Role of Mastoid Pneumatization in Temporal Bone Fractures
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Morphometric Study of Occurrence and Variations of Foramen Ovale S
Research Article The morphometric study of occurrence and variations of foramen ovale S. Ajrish George*, M. S. Thenmozhi ABSTRACT Background: Foramen vale is one of the important foramina present in the sphenoid bone. Anatomically it is located in the greater wing of the sphenoid bone. The foramen ovale is situated posterolateral to the foramen rotundum and anteromedial to the foramen spinosum. The foramen spinosum is present posterior to the foramen ovale. The carotid canal is present posterior and medial to the foramen spinosum and the foramen rotundum is present anterior to the foramen ovale. The structures which pass through the foramen ovale are the mandibular nerve, emissary vein, accessory middle meningeal artery, and lesser petrosal nerve. The sphenoid bone has a body, a pair of greater wing, pair of lesser wing, pair of lateral pterygoid plate, and a pair of medial pterygoid plate. Aim: The study involves the assessment of any additional features in foramen ovale in dry South Indian skulls. Materials and Methods: This study involves examination of dry adult skulls. First, the foramen ovale is located, and then it is carefully examined for presence of alterations and additional features, and is recorded following computing the data and analyzing it. Results: The maximum length of foramen ovale on the right and left was 10.1 mm, 4.3 mm, respectively. The minimum length of the foramen in right and left was 9.1 mm, 3.2 mm, respectively. The maximum width of foramen ovale on the right and left was 4.8 mm and 2.3 mm, respectively. The minimum width of the foramen in the right and the left side was 5.7 mm and 2.9 mm, respectively. -

Gross Anatomy Assignment Name: Olorunfemi Peace Toluwalase Matric No: 17/Mhs01/257 Dept: Mbbs Course: Gross Anatomy of Head and Neck
GROSS ANATOMY ASSIGNMENT NAME: OLORUNFEMI PEACE TOLUWALASE MATRIC NO: 17/MHS01/257 DEPT: MBBS COURSE: GROSS ANATOMY OF HEAD AND NECK QUESTION 1 Write an essay on the carvernous sinus. The cavernous sinuses are one of several drainage pathways for the brain that sits in the middle. In addition to receiving venous drainage from the brain, it also receives tributaries from parts of the face. STRUCTURE ➢ The cavernous sinuses are 1 cm wide cavities that extend a distance of 2 cm from the most posterior aspect of the orbit to the petrous part of the temporal bone. ➢ They are bilaterally paired collections of venous plexuses that sit on either side of the sphenoid bone. ➢ Although they are not truly trabeculated cavities like the corpora cavernosa of the penis, the numerous plexuses, however, give the cavities their characteristic sponge-like appearance. ➢ The cavernous sinus is roofed by an inner layer of dura matter that continues with the diaphragma sellae that covers the superior part of the pituitary gland. The roof of the sinus also has several other attachments. ➢ Anteriorly, it attaches to the anterior and middle clinoid processes, posteriorly it attaches to the tentorium (at its attachment to the posterior clinoid process). Part of the periosteum of the greater wing of the sphenoid bone forms the floor of the sinus. ➢ The body of the sphenoid acts as the medial wall of the sinus while the lateral wall is formed from the visceral part of the dura mater. CONTENTS The cavernous sinus contains the internal carotid artery and several cranial nerves. Abducens nerve (CN VI) traverses the sinus lateral to the internal carotid artery. -

