Annual Report & Accounts
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Guide to Being a Perioperative Nurse Foreword Contents
HEALTH AND SOCIAL CARE OF NORTHERN IRELAND A GUIDE TO BEING A PERIOPERATIVE NURSE FOREWORD CONTENTS Section 1: Benefits of Working in Health Care P5 Section 2: Working and Living in Northern Ireland P6 Perioperative Nursing Section 3: P7 ─ 10 • Belfast Health and Social Care Trust • Northern Health and Social Care Trust • South Eastern Health and Social Care Trust A few words from the Chief Nursing Officer, You as a Registered Nurse or as a Nursing Assistant / • Southern Health and Social Care Trust Professor Charlotte McArdle Senior Nursing Assistant will have a key role to play and I know you will contribute a lot to the care of our citizens • Western Health and Social Care Trust ‘I am delighted that you are reading this brochure and and you will also be rewarded with an exciting career already considering the exciting possibility of working with and a new extended family. us. Northern Ireland (NI) is a fabulous place to live, nurse and learn. You can have a wonderful and fulfilling career There are lots of opportunities for career development as Section 4: Perioperative Nursing Career Pathway P11 12 in Nursing within the Health and Social Care (HSC) family part of our transformation programme Delivering Together ─ and at the same time find plenty of time for an active and the Rebuilding Programme Strategic Framework lifestyle. Our people are our greatest strength. which looks to an exciting future for HSC in NI. Section 5: What our Patients Say P13 This includes new nursing roles, extended practice and continuous learning and development. I hope that you There are lots of find the brochure informative and that it encourages you opportunities for career to take the next step in developing your nursing career Section 6: Nursing Testimonials P14 20 with us in NI, a great place to live, work and have an ─ development.. -

Dr.Michelle Stephens
DR.MICHELLE STEPHENS 22 WHEATCROFT GARDENS • SHEFFIELD • SOUTH YORKSHIRE • S36 6GA PHONE: 07908955614 • E-MAIL: [email protected] WWW.MICHELLESTEPHENS.CO.UK QUALIFICATIONS 2015 - 19: Practice-based PhD, “Coded Cloth: How a generative digital design process for jacquard weave can reanimate historical pattern archives”, MMU, Manchester 2015: PGCLTHE – ILTA, MMU, Manchester, Associate Fellow of the HEA 2013 - 14: M.A. Textile Practice, Distinction, Manchester Metropolitan University, Manchester 2006 - 10: B.A. (Hons) Fine & Applied Arts, Textile Art, First Class Honours, University of Ulster, Belfast 2008 - 09: Diploma in Area Studies (Business Education Initiative), College of Saint Elizabeth, NJ 2005 - 06: Foundation Studies in Art and Design (Pass with Commendation), University of Ulster, Belfast EMPLOYMENT HISTORY 2018 – Current: 3D Weaving Research Technician, 3D Weaving Innovation Centre, University of Leeds, Leeds 2014 - Current: Part Time Lecturer, Textiles in Practice, Manchester Metropolitan University, Manchester 2010 - 15: Part Time Lecturer, Textile Design, University of Ulster, Belfast 2012 - 14: Workshop Facilitator, Island Arts Centre, Lisburn 2012 - 14: Workshop Facilitator, Atlas Women’s Group, Lisburn 2010 - Current: Visiting Textile Designer at the University of Ulster, Belfast 2011 - 14: Workshop Facilitator, Dromore Nursery School, Dromore 2012: Workshop Facilitator, St Aloysius PS, Lisburn 2012: Workshop Facilitator: 6 week program. Oakwood Integrated PS, Lisburn 2010 - 12: Weave Workshop Facilitator, Ulster Folk and Transport Museum, Cultra 2011: Textile Workshop Facilitator, Irish Linen Centre, Lisburn 2007 - 11: Art Facilitator, Friendly Faces, Lurgan 2008 - 09: Gallery Assistant, Malony Art Gallery, College of Saint Elizabeth, NJ 2007: Art Workshops: Individually Themed Projects, 6 week program. Pineview Day Nursery, Lurgan 2007: Art Workshop: Mixed media. -

