amenorrhea The Practice Committee of the American Society for Reproductive Medicine Birmingham, Alabama Amenorrhea is the absence or abnormal cessation of the menses. Primary and secondary amenorrhea describe the occurrence of amenorrhea before and after menarche, respectively. (Fertil Steril 2006;86(Suppl 4):S148–55. © 2006 by American Society for Reproductive Medicine.) Amenorrhea is the absence or abnormal cessation of the menses complaint. The sexual ambiguity or virilization should be (1). Primary and secondary amenorrhea describe the occurrence evaluated as separate disorders, mindful that amenorrhea is of amenorrhea before and after menarche, respectively. The an important component of their presentation (9). majority of the causes of primary and secondary amenorrhea are similar. Timing of the evaluation of primary amenorrhea EVALUATION OF THE PATIENT recognizes the trend to earlier age at menarche and is therefore History, physical examination, and estimation of follicle indicated when there has been a failure to menstruate by age 15 stimulating hormone (FSH), thyroid stimulating hormone in the presence of normal secondary sexual development (two (TSH), and prolactin will identify the most common causes standard deviations above the mean of 13 years), or within five of amenorrhea (Fig. 1). The presence of breast development years after breast development if that occurs before age 10 (2). means there has been previous estrogen action. Excessive Failure to initiate breast development by age 13 (two standard testosterone secretion is suggested most often by hirsutism deviations above the mean of 10 years) also requires investiga- and rarely by increased muscle mass or other signs of viril- tion (2). -

Abnormal Uterine Bleeding: a Management Algorithm
J Am Board Fam Med: first published as 10.3122/jabfm.19.6.590 on 7 November 2006. Downloaded from EVIDENCED-BASED CLINICAL MEDICINE Abnormal Uterine Bleeding: A Management Algorithm John W. Ely, MD, MSPH, Colleen M. Kennedy, MD, MS, Elizabeth C. Clark, MD, MPH, and Noelle C. Bowdler, MD Abnormal uterine bleeding is a common problem, and its management can be complex. Because of this complexity, concise guidelines have been difficult to develop. We constructed a concise but comprehen- sive algorithm for the management of abnormal uterine bleeding between menarche and menopause that was based on a systematic review of the literature as well as the actual management of patients seen in a gynecology clinic. We started by drafting an algorithm that was based on a MEDLINE search for rel- evant reviews and original research. We compared this algorithm to the actual care provided to a ran- dom sample of 100 women with abnormal bleeding who were seen in a university gynecology clinic. Discrepancies between the algorithm and actual care were discussed during audiotaped meetings among the 4 investigators (2 family physicians and 2 gynecologists). The audiotapes were used to revise the algorithm. After 3 iterations of this process (total of 300 patients), we agreed on a final algorithm that generally followed the practices we observed, while maintaining consistency with the evidence. In clinic, the gynecologists categorized the patient’s bleeding pattern into 1 of 4 types: irregular bleeding, heavy but regular bleeding (menorrhagia), severe acute bleeding, and abnormal bleeding associated with a contraceptive method. Subsequent management involved both diagnostic and treatment interven- tions, which often occurred simultaneously. -

Too Much, Too Little, Too Late: Abnormal Uterine Bleeding
Too much, too little, too late: Abnormal uterine bleeding Jody Steinauer, MD, MAS July, 2015 The Questions • Too much (& too early or too late) – Differential and approach to work‐up – Does she need an endometrial biopsy (EMB)? – Does she need an ultrasound? – How do I stop peri‐menopausal bleeding? – Isn’t it due to the fibroids? • Too fast: She’s hemorrhaging—what do I do? • Too little: A quick review of amenorrhea Case 1 A 46 yo G3P2T1 reports her periods have become 1. What term describes increasingly irregular and heavy her symptoms? over the last 6‐8 months. 2. Physiologically, what Sometimes they come 2 times causes this type of per month and sometimes there bleeding pattern? are 2 months between. LMP 2 3. What is the months ago. She bleeds 10 days differential? with clots and frequently bleeds through pads to her clothes. She occasionally has hot flashes. She also has diabetes and is obese. Q1: In addition to a urine pregnancy test and TSH, which of the following is the most appropriate test to obtain at this time? 1. FSH 2. Testosterone & DHEAS 3. Serum beta‐HCG 4. Transvaginal Ultrasound (TVUS) 5. Endometrial Biopsy (EMB) Terminology: What is abnormal? • Normal: Cycle= 28 days +‐ 7 d (21‐35); Length=2‐7 days; Heaviness=self‐defined • Too little bleeding: amenorrhea or oligomenorrhea • Too much bleeding: Menorrhagia (regular timing but heavy (according to patient) OR long flow (>7 days) • Irregular bleeding: Metrorrhagia, intermenstrual or post‐ coital bleeding • Irregular and Excessive: Menometrorrhagia • Preferred term for non‐pregnant bleeding issues= Abnormal Uterine Bleeding (AUB) – Avoid “DUB” ‐ dysfunctional uterine bleeding. -