Septation of the Sphenoid Sinus and Its Clinical Significance
1793 International Journal of Collaborative Research on Internal Medicine & Public Health Septation of the Sphenoid Sinus and its Clinical Significance Eldan Kapur 1* , Adnan Kapidžić 2, Amela Kulenović 1, Lana Sarajlić 2, Adis Šahinović 2, Maida Šahinović 3 1 Department of anatomy, Medical faculty, University of Sarajevo, Čekaluša 90, 71000 Sarajevo, Bosnia and Herzegovina 2 Clinic for otorhinolaryngology, Clinical centre University of Sarajevo, Bolnička 25, 71000 Sarajevo, Bosnia and Herzegovina 3 Department of histology and embriology, Medical faculty, University of Sarajevo, Čekaluša 90, 71000 Sarajevo, Bosnia and Herzegovina * Corresponding Author: Eldan Kapur, MD, PhD Department of anatomy, Medical faculty, University of Sarajevo, Bosnia and Herzegovina Email: [email protected] Phone: 033 66 55 49; 033 22 64 78 (ext. 136) Abstract Introduction: Sphenoid sinus is located in the body of sphenoid, closed with a thin plate of bone tissue that separates it from the important structures such as the optic nerve, optic chiasm, cavernous sinus, pituitary gland, and internal carotid artery. It is divided by one or more vertical septa that are often asymmetric. Because of its location and the relationships with important neurovascular and glandular structures, sphenoid sinus represents a great diagnostic and therapeutic challenge. Aim: The aim of this study was to assess the septation of the sphenoid sinus and relationship between the number and position of septa and internal carotid artery in the adult BH population. Participants and Methods: A retrospective study of the CT analysis of the paranasal sinuses in 200 patients (104 male, 96 female) were performed using Siemens Somatom Art with the following parameters: 130 mAs: 120 kV, Slice: 3 mm. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -

Microscopic Anatomy of the Carotid Canal and Its Relations with Cochlea
Rev Bras Otorrinolaringol. V.71, n.4, 410-4, jul./ago. 2005 ARTIGO ORIGINAL ORIGINAL ARTICLE Anatomia microscópica do canal Microscopic anatomy of the carótico e suas relações com a carotid canal and its relations cóclea e a cavidade timpânica with cochlea and middle ear Norma de Oliveira Penido1, Andrei Borin2, 3 4 Palavras-chave: anatomia, osso temporal, Yotaka Fukuda , Cristina Navarro Santos Lion artéria carótida interna, cóclea, orelha. Key words: anatomy, temporal bone, internal carotid artery, cochlea, ear. Resumo / Summary s relações entre as diversas estruturas nobres e vitais he knowledge of the relations between the noble and queA se apresentam na intimidade do osso temporal consti- vitalT structures of temporal bone is still a great challenge for tuem ainda hoje um grande desafio para o cirurgião otológico. the otologic surgeon. The microscopic anatomic studies of Os estudos micro-anatômicos do mesmo se encontram en- the temporal bone are one of the greatest help to prevent tre as grandes armas na busca deste entendimento. Objeti- lesions during surgical intervention. Aim: To study the vo: Estudar as correlações anatômicas entre o canal carótico anatomic correlations between the carotid canal and the e a cóclea, e a ocorrência de deiscências do mesmo junto à cochlea, and the occurrence of dehiscence of the carotid cavidade timpânica. Material e Método: Estudo microscó- canal in the middle ear tympanic cavity. Material and pico de 122 ossos temporais humanos. Resultados: As dis- Methods: Microscopic study of 122 human temporal bones. tâncias médias entre o canal carótico e os giros cocleares RESULTS: The average distance between the carotid canal foram: no local de menor distância 1,05mm; no giro basal, and the cochlea were: the shortest distance, 1.05mm; basal 2,04mm; no giro médio, 2,32mm; e no giro apical, 5,7mm. -

