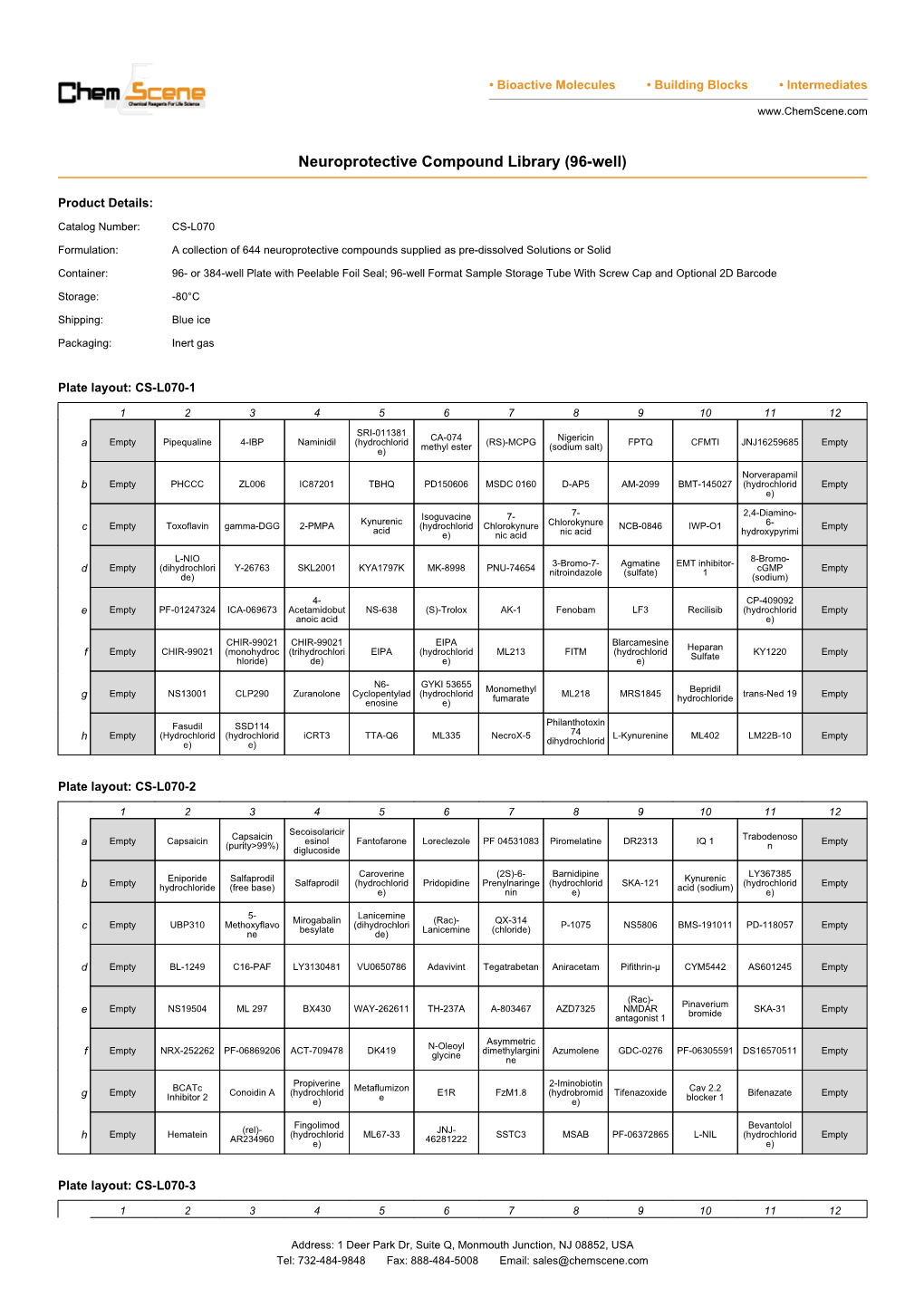
Neuroprotective Compound Library (96-Well)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
NMDA Receptor Dynamics Dictate Neuronal Plasticity and Function
NMDA Receptor Dynamics Dictate Neuronal Plasticity and Function Tommy Weiss Sadan, Ph.D. and Melanie R. Grably, Ph.D. N-Methyl-D-Aspartate Receptor (NMDAR) are ubiquitously expressed along the central nervous system and are instrumental to various physiological processes such as synaptic plasticity and learning. Nevertheless, several mental disabilities including schizophrenia and Alzheimer’s disease are all related to NMDAR dysfunction. Here, we review many aspects of NMDAR function and regulation and describe their involvement in pathophysiological states using Alomone Labs products. Right: Cell surface detection of GluN2B in rat hippocampal neurons. Introduction Mechanism of Action Glutamate is a key neuro-transmitter in the central nervous system and NMDAR activation depends on sequential conformational changes to acts on a variety of cell surface receptors, collectively termed ionotropic relieve the magnesium blockade which is achieved by rapid membrane glutamate receptors (iGluRs)15. The N-Methyl-D-Aspartate receptors (NMDAR) depolarization and binding of both glycine and glutamate ligands6, 21. This in are members of the iGluR superfamily and are pivotal to many physiological turn removes the inhibitory electrostatic forces of magnesium and enables processes such as the formation of long term memory, synaptic plasticity calcium influx and transmission of long lasting signals (i.e. long-term and many other cognitive functions. Therefore, it is not surprising that potentiation), a key mechanism to learning and memory formation10. -

Metabotropic Glutamate Receptors
mGluR Metabotropic glutamate receptors mGluR (metabotropic glutamate receptor) is a type of glutamate receptor that are active through an indirect metabotropic process. They are members of thegroup C family of G-protein-coupled receptors, or GPCRs. Like all glutamate receptors, mGluRs bind with glutamate, an amino acid that functions as an excitatoryneurotransmitter. The mGluRs perform a variety of functions in the central and peripheral nervous systems: mGluRs are involved in learning, memory, anxiety, and the perception of pain. mGluRs are found in pre- and postsynaptic