Hair and Nail Disorders
Hair and Nail Disorders E.J. Mayeaux, Jr., M.D., FAAFP Professor of Family Medicine Professor of Obstetrics/Gynecology Louisiana State University Health Sciences Center Shreveport, LA Hair Classification • Terminal (large) hairs – Found on the head and beard – Larger diameters and roots that extend into sub q fat LSUCourtesy Health of SciencesDr. E.J. Mayeaux, Center Jr., – M.D.USA Hair Classification • Vellus hairs are smaller in length and diameter and have less pigment • Intermediate hairs have mixed characteristics CourtesyLSU Health of E.J. Sciences Mayeaux, Jr.,Center M.D. – USA Life cycle of a hair • Hair grows at 0.35 mm/day • Cycle is typically as follows: – Anagen phase (active growth) - 3 years – Catagen (transitional) - 2-3 weeks – Telogen (preshedding or rest) about 3 Mon. • > 85% of hairs of the scalp are in Anagen – Lose 75 – 100 hairs a day • Each hair follicle’s cycle is usually asynchronous with others around it LSU Health Sciences Center – USA Alopecia Definition • Defined as partial or complete loss of hair from where it would normally grow • Can be total, diffuse, patchy, or localized Courtesy of E.J. Mayeaux, Jr., M.D. CourtesyLSU of Healththe Color Sciences Atlas of Family Center Medicine – USA Classification of Alopecia Scarring Nonscarring Neoplastic Medications Nevoid Congenital Injury such as burns Infectious Systemic illnesses Genetic (male pattern) (LE) Toxic (arsenic) Congenital Nutritional Traumatic Endocrine Immunologic PhysiologicLSU Health Sciences Center – USA General Evaluation of Hair Loss • Hx is -

Age and Fertility: a Guide for Patients
Age and Fertility A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive Medicine under the direction of the Patient Education Committee and the Publications Committee. No portion herein may be reproduced in any form without written permission. This booklet is in no way intended to replace, dictate or fully define evaluation and treatment by a qualified physician. It is intended solely as an aid for patients seeking general information on issues in reproductive medicine. Copyright © 2012 by the American Society for Reproductive Medicine AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE Age and Fertility A Guide for Patients Revised 2012 A glossary of italicized words is located at the end of this booklet. INTRODUCTION Fertility changes with age. Both males and females become fertile in their teens following puberty. For girls, the beginning of their reproductive years is marked by the onset of ovulation and menstruation. It is commonly understood that after menopause women are no longer able to become pregnant. Generally, reproductive potential decreases as women get older, and fertility can be expected to end 5 to 10 years before menopause. In today’s society, age-related infertility is becoming more common because, for a variety of reasons, many women wait until their 30s to begin their families. Even though women today are healthier and taking better care of themselves than ever before, improved health in later life does not offset the natural age-related decline in fertility. It is important to understand that fertility declines as a woman ages due to the normal age- related decrease in the number of eggs that remain in her ovaries. -

Trachyonychia Associated with Alopecia Areata and Secondary Onychomycosis
TRACHYONYCHIA ASSOCIATED WITH ALOPECIA AREATA AND SECONDARY ONYCHOMYCOSIS Jose L. Anggowarsito Renate T. Kandou Department of Dermatovenereology Medical Faculty of Sam Ratulangi University Prof. Dr. R. D. Kandou Hospital Manado Email: [email protected] Abstract: Trachyonychia is an idiopathic nail inflammatory disorder that causes nail matrix keratinization abnormality, often found in children, and associated with alopecia areata, psoriasis, atopic dermatitis, or nail lichen planus. Trachyonychia could be a manifestation of associated pleomorphic or idiopathic disorders; therefore, it may occur without skin or other systemic disorders. There is no specific diagnostic criteria for tracyonychia. A biopsy is needed to determine the definite pathologic diagnosis for nail matrix disorder; albeit, in a trachyonychia case it is not entirely necessary. Trachyonychia assessment is often unsatisfactory and its management is focused primarily on the underlying disease. We reported an 8-year-old girl with twenty dystrophic nails associated with alopecia areata. Cultures of nail base scrapings were performed two times and the final impression was trichophyton rubrum. Conclusion: Based on the clinical examination and all the tests performed the diagnosis of this case was trachyonychia with twenty dystrophic nails associated with alopecia areata and secondary onychomycosis.The majority of trachyonychia cases undergo spontaneous improvement; therefore, a specific therapy seems unnecessary. Onychomycosis is often difficult to be treated. Eradication of the fungi is not always followed by nail restructure, especially if there has been dystrophy before the infection. Keywords: trachyonychia, alopecia areata, onychomycosis. Abstrak: Trakionikia adalah inflamasi kuku idiopatik yang menyebabkan gangguan keratinisasi matriks kuku, sering terjadi pada anak, dan terkait dengan alopesia areata, psoriasis, dermatitis atopik atau lichen planus kuku. -