Minutes of the Proceedings of a Meeting of Held in the , on At
PC 08.05 2017 LISBURN & CASTLEREAGH CITY COUNCIL Minutes of Meeting of the Planning Committee held in the Council Chamber, Lisburn & Castlereagh City Council Offices, Island Civic Centre, The Island, Lisburn on Monday 8 May 2017 at 2.20 pm PRESENT: Councillor A Redpath (Chairman) Councillor N Anderson (Vice-Chairman) Aldermen J Dillon MBE JP, G Rice MBE Councillors T Beckett, A Girvin, U Mackin, L Poots OTHER The Right Worshipful the Mayor, MEMBERS: Councillor R B Bloomfield Councillor A Grehan IN ATTENDANCE: Lead Head of Planning & Building Control Principal Planning Officers (RH and LJ) Senior Planning Officers (RT and AS,) Planning Officers (MB and KM) Committee Secretary Attendance Clerk Cleaver Fulton & Rankin Louise Coll (Legal Adviser) A&L Goodbody Micaela Diver (Legal Adviser) Commencement of Meeting In the absence of the Chairman, the Vice-Chairman, Councillor N Anderson, welcomed everyone to the meeting. Introductions were made by the Vice-Chairman and some housekeeping and evacuation announcements were made by the Lead Head of Service (Planning & Building Control). 1. Apologies Apologies for non-attendance at the Meeting were accepted and recorded on behalf of Alderman D Drysdale and Councillor M Tolerton. It was noted that the Chairman, Councillor A Redpath, would be arriving later in the meeting. 454 PC 08.05 2017 2. Declarations of Interest The Vice-Chairman sought Declarations of Interest from Members and reminded them to complete the supporting forms which had been left at each desk. The following Declarations of Interest were made: o Alderman WJ Dillon declared an interest in Application No LAO5/2016/0542F and indicated that he would be speaking in support of the application. -

Census of Drug & Alcohol Treatment Services in Northern Ireland
Census of Drug and Alcohol Treatment Services inLifestyle Northern Ireland – 1st March 2017 st Published 1 August 2017 Census of Drug and Alcohol Treatment Services in Northern Ireland – 1st March 2017 Author: Deirdre Corrigan Public Health Information & Research Branch, Information Analysis Directorate Department of Health Castle Buildings, Belfast BT4 3SQ Tel: 02890 522 523 Ext: 22523 Email: [email protected] http://www.health-ni.gov.uk © Crown Copyright 2017. Published with the permission of the Controller of Her Majesty’s Stationary Office. This publication is Crown copyright and may be reproduced free of charge in any format or medium. Any material used must be acknowledged and the title of the publication specified. Statistics and research for the Department of Health is provided by Information Analysis Directorate (IAD). It comprises four statistical sections: Hospital Information, Community Information, Public Health Information & Research and Project Support Analysis. IAD is responsible for compiling, processing, analysing, interpreting and disseminating a wide range of statistics covering health and social care. The statisticians within IAD are out-posted from the Northern Ireland Statistics & Research Agency (NISRA) and our statistics are produced in accordance with the principles and protocols set out in the Code of Practice for Official Statistics. About Public Health Information and Research Branch The role of Public Health Information and Research Branch (PHIRB) is to support the public health survey function and to provide support on public health issues within the Department. The head of the branch is the Principal Statistician, Mr. Bill Stewart. In support of the public health survey function, PHIRB is involved in the commissioning, managing and publishing of results from departmental funded surveys, such as the Health Survey Northern Ireland, All Ireland Drug Prevalence Survey, Young Persons Behaviour & Attitudes Survey, and the Adult Drinking Patterns Survey. -