neurons in synapses of the hippocampus, cerebellum, and the cerebral cortex, as well as other parts of the brain and in peripheral tissues. Eight different types of mGluRs, labeled mGluR1 to mGluR8, are divided into groups I, II, and III. Receptor types are grouped based on receptor structure and physiological activity. www.MedChemExpress.com 1 mGluR Agonists, Antagonists, Inhibitors, Modulators & Activators (-)-Camphoric acid (1R,2S)-VU0155041 Cat. No.: HY-122808 Cat. No.: HY-14417A (-)-Camphoric acid is the less active enantiomer (1R,2S)-VU0155041, Cis regioisomer of VU0155041, is of Camphoric acid. Camphoric acid stimulates a partial mGluR4 agonist with an EC50 of 2.35 osteoblast differentiation and induces μM. glutamate receptor expression. Camphoric acid also significantly induced the activation of NF-κB and AP-1. Purity: ≥98.0% Purity: ≥98.0% Clinical Data: No Development Reported Clinical Data: No Development Reported Size: 10 mM × 1 mL, 100 mg Size: 10 mM × 1 mL, 5 mg, 10 mg, 25 mg (2R,4R)-APDC (R)-ADX-47273 Cat. No.: HY-102091 Cat. No.: HY-13058B (2R,4R)-APDC is a selective group II metabotropic (R)-ADX-47273 is a potent mGluR5 positive glutamate receptors (mGluRs) agonist. -

Edison Healthcare Insight
Edison Healthcare Insight December 2020 Published by Edison Investment Research The Edison healthcare team www.edisongroup.com Maxim Jacobs Dr Nathaniel Calloway Max joined Edison’s healthcare team in December Nathaniel Calloway joined the healthcare team in 2014. Prior to this he worked as a senior analyst at December 2015. Before Edison, he performed Guidepoint Global. Max has also previously worked healthcare investment research for a fund at Bishop as a senior analyst at Ridgemark Capital, a sector Rosen and for Wainscott Capital Partners. Prior to head at Broadfin Capital and as a senior analyst at his role as an analyst he performed molecular Mehta Partners. He is a CFA charter holder. neuroscience research at Cornell Medical School and holds a PhD in chemistry from Cornell. He has published eight scientific papers on topics ranging from physical chemistry to immunology, and he has been recognised as an American Heart Association fellow and an American Chemical Society Medicinal Chemistry fellow. Pooya Hemami Dr John Savin Pooya is a licensed optometrist with over five years John is an analyst working on biotech, pharