Integrated Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Folate and Pterin Metabolism by Cancer Cells in Culture1
[CANCER RESEARCH 38, 2378-2384, August 1978) 0008-5472/78/0038-0000$02.00 Folate and Pterin Metabolism by Cancer Cells in Culture1 Baldassarre Stea, Peter S. Backlund, Jr., Phillip B. Berkey, Arthur K. Cho, Barbara C. Halpern, Richard M. Halpern, and Roberts A. Smith2 Departments of Chemistry (B. S., P. S. B., P. B. B., B. C. H.¡,Pharmacology ¡A.K. C.], Medicine, ¡Ft.M. H.]. and Chemistry [Ft. A. SJ and Molecular Biology Institute ¡R.M. H., R. A. S.], University of California, Los Angeles, California 90024 ABSTRACT cells, a significant peak of radioactivity was observed in the blue-fluorescent region. This peak of radioactivity was ab Malignant cells grown in culture excrete into their sent in chromatograms of growth media of normal cells growth medium a folate catabolite that can be seen as a grown under the same conditions. blue-fluorescent region on paper chromatograms of such We tentatively identified this blue-fluorescent compound media. This folate catabolite has now been identified by as Pt-6-CHO,3 primarily on the basis of its inhibitory power paper chromatography, thin-layer chromatography, and toward xanthine oxidase. However, we later found that Pt- combined gas chromatography-mass spectrometry as 6- 6-CH2OH also is a potent inhibitor of the same enzyme hydroxymethylpterin and not as pterin-6-carboxaldehyde system. This prompted us to identify by unequivocal means as previously reported. the fluorescent folate catabolite characteristic of cultured Moreover, when pterin-6-carboxaldehyde was added to malignant cells. the growth medium of logarithmically growing malignant Here we report the definitive identification of this blue- cells, it was primarily reduced to 6-hydroxymethylpterin. -

Relevance to Neurological Damage
Postgrad Med J: first published as 10.1136/pgmj.62.724.113 on 1 February 1986. Downloaded from Postgraduate Medical Journal (1986) 62, 113-123 Pteridines and mono-amines: relevance to neurological damage I. Smith, D.W. Howells and K. Hyland Institute ofChildHealth (University ofLondon), 30 Guilford Street, London WCIN2NR, UK. Summary: Patients with phenylalanine hydroxylase deficiency show increased concentrations of biopterins and neopterins, and reduced concentrations ofserotonin and catecholamines, when phenylalan- ine concentrations are raised. The pterin rise reflects increased synthesis of dihydroneopterin and tetrahydrobiopterin, and the amine fall a reduction in amine synthesis due to inhibition by phenylalanine of tyrosine and typtophan transport into neurones. The pterin and amine changes appear to be independent of each other and are present in the central nervous system as well as the periphery; they disappear when phenylalanine concentrations are reduced to normal. Patients with arginase deficiency show a similar amine disturbance but have normal pterin levels. The amine changes probably contribute neurological symptoms but pterin disturbance is not known to affect brain function. Patients with defective biopterin metabolism exhibit severely impaired amine synthesis due to tetrahydrobiopterin deficiency. Pterin concentrations vary with the site of the defect. Symptoms include profound hypokiesis and other features of basal ganglia disease. Neither symptoms nor amine changes are relieved by controlling phenylalanine concentrations. Patients with dihydropteridine reductase (DHPR) deficiency accumulate dihydrobiopterins and develop secondary folate deficiency which resembles that occurring in patients with defective 5,10-methylene tetrahydrofolate reductase activity. The latter disorder is also associated writh Parkinsonisn and defective amine and pterin turnover in the and a occurs in In central nervous system, demyelinating illness both disorders. -

34Th International Winter Workshop Clinical, Chemical and Biochemical
DOI 10.1515/pterid-2015-0007 Pteridines 2015; 26(3): 113–133 Abstracts*) 34th International Winter Workshop Clinical, Chemical and Biochemical Aspects of Pteridines and Related Topics Society for Exploitation of Education and Research in Immunology and Infectious Diseases, Innsbruck, Austria in collaboration with The International Society of Pteridinology and The Austrian Society of Laboratory Medicine and Clinical Chemistry Held in Innsbruck, Tyrol, Austria, February 24th–27th, 2015 Scientific committee: Dietmar Fuchs (Innsbruck), Andrea Griesmacher (Innsbruck), Bohuslav Melichar (Olomouc), Gilbert Reibnegger (Graz), Barbara Strasser (Hall), Guenter Weiss (Innsbruck) and Ernst R. Werner (Innsbruck) Organization: Dietmar Fuchs, Sektion für Biologische Chemie, Biozentrum, Medizinische Universität Innsbruck, Innrain 80, 6020 Innsbruck, Austria, e-mail: [email protected] *)These abstracts have been reproduced directly from the material supplied by the authors, without editorial alteration by the staff of this Journal. Insufficiencies of preparation, grammar, spelling, style, syntax, and usage are the authors’ responsibility. 114 34th International Winter Workshop Circulating neopterin and citrulline concentrations Influence of carbon nanotubes, ZnO and in patients with germ-cell tumors during gold-doped TiO2 nanoparticles on human PBMC chemotherapy in vitro Bartoušková M, Študentová H, Pejpková I, Zezulová M, Adam T, Becker K, Herlin N, Bouhadoun S, Gostner JM, Ueberall F, Schennach Melichar B H, Fuchs D Palacký University Medical School and Teaching Hospital, Olomouc, Divisions of Biological Chemistry and of Medical Biochemistry, Czech Republic Biocenter, Medical University, and Central Institute of Blood ([email protected]) Transfusion and Immunology, University Hospital, Innsbruck, Austria; Au Service des Photons, Atomes et Molécules - Laboratoire Francis Germ-cell tumors are relatively rare neoplasms that affect mostly Perrin, Gif-sur Yvette, France young adults. -

A Simple and Useful Method for Evaluation of Oxidative Stress in Vivo
www.nature.com/scientificreports OPEN A simple and useful method for evaluation of oxidative stress in vivo by spectrofuorometric estimation of urinary pteridines Ichiro Wakabayashi1*, Mamoru Nakanishi2, Makoto Ohki2, Akira Suehiro3 & Kagehiro Uchida2,4 Pteridine derivatives are intermediate metabolites of folic acid and its cofactors. Oxidized-form pteridines, but not reduced-form pteridines, are fuorescent substances. The purpose of this study was to clarify whether oxidized-form pteridine level in urine, estimated by spectrofuorometry, refects oxidative stress in vivo. The subjects were healthy middle-aged men (n = 258). Urinary pteridine level was estimated by spectrofuorometry with an excitation wavelength of 360 nm and an emission wavelength of 450 nm. Relationships of urinary pteridines with oxidative stress markers (urinary DNA/ RNA oxidation products and 15-isoprostane F 2t) and with smoking were analyzed. Concentrations of pteridines, DNA/RNA oxidation products and 15-isoprostane F 2t were used after logarithmic transformation in linear analyses. Pteridine levels were signifcantly correlated with levels of DNA/ RNA oxidation products (Pearson’s correlation coefcient: 0.626, p < 0.01) and 15-isoprostane F2t (Pearson’s correlation coefcient: 0.695, p < 0.01). These correlations were not confounded by age, body mass index, history of smoking and estimated glomerular fltration rate in multivariate analysis. The mean urinary pteridine level was signifcantly higher in heavy smokers (16 cigarettes or more per day) than in nonsmokers and light smokers (less than 16 cigarettes per day) and was higher in light smokers than in nonsmokers. Thus, urinary fuorometric pteridine levels were shown to be associated with known biomarkers of oxidative stress as well as smoking, which causes oxidative stress in vivo. -

Metabolic Engineering of the Pterin Branch of Folate Synthesis by Over-Expression of a GTP Cyclohydrolase I in Peanut
Metabolic engineering of the pterin branch of folate synthesis by over-expression of a GTP cyclohydrolase I in peanut Nicole Czarina Juba Dissertation submitted to the faculty of Virginia Polytechnic Institute and State University in partial fulfillment of the requirement for the degree of Doctor of Philosophy in Plant Pathology, Physiology and Weed Science Elizabeth A. Grabau, Chair Amy M. Brunner Steven L. Rideout James H. Westwood October 14th, 2011 Blacksburg, VA Keywords: Arachis hypogaea, peanut, folate, biofortification, GTP cyclohydrolase I, LC/MS/M Metabolic engineering of the pterin branch of folate synthesis by over-expression of a GTP cyclohydrolase I in peanut Nicole Czarina Juba Abstract Folate, also known as vitamin B9, is an essential dietary vitamin that provides the donor group for one carbon transfer reactions. Deficiency in folate is associated with neural tube birth defects (NTDs), cancer, cardiovascular disease, and anemia. In the US enriched food products including bread, pasta, and cereal are fortified with folic acid, the synthetic analog of folate. While effective in reducing NTDs, this practice is costly and not economically practical in developing countries. Folate biofortification, increasing the natural folate level in foods by metabolic engineering, has been proposed as a sustainable alternative to food fortification with folic acid. To increase folate levels in peanut seed, GTP cyclohydrolase I from Arabidopsis thaliana (AtGCHI) was introduced into peanut by biolistic transformation. Plant transformation vectors were constructed using publicly available or licensable vector components to avoid intellectual property restrictions that hinder commercialization. Thirteen peanut cultivars were evaluated for transformation efficiencies and regeneration potential. Expression levels of the AtGCHI transgene were determined by quantitative real-time PCR. -

GTP-Cyclohydrolase I Deficiency Presenting
Dayasiri et al. BMC Pediatrics (2019) 19:199 https://doi.org/10.1186/s12887-019-1580-x CASE REPORT Open Access GTP-Cyclohydrolase I deficiency presenting as malignant hyperphenylalaninemia, recurrent hyperthermia and progressive neurological dysfunction in a South Asian child – a case report Kavinda Chandimal Dayasiri1*, Nayani Suraweera1, Deepal Nawarathne1, U. E. Senanayake2, B. K. T. P. Dayanath2, Eresha Jasinge1 and Kumudu Weerasekara1 Abstract Background: Tetrahydrobiopterin (BH4) deficiencies are disorders affecting phenylalanine homeostasis, and catecholamine and serotonin biosynthesis. GTP-Cyclohydrolase I deficiency (OMIM 600225) is an extremely rare variant of inborn error of BH4 synthesis which exists in recessive and dominant forms. The recessive form presents with complex neurological and autonomic dysfunction whilst the dominant form presents as Dopa-responsive dystonia. Case presentation: We describe a South Asian child who initially presented with neurological dysfunction and recurrent vomiting and later developed recurrent hyperthermia for several months. The child did not have screening for hyperphenylalaninemia at birth and was found to have marked hyperphenylalaninemia after clinical presentation at 5 months. Further evaluation revealed BH4 deficiency. GTP-Cyclohydrolase I deficiency (GTPCH) was identified based on normal dihydro pteridine reductase activity and markedly reduced neopterin in dried blood spot test. After institution of treatment and control of high phenylalanine levels, clinical deterioration decelerated yet with noticeable residual neurological dysfunction. Conclusion: To authors’ knowledge, this is first report of GTPCH deficiency in a South Asian child. The case highlights practical issues regarding diagnosis of GTPCH deficiency, especially in countries without broader universal newborn screening programs for early detection of inherited metabolic disorders. Testing for GTPCH deficiency should be considered for patients with unexplained neurological and autonomic symptoms following initial metabolic screen. -

Analysis of Catecholamines and Pterins in Inborn Errors of Monoamine Neurotransmitter Metabolism—From Past to Future
cells Review Analysis of Catecholamines and Pterins in Inborn Errors of Monoamine Neurotransmitter Metabolism—From Past to Future Sabine Jung-Klawitter * and Oya Kuseyri Hübschmann Department of General Pediatrics, Division of Neuropediatrics and Metabolic Medicine, University Hospital Heidelberg, 69120 Heidelberg, Germany * Correspondence: [email protected]; Tel.: +49-(0)6221-5639586 Received: 30 June 2019; Accepted: 4 August 2019; Published: 9 August 2019 Abstract: Inborn errors of monoamine neurotransmitter biosynthesis and degradation belong to the rare inborn errors of metabolism. They are caused by monogenic variants in the genes encoding the proteins involved in (1) neurotransmitter biosynthesis (like tyrosine hydroxylase (TH) and aromatic amino acid decarboxylase (AADC)), (2) in tetrahydrobiopterin (BH4) cofactor biosynthesis (GTP cyclohydrolase 1 (GTPCH), 6-pyruvoyl-tetrahydropterin synthase (PTPS), sepiapterin reductase (SPR)) and recycling (pterin-4a-carbinolamine dehydratase (PCD), dihydropteridine reductase (DHPR)), or (3) in co-chaperones (DNAJC12). Clinically, they present early during childhood with a lack of monoamine neurotransmitters, especially dopamine and its products norepinephrine and epinephrine. Classical symptoms include autonomous dysregulations, hypotonia, movement disorders, and developmental delay. Therapy is predominantly based on supplementation of missing cofactors or neurotransmitter precursors. However, diagnosis is difficult and is predominantly based on quantitative detection of neurotransmitters, cofactors, and precursors in cerebrospinal fluid (CSF), urine, and blood. This review aims at summarizing the diverse analytical tools routinely used for diagnosis to determine quantitatively the amounts of neurotransmitters and cofactors in the different types of samples used to identify patients suffering from these rare diseases. Keywords: inborn errors of metabolism; catecholamines; pterins; HPLC; fluorescence detection; electrochemical detection; MS/MS 1. -