Understanding Amenorrhea and PCOS
UCSF Essentials of Primary Care August 7, 2015 Squaw Creek, CA Understanding Amenorrhea and PCOS Michael Policar, MD, MPH Professor of Ob, Gyn, and Repro Sciences UCSF School of Medicine [email protected] Disclosure • I am a litigation consultant to a law firm contracted with Bayer Healthcare relating to the Mirena IUD 1 Amenorrhea: Definitions • Primary Amenorrhea – Absence of menarche by • 16 yo with sexual development – ASRM: 15 yo or >5 years after breasts develop • 14 yo without sexual development • Secondary Amenorrhea – No vaginal bleeding for at least • Three cycle lengths OR six months – ASRM: oligomenorrhea with < 9 menses/ year ASRM: American Society of Reproductive Medicine Presentation Approach to Amenorrhea • Most common diagnoses early in workup • Minimize potentially unnecessary tests and office visits • Separate evaluation schemes for – Spontaneous secondary amenorrhea – Post‐surgical amenorrhea – Primary amenorrhea – Progestin‐induced failure to withdraw 2 Reproductive Hormonal Axis HYPOTHALAMUS Hypothalamic GnRH Amenorrhea ANTERIOR PITUITARY Pituitary FSH Amenorrhea LH OVARY Ovarian Estradiol (E2 ) Failure Progesterone (P) ENDOMETRIUM Outflow Failure Amenorrhea: Causes • Hypothalamic amenorrhea • Pituitary amenorrhea • Ovarian failure • Outflow tract failure • Anovulatory amenorrhea • Pregnancy induced amenorrhea 3 2o Amenorrhea: Hypothalamic Amenorrhea • Athlete's amenorrhea – Critical ratio of muscle to body fat exceeded – Despite exercise, risk osteoporosis (and fracture) • Female athlete triad: disordered eating, -

Functional Hypothalamic Amenorrhea: a Stress-Based Disease
Review Functional Hypothalamic Amenorrhea: A Stress-Based Disease Agnieszka Podfigurna and Blazej Meczekalski * Department of Gynecological Endocrinology, Poznan University of Medical Sciences, 60-701 Poznan, Poland; agnieszkapodfi[email protected] * Correspondence: [email protected]; Tel.: +0048-6184-1933 Abstract: The aim of the study is to present the problem of functional hypothalamic amenorrhea, taking into account any disease and treatment, diagnosis, and consequences of this disease. We searched PubMed (MEDLINE) and included 38 original and review articles concerning functional hypothalamic amenorrhea. Functional hypothalamic amenorrhea is the most common cause of secondary amenorrhea in women of childbearing age. It is a reversible disorder caused by stress related to weight loss, excessive exercise and/or traumatic mental experiences. The basis of functional hypothalamic amenorrhea is hormonal, based on impaired pulsatile GnRH secretion in the hypotha- lamus, then decreased secretion of gonadotropins, and, consequently, impaired hormonal function of the ovaries. This disorder leads to hypoestrogenism, manifested by a disturbance of the menstrual cycle in the form of amenorrhea, leading to anovulation. Prolonged state of hypoestrogenism can be very detrimental to general health, leading to many harmful short- and long-term consequences. Treatment of functional hypothalamic amenorrhea should be started as soon as possible, and it should primarily involve lifestyle modification. Only then should pharmacological treatment be applied. Importantly, treatment is most often long-term, but it results in recovery for the majority of patients. Effective therapy, based on multidirectional action, can protect patients from numerous negative impacts on fertility, cardiovascular system and bone health, as well as reducing mental morbidity. Citation: Podfigurna, A.; Meczekalski, B.