Lab Manual Axial Skeleton Atla
1 PRE-LAB EXERCISES When studying the skeletal system, the bones are often sorted into two broad categories: the axial skeleton and the appendicular skeleton. This lab focuses on the axial skeleton, which consists of the bones that form the axis of the body. The axial skeleton includes bones in the skull, vertebrae, and thoracic cage, as well as the auditory ossicles and hyoid bone. In addition to learning about all the bones of the axial skeleton, it is also important to identify some significant bone markings. Bone markings can have many shapes, including holes, round or sharp projections, and shallow or deep valleys, among others. These markings on the bones serve many purposes, including forming attachments to other bones or muscles and allowing passage of a blood vessel or nerve. It is helpful to understand the meanings of some of the more common bone marking terms. Before we get started, look up the definitions of these common bone marking terms: Canal: Condyle: Facet: Fissure: Foramen: (see Module 10.18 Foramina of Skull) Fossa: Margin: Process: Throughout this exercise, you will notice bold terms. This is meant to focus your attention on these important words. Make sure you pay attention to any bold words and know how to explain their definitions and/or where they are located. Use the following modules to guide your exploration of the axial skeleton. As you explore these bones in Visible Body’s app, also locate the bones and bone markings on any available charts, models, or specimens. You may also find it helpful to palpate bones on yourself or make drawings of the bones with the bone markings labeled. -

MBB: Head & Neck Anatomy
MBB: Head & Neck Anatomy Skull Osteology • This is a comprehensive guide of all the skull features you must know by the practical exam. • Many of these structures will be presented multiple times during upcoming labs. • This PowerPoint Handout is the resource you will use during lab when you have access to skulls. Mind, Brain & Behavior 2021 Osteology of the Skull Slide Title Slide Number Slide Title Slide Number Ethmoid Slide 3 Paranasal Sinuses Slide 19 Vomer, Nasal Bone, and Inferior Turbinate (Concha) Slide4 Paranasal Sinus Imaging Slide 20 Lacrimal and Palatine Bones Slide 5 Paranasal Sinus Imaging (Sagittal Section) Slide 21 Zygomatic Bone Slide 6 Skull Sutures Slide 22 Frontal Bone Slide 7 Foramen RevieW Slide 23 Mandible Slide 8 Skull Subdivisions Slide 24 Maxilla Slide 9 Sphenoid Bone Slide 10 Skull Subdivisions: Viscerocranium Slide 25 Temporal Bone Slide 11 Skull Subdivisions: Neurocranium Slide 26 Temporal Bone (Continued) Slide 12 Cranial Base: Cranial Fossae Slide 27 Temporal Bone (Middle Ear Cavity and Facial Canal) Slide 13 Skull Development: Intramembranous vs Endochondral Slide 28 Occipital Bone Slide 14 Ossification Structures/Spaces Formed by More Than One Bone Slide 15 Intramembranous Ossification: Fontanelles Slide 29 Structures/Apertures Formed by More Than One Bone Slide 16 Intramembranous Ossification: Craniosynostosis Slide 30 Nasal Septum Slide 17 Endochondral Ossification Slide 31 Infratemporal Fossa & Pterygopalatine Fossa Slide 18 Achondroplasia and Skull Growth Slide 32 Ethmoid • Cribriform plate/foramina -

Surgical Management of Posterior Petrous Meningiomas
Neurosurg Focus 14 (6):Article 7, 2003, Click here to return to Table of Contents Surgical management of posterior petrous meningiomas JAMES K. LIU, M.D., OREN N. GOTTFRIED, M.D., AND WILLIAM T. COULDWELL, M.D., PH.D. Department of Neurosurgery, University of Utah School of Medicine, Salt Lake City, Utah Posterior petrous meningiomas (commonly termed posterior pyramid meningiomas and/or meningiomas of the pos- terior surface of the petrous pyramid) are the most common meningiomas of the posterior cranial fossa. They are locat- ed along the posterior surface of the temporal bone in the region of the cerebellopontine angle. They often mimic vestibular schwannomas, both clinically and on neuroimaging studies. Common clinical symptoms include hearing loss, cerebellar ataxia, and trigeminal neuropathy. The site of dural origin determines the direction of cranial nerve dis- placement. Total resection can be achieved in most cases with a low morbidity rate and an excellent prognosis. The authors review the surgical management of posterior petrous meningiomas. KEY WORDS • meningioma • cerebellopontine angle • skull base surgery • petrous bone Posterior fossa meningiomas comprise approximately In their series Samii and Ammirati18 used the term “pos- 10% of all intracranial meningiomas.8 Castellano and terior pyramid meningiomas” and defined them as tumors Ruggiero4 reviewed Olivecrona’s experience with treat- whose main direction of growth brings them in contact ing posterior fossa meningiomas and classified them with the posterior pyramid, irrespective of their site of based on the site of dural attachment. They described the dural attachment. They also designated those located ante- location as cerebellar convexity (10%), tentorium (30%), rior and those posterior to the internal acoustic meatus. -