Structural and Functional Characterization of the Intracellular Filament-Forming Nitrite Oxidoreductase Multiprotein Complex
ARTICLES https://doi.org/10.1038/s41564-021-00934-8 Structural and functional characterization of the intracellular filament-forming nitrite oxidoreductase multiprotein complex Tadeo Moreno Chicano1,8, Lea Dietrich2,8, Naomi M. de Almeida3,8, Mohd. Akram1, Elisabeth Hartmann1, Franziska Leidreiter 1, Daniel Leopoldus 1, Melanie Mueller1, Ricardo Sánchez2,4, Guylaine H. L. Nuijten3, Joachim Reimann3, Kerstin-Anikó Seifert1, Ilme Schlichting 1, Laura van Niftrik 3, Mike S. M. Jetten3, Andreas Dietl1 ✉ , Boran Kartal5,6 ✉ , Kristian Parey2,7 ✉ and Thomas R. M. Barends 1 ✉ Nitrate is an abundant nutrient and electron acceptor throughout Earth’s biosphere. Virtually all nitrate in nature is produced by the oxidation of nitrite by the nitrite oxidoreductase (NXR) multiprotein complex. NXR is a crucial enzyme in the global biologi- cal nitrogen cycle, and is found in nitrite-oxidizing bacteria (including comammox organisms), which generate the bulk of the nitrate in the environment, and in anaerobic ammonium-oxidizing (anammox) bacteria which produce half of the dinitrogen gas in our atmosphere. However, despite its central role in biology and decades of intense study, no structural information on NXR is available. Here, we present a structural and biochemical analysis of the NXR from the anammox bacterium Kuenenia stutt- gartiensis, integrating X-ray crystallography, cryo-electron tomography, helical reconstruction cryo-electron microscopy, inter- action and reconstitution studies and enzyme kinetics. We find that NXR catalyses both nitrite oxidation and nitrate reduction, and show that in the cell, NXR is arranged in tubules several hundred nanometres long. We reveal the tubule architecture and show that tubule formation is induced by a previously unidentified, haem-containing subunit, NXR-T. -
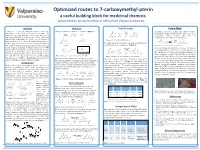
Optimized Routes to 7-Carboxymethyl-Pterin: a Useful
Optimized routes to 7-carboxymethyl-pterin a useful building block for medicinal chemists Zachary Bennett, Kassidy Grumbles, Dr. Jeffery Pruet | Valparaiso University Abstract Methods Path B Results Future Work Pterins are a class of nitrogen-heterocycle with wide Two general routes to 7-CMP were envisioned (Figure 3): O Na2SO3 O To continue this project, a third route (Path C) will be O H2O application in the field of medicinal chemistry. The NH2 O H N investigated. Similar to Path B, this route relies on a NH2 HN 30 min HN importance of pterin derivatives stems from discovery of Path A HN Path B H N N NH O H 95% regiospecific Minisci reaction, this time via H2N N NH2 2 2 H2N N N numerous biologically relevant pterins, such as folate and H2SO4 decarboxylative generation of the acyl radical. O O bioterin. Due to this biological relevance, several pterin-based N N O O HN HN Scheme 5: Synthesis of unsubstituted pterin N AgNO3 N HN O O inhibitors have been developed for various biological targets. Na2S2O8 HN H2N N N H2N N N MeO O K H2SO4 O 6-methyl regioisomer also possible The sulfate salt of the pyrimidine was condensed with glyoxal, H N N N In this regard pterins can be viewed as a privileged scaffold, as 2 H2N N N [Acyl radical insertion] removing the issue of regiosiomers (Scheme 5). O the discovery of new pterin analogs gives rise to a vast array [Oxidation] Figure 4: New route under investigation (Path C) O of potential drug candidates. -