The Care of Older People in Acute Hospitals
Theatre Practice Heading Regulation and Quality Improvement Authority The Care of Older People in Acute Hospitals Place your message here. For maximum impact, use two or three sentences. Unannounced inspection Lagan Valley Hospital South Eastern Health and Social Care Trust 13 & 14 November 2013 The Regulation and Quality Improvement Authority The Regulation and Quality Improvement Authority (RQIA) is the independent body responsible for regulating and inspecting the quality and availability of health and social care (HSC) services in Northern Ireland. RQIA’s reviews and inspections are designed to identify best practice, to highlight gaps or shortfalls in services requiring improvement and to protect the public interest. This inspection was carried out by a team of RQIA inspectors as part of a programme of inspections to inform the RQIA thematic review of the care of older people in acute hospitals. This review was identified and scheduled within the RQIA three year review programme for 2012 to 2015. Membership of the Team Lead Director David Stewart Review Lead / Head of Programme Liz Colgan Project Manager/Inspector Mary McClean Inspector Sheelagh O’Connor Inspector Lyn Gawley Inspector Thomas Hughes Inspector Margaret Keating Inspector Linda Thompson Lay Reviewer Ann Brooks RQIA Project Administrator Anne McKibben Contents 1.0 Summary 1 2.0 Introduction 4 2.1 Background and Methodology 4 2.2 Terms of Reference 5 3.0 Inspection Format 6 3.1 Unannounced Inspection Process 6 3.2 Reports 7 3.3 Escalation 7 4.0 Inspection Team Findings 8 4.1 Ward Governance 8 4.2 Ward Observations (Treating older People with compassion 16 dignity, and respect). -

Hospital Name Country Location
Hospital Name Country Location 1 Tameside Hospital NHS Foundation Trust England Ashton-under-Lyne 2 Barnsley Hospital NHS Foundation Trust England Barnsley 3 Royal National Hospital for Rheumatic Diseases England Bath 4 Royal United Hospitals Bath NHS Foundation Trust England Bath 5 Bedford Hospital NHS Trust England Bedford 6 South Central Ambulance Service NHS Foundation Trust England Bicester 7 Wirral Community NHS Trust England Birkenhead 8 Birmingham Children's Hospital NHS Foundation Trust England Birmingham 9 Heart Of England NHS Foundation Trust England Birmingham 10 Sandwell and West Birmingham Hospitals NHS Trust England Birmingham 11 University Hospital Birmingham NHS Foundation Trust England Birmingham 12 Birmingham and Solihull Mental Health NHS Foundation Trust England Birmingham 13 Birmingham Community Healthcare NHS Foundation Trust England Birmingham 14 Birmingham Women's NHS Foundation Trust England Birmingham 15 The Royal Orthopaedic Hospital NHS Foundation Trust England Birmingham 16 Blackpool Teaching Hospitals NHS Foundation Trust England Blackpool 17 Bolton NHS Foundation Trust England Bolton 18 The Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust England Bournmouth 19 Poole Hospital NHS Foundation Trust England Bournmouth 20 Bradford Teaching Hospitals NHS Foundation Trust England Bradford 21 Bradford District NHS Foundation Trust England Bradford 22 South East Coast Ambulance Service NHS Foundation Trust England Bridgwater 23 Sussex Community NHS Foundation Trust England Brighton 24 Brighton and -

Locality Planning for Lisburn South and Castlereagh East Deas
Locality Planning for Lisburn South and Castlereagh East DEAs Projects and Investments by Lisburn and Castlereagh Strategic Community Planning Partnership Partners January 2021 Locality Planning for Lisburn South and Castlereagh East DEAs Contents Page Introduction 3 Partners’ Projects and Investments ➢ Belfast Health and Social Care Trust 4 ➢ Council for Catholic Maintained Schools 10 ➢ Education Authority 12 ➢ Invest NI 17 ➢ Libraries NI 19 ➢ Lisburn and Castlereagh City Council – Economic Development Unit 22 ➢ Lisburn and Castlereagh City Council – Parks Department (Castlereagh East) 29 ➢ Lisburn and Castlereagh City Council – Parks Department (Lisburn South) 32 ➢ Northern Ireland Fire and Rescue Service 33 ➢ Northern Ireland Housing Executive (Castlereagh East) 35 ➢ Northern Ireland Housing Executive (Lisburn South) 37 ➢ Police Service of Northern Ireland 39 ➢ Public Health Agency 46 ➢ South Eastern Health Trust 61 ➢ South Eastern Regional College 70 ➢ Sport NI 74 ➢ Translink 76 ➢ Volunteer Now 79 ➢ Department of Education 81 ➢ Department for Infrastructure 86 Locality Planning for Lisburn South and Castlereagh East DEAs Introduction The Community Planning Partnership is engaging with the community sector to develop Locality Plans for two DEAs (District Electoral Areas) – Lisburn South and Castlereagh East. To support and inform these Plans all the partner agencies and departments involved in the Partnership were asked to provide information on their projects and/or investments in each DEA under three headings (where applicable): ➢ Support of a social nature. ➢ Physical projects. ➢ Economic support and initiatives. This document brings all the information provided by the community planning partners together in one place. Community groups in the two DEAs are invited to scroll through the document to obtain details of what the agencies and departments are doing and plan to do and to draw on this information when contributing their views on what the priorities in the Locality Plans should be. -

Newry, Mourne & Down District Council
NEWRY, MOURNE & DOWN DISTRICT COUNCIL NMC/SC Minutes of Special Council Meeting held on 22 October 2018 at 6pm in the Mourne Room, Downshire Civic Centre, Downpatrick In the Chair: Councillor M Murnin In attendance: (Councillors) Councillor T Andrews Councillor R Burgess Councillor P Byrne Councillor C Casey Councillor W Clarke Councillor C Enright Councillor G Hanna Councillor H Harvey Councillor T Hearty Councillor R Howell Councillor M Larkin Councillor K Loughran Councillor J Macauley Councillor D McAteer Councillor O McMahon Councillor Mulgrew Councillor B Quinn Councillor H Reilly Councillor J Rice Councillor M Ruane Councillor M Savage Councillor D Taylor Councillor JJ Tinnelly Councillor J Trainor Councillor W Walker (Officials) Mr. L Hannaway, Chief Executive Mr. J McBride, Assistant Director, Community Planning and Performance Mrs D Starkey, Democratic Services Officer Ms S Taggart, Democratic Services Officer Also in attendance: Northern Ireland Ambulance Service (NIAS) Mr. M Bloomfield, Chief Executive Mr. B McNeill, Director of Operations Southern Health and Social Care Trust Mr Shane Devlin, Chief Executive Mrs Melanie McClements, Director of Older People & Primary Care Services Mrs Charlene Stoops, Assistant Director of Corporate Planning South Eastern Health and Social Care Trust Roisin Coulter, Director of Planning, Performance and Informatics Seamus McGoran, Director of Hospital Services Claire Campbell, Planning Manager, Engagement and Involvement Lead SC/35/2018 APOLOGIES AND CHAIRPERSON’S REMARKS Apologies were received from Councillors Carr, Craig, Curran, Devlin, Fitzpatrick, Harte, McMurray, Sharvin and Stokes. SC/36/2018 DECLARATIONS OF INTEREST There were no Declarations of Interest. The Chairman welcomed everyone to the meeting and advised there would be a question and answer session following each of the three presentations. -

Ulster Hospital 9 – 12 February 2016 Ward 13 Medical Ward 11
Acute Hospital Inspection: Ulster Hospital 9 – 12 February 2016 Ward 13 Medical Ward 11 Surgical Emergency Department www.rqia.org.uk Assurance, Challenge and Improvement in Health and Social Care 93721 RQIA Coloured Report Template (Hygiene Team).indd 1 26/01/2016 13:58 The Regulation and Quality Improvement Authority The Regulation and Quality Improvement Authority (RQIA) is the independent body responsible for regulating and inspecting the quality and availability of health and social care (HSC) services in Northern Ireland. RQIA’s reviews and inspections are designed to identify best practice, to highlight gaps or shortfalls in services requiring improvement and to protect the public interest. Our Acute Hospital Inspections are carried out by a dedicated team of inspectors, from our Healthcare Team supported by lay assessors and peer reviewers from all trusts who have the relevant experience and knowledge. Our reports are available on the RQIA’s website at www.rqia.org.uk. RQIA wishes to thank those (including patients, their families and HSC staff) who facilitated this inspection through participating in interviews, or providing relevant information. Background In April 2014, the Minister for Health asked RQIA to put in place appropriate arrangements to deliver a rolling programme of unannounced inspections of the quality of services in acute hospitals in Northern Ireland to commence in 2015. In a statement to the Northern Ireland Assembly on 1 July 2014, the Minister indicated that the programme of inspections would focus on a selection of quality indicators that would not be pre-notified to the trusts. No advance warning is provided to trusts as to which sites, or services within a hospital, will be visited as part of an unannounced inspection. -
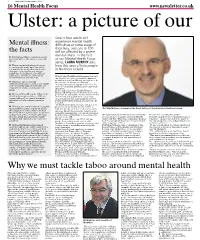
Why We Must Tackle Taboo Around Mental Health
16 News Letter, Tuesday, January 11, 2011 16 Mental Health Focus www.newsletter.co.uk Ulster: a picture of our poor state of mind One in four adults will experience mental health Mental illness: difficulties at some stage of their lives, and one in 100 the facts will be affected by a severe n It is believed that a variety of factors mental illness. In the first can contribute to the onset of a mental of our Mental Health Focus illness series, LAURA MURPHY asks n These can include physical causes i.e. our genetic make-up, if we suffer how this issue affects people a trauma to the brain (this can lead to in Northern Ireland changes in personality and ‘trigger’ symptoms of an illness), if we misuse substances, or if we are deficient in IN 1948, the World Health Organisation said certain vitamins and minerals that health “is a state of complete physical, mental and social wellbeing, and not merely n There are also social and the absence of disease or infirmity.” environmental causes, such as our family In today’s pressured, fast-paced society, the and community support networks, our state of our mental health is more important employment status, and standard of than ever. living At the end of last year, Health Minister Michael McGimpsey said that mental health n Our mental health can be influenced problems are among the most common forms by our psychological state i.e. if we are of ill health and disability in our society. coping with past or current traumatic “It is estimated that approximately 280,000 experiences such as bereavement or people in Northern Ireland are affected,” he abuse revealed. -

Laura Mccoy Report Lisburn and Castlereagh City Parking Strategy
Lisburn and Castlereagh City Parking Strategy Stage 4 - Parking Strategy and Action Plan Lisburn and Castlereagh City Council Project number: 60539778 13 September 2018 Prepared for: Lisburn and Castlereagh City Council Prepared by: Laura McCoy Graduate Consultant T: 028 9060 7200 E: [email protected] AECOM Limited The Studio Cleaver House 1-3 Donegall Square North Belfast BT1 5YE United Kingdom T: +44 28 9060 7200 aecom.com © 2018 AECOM Limited. All Rights Reserved. This document has been prepared by AECOM Limited (“AECOM”) for sole use of our client (the “Client”) in accordance with generally accepted consultancy principles, the budget for fees and the terms of reference agreed between AECOM and the Client. Any information provided by third parties and referred to herein has not been checked or verified by AECOM, unless otherwise expressly stated in the document. No third party may rely upon this document without the prior and express written agreement of AECOM. Prepared for: Lisburn and Castlereagh City Council AECOM Table of Contents 1. Introduction .................................................................................................................................................. 6 1.1 Parking Strategy Stages ................................................................................................................... 6 2. Baseline Review and Consultation............................................................................................................... 7 2.1 Introduction ...................................................................................................................................... -

6 June 2019 Chairman
6 June 2019 Chairman: Alderman A G Ewart MBE Vice-Chairman: Alderman W J Dillon MBE Aldermen: J Baird, D Drysdale, A Grehan and T Morrow Councillors: N Anderson, R T Beckett, S Carson, J Gallen, D Honeyford, H Legge, U Mackin, T Mitchell and G McCleave Ex Officio The Right Worshipful the Mayor, Councillor A Givan Deputy Mayor, Councillor J McCarthy A meeting of the Development Committee will be held in the Island Civic Centre, The Island, Lisburn, on Tuesday, 11 June 2019 at 7.00 pm for the transaction of business on the undernoted Agenda. You are requested to attend. DAVID BURNS Chief Executive Lisburn & Castlereagh City Council Agenda 1 Apologies 2 Declarations of Interest (i) Conflict of Interest on any matter before the meeting (Members to confirm the specific item) (ii) Pecuniary and non-pecuniary interest (Member to complete the Disclosure of Interest form) 3 Report of the Director of Service Transformation 3.1 Review of Work of the Committee 3.2 Report of the Head of Economic Development 3.2.1 Lisburn Castlereagh Car Park Strategy 3.2.2 Lisburn City Centre Masterplan Update & Consultation Approach 3.2.3 Lisburn Linkages Public Realm Scheme Proposed Amendments 3.2.4 Urban Regeneration Programme Review 3.2.5 Pocket Parks & Environmental Improvements Update 3.2.6 Invitation to BDUK Conference 4 Confidential Business Members are requested to go to the Confidential Folder to access the Development Committee confidential report. Confidential Report by Director of Service Transformation 4.1 Lisburn Public Realm Scheme Update on Adjudication