The Braincase of Two Late Cretaceous Asian Multituberculates Studied by Serial Sections
The braincase of two Late Cretaceous Asian multituberculates studied by serial sections J0RN H. HURUM Hurum, J.H. 1998. The braincase of two Late Cretaceous Asian multituberculatesstudied by serial sections. -Acta Palaeontologica Polonica 43, 1, 21-52. The braincase structure of two Late Cretaceous Mongolian djadochtatherian multituber- culates Nemegtbaatar gobiensis and Chulsanbaatar vulgaris from the ?late Campanian of Mongolia is presented based on the two serially sectioned skulls and additional specimens. Reconstructions of the floor of the braincase in both taxa are given. The complete intracranial sphenoid region is reconstructed for the first time in multitubercu- lates. Cavum epiptericum is a separate space with the taenia clino-orbitalis (ossified pila antotica) as the medial wall, anterior lamina of the petrosal and possibly the alisphenoid as the lateral wall, and the basisphenoid, petrosal and possibly alisphenoid ventrally. The fovea hypochiasmatica is shallow, tuberculurn sellae is wide and more raised from the skull base than it is in the genus Pseudobolodon. The dorsal opening of the carotid canal is situated in the fossa hypophyseos. The taenia clino-orbitalis differs from the one described in Pseudobolodon and Lambdopsalis in possessing just one foramen (metoptic foramen). Compared to all extant mammals the braincase in Nemegtbaatar and Chulsan- baatar is primitive in that both the pila antotica and pila metoptica are retained. In both genera the anterior lamina of the petrosal is large with a long anterodorsal process while the alisphenoid is small. A review is given of the cranial anatomy in Nemegtbaatar and Chulsanbaatar. K e y w o r d s : Braincase structure, sphenoid complex, cavum epiptericum,Mammalia, Multituberculata,Djadochtatheria, Cretaceous, Mongolia. -