Defect in GTP-Cyclohydrolase
Defect in GTP-cyclohydrolase Author: Professor Jean-Louis Dhondt 1 Creation Date: April 2001 Updates: May 2003 February 2005 Scientific Editor: Professor Jean-Marie Saudubray 1Centre régional de dépistage néonatal, 68 Rue Sylvere Verhulst, 59000 Lille, France. [email protected] Abstract Keywords Disease name and synonyms Excluded diseases Diagnostic criteria/definition Differential diagnosis Prevalence Clinical description Management including treatment Diagnostic methods Genetic counseling Antenatal diagnosis References Abstract GTP-cyclohydrolase I deficiency, an autosomal recessive genetic disorder, is one of the causes of malignant hyperphenylalaninemia due to tetrahydrobiopterin deficiency. Not only does tetrahydrobiopterin deficiency cause hyperphenylalaninemia, it is also responsible for defective neurotransmission of monoamines because of malfunctioning tyrosine and tryptophan hydroxylases, both tetrahydrobiopterin- dependent hydroxylases. GTP-cyclohydrolase I deficiency should be suspected in all infants with a positive neonatal screening test for phenylketonuria, especially when hyperphenylalaninemia is moderate. The most effective way to diagnose the disorder is to measure pteridine levels in urine and to confirm the result by measuring neurotransmitters (5-hydroxyindolacetic acid, homovanillic acid) in cerebrospinal fluid and with an oral tetrahydrobiopterin-loading test (20 mg/kg). When left untreated, the deficiency causes neurological signs at age 4 or 5 months, although clinical signs are often obvious -

Metabolic Effects of Sapropterin Treatment in Autism Spectrum Disorder: a Preliminary Study
Citation: Transl Psychiatry (2013) 3, e237; doi:10.1038/tp.2013.14 & 2013 Macmillan Publishers Limited All rights reserved 2158-3188/13 www.nature.com/tp Metabolic effects of sapropterin treatment in autism spectrum disorder: a preliminary study RE Frye1, R DeLaTorre2, HB Taylor3, J Slattery1, S Melnyk1, N Chowdhury1 and SJ James1 Sapropterin, a synthetic form of tetrahydrobiopterin (BH4), has been reported to improve symptoms in children with autism spectrum disorder (ASD). However, as BH4 is involved in multiple metabolic pathway that have been found to be dysregulated in ASD, including redox, pterin, monoamine neurotransmitter, nitric oxide (NO) and immune metabolism, the metabolic pathway by which sapropterin exerts its therapeutic effect in ASD effect remains unclear. This study investigated which metabolic pathways were associated with symptomatic improvement during sapropterin treatment. Ten participants (ages 2–6 years old) with current À 1 À 1 social and/or language delays, ASD and a central BH4 concentration p30 nM l were treated with a daily morning 20 mg kg dose of sapropterin for 16 weeks in an open-label fashion. At baseline, 8 weeks and 16 weeks after starting the treatment, measures of language, social function and behavior and biomarkers of redox, pterin, monoamine neurotransmitter, NO and immune metabolism were obtained. Two participants discontinued the study, one from mild adverse effects and another due to noncompliance. Overall, improvements in subscales of the Preschool Language Scale (PLS), Vineland Adaptive Behavior Scale (VABS), Aberrant Behavior Checklist (ABC) and autism symptoms questionnaire (ASQ) were seen. Significant changes in biomarkers of pterin, redox and NO were found. -

Consensus Guideline for the Diagnosis and Treatment of Tetrahydrobiopterin
Opladen et al. Orphanet Journal of Rare Diseases (2020) 15:126 https://doi.org/10.1186/s13023-020-01379-8 REVIEW Open Access Consensus guideline for the diagnosis and treatment of tetrahydrobiopterin (BH4) deficiencies Thomas Opladen1*†, Eduardo López-Laso2†, Elisenda Cortès-Saladelafont3,4†, Toni S. Pearson5, H. Serap Sivri6, Yilmaz Yildiz6, Birgit Assmann1, Manju A. Kurian7,8, Vincenzo Leuzzi9, Simon Heales10, Simon Pope10, Francesco Porta11, Angeles García-Cazorla3, Tomáš Honzík12, Roser Pons13, Luc Regal14, Helly Goez15, Rafael Artuch16, Georg F. Hoffmann1, Gabriella Horvath17, Beat Thöny18, Sabine Scholl-Bürgi19, Alberto Burlina20, Marcel M. Verbeek21, Mario Mastrangelo9, Jennifer Friedman22, Tessa Wassenberg14, Kathrin Jeltsch1†, Jan Kulhánek12*†, Oya Kuseyri Hübschmann1† and on behalf of the International Working Group on Neurotransmitter related Disorders (iNTD) Abstract Background: Tetrahydrobiopterin (BH4) deficiencies comprise a group of six rare neurometabolic disorders characterized by insufficient synthesis of the monoamine neurotransmitters dopamine and serotonin due to a disturbance of BH4 biosynthesis or recycling. Hyperphenylalaninemia (HPA) is the first diagnostic hallmark for most BH4 deficiencies, apart from autosomal dominant guanosine triphosphate cyclohydrolase I deficiency and sepiapterin reductase deficiency. Early supplementation of neurotransmitter precursors and where appropriate, treatment of HPA results in significant improvement of motor and cognitive function. Management approaches differ across the world