Topographical Anatomy and Morphometry of the Temporal Bone of the Macaque
Folia Morphol. Vol. 68, No. 1, pp. 13–22 Copyright © 2009 Via Medica O R I G I N A L A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl Topographical anatomy and morphometry of the temporal bone of the macaque J. Wysocki 1Clinic of Otolaryngology and Rehabilitation, II Medical Faculty, Warsaw Medical University, Poland, Kajetany, Nadarzyn, Poland 2Laboratory of Clinical Anatomy of the Head and Neck, Institute of Physiology and Pathology of Hearing, Poland, Kajetany, Nadarzyn, Poland [Received 7 July 2008; Accepted 10 October 2008] Based on the dissections of 24 bones of 12 macaques (Macaca mulatta), a systematic anatomical description was made and measurements of the cho- sen size parameters of the temporal bone as well as the skull were taken. Although there is a small mastoid process, the general arrangement of the macaque’s temporal bone structures is very close to that which is observed in humans. The main differences are a different model of pneumatisation and the presence of subarcuate fossa, which possesses considerable dimensions. The main air space in the middle ear is the mesotympanum, but there are also additional air cells: the epitympanic recess containing the head of malleus and body of incus, the mastoid cavity, and several air spaces on the floor of the tympanic cavity. The vicinity of the carotid canal is also very well pneuma- tised and the walls of the canal are very thin. The semicircular canals are relatively small, very regular in shape, and characterized by almost the same dimensions. The bony walls of the labyrinth are relatively thin. -
The Axial Skeleton Visual Worksheet
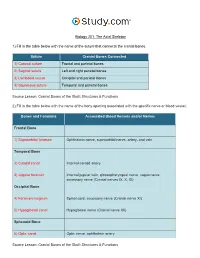
Biology 201: The Axial Skeleton 1) Fill in the table below with the name of the suture that connects the cranial bones. Suture Cranial Bones Connected 1) Coronal suture Frontal and parietal bones 2) Sagittal suture Left and right parietal bones 3) Lambdoid suture Occipital and parietal bones 4) Squamous suture Temporal and parietal bones Source Lesson: Cranial Bones of the Skull: Structures & Functions 2) Fill in the table below with the name of the bony opening associated with the specific nerve or blood vessel. Bones and Foramina Associated Blood Vessels and/or Nerves Frontal Bone 1) Supraorbital foramen Ophthalmic nerve, supraorbital nerve, artery, and vein Temporal Bone 2) Carotid canal Internal carotid artery 3) Jugular foramen Internal jugular vein, glossopharyngeal nerve, vagus nerve, accessory nerve (Cranial nerves IX, X, XI) Occipital Bone 4) Foramen magnum Spinal cord, accessory nerve (Cranial nerve XI) 5) Hypoglossal canal Hypoglossal nerve (Cranial nerve XII) Sphenoid Bone 6) Optic canal Optic nerve, ophthalmic artery Source Lesson: Cranial Bones of the Skull: Structures & Functions 3) Label the anterior view of the skull below with its correct feature. Frontal bone Palatine bone Ethmoid bone Nasal septum: Perpendicular plate of ethmoid bone Sphenoid bone Inferior orbital fissure Inferior nasal concha Maxilla Orbit Vomer bone Supraorbital margin Alveolar process of maxilla Middle nasal concha Inferior nasal concha Coronal suture Mandible Glabella Mental foramen Nasal bone Parietal bone Supraorbital foramen Orbital canal Temporal bone Lacrimal bone Orbit Alveolar process of mandible Superior orbital fissure Zygomatic bone Infraorbital foramen Source Lesson: Facial Bones of the Skull: Structures & Functions 4) Label the right lateral view of the skull below with its correct feature. -

Syndromes of the Orbital Fissure, Cavernous Sinus, Cerebello
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.2005.075259 on 16 August 2005. Downloaded from SYNDROMES OF THE ORBITAL FISSURE, CAVERNOUS SINUS, CEREBELLO- PONTINE ANGLE, AND SKULL BASE iii29 I Bone, D M Hadley J Neurol Neurosurg Psychiatry 2005;76(Suppl III):iii29–iii38. doi: 10.1136/jnnp.2005.075259 his article outlines the clinical presentation, neuroradiological approach, and the application of helpful ancillary investigations in the diagnosis of a range of cranial nerve syndromes. TThese syndromes are characterised by combinations of cranial nerve lesions that occur because of the involvement of contiguous nerves that direct investigation to a specific site. The syndromes highlight some important basic anatomy—in particular, knowledge of the contents of the cranial nerve exit/entry foramina (table 1) as well as the sites at which cranial nerves are clustered (table 2). The rate of presentation, with or without more widespread neurological or systemic involvement, hints at the particular pathological process at play. Advances in neuroimaging mean that the clinician and neuroradiologist have a range of available modalities to choose from. Discussion and appropriate selection of these is essential to accurate diagnosis and correct management. Magnetic resonance (MR) imaging is the modality of choice to depict many of the lesions involved in producing these syndromes based on their water content and molecular environment. Data can be acquired in multiple planes with differing contrast and is especially useful for showing soft tissue anatomy and pathology. There is now also widespread availability of spiral (helical) volume computed tomography (CT) where high definition planes or surfaces can be reconstructed to produce detailed depiction of bone, contrast filled vessels, and enhancing soft tissues based on their differences in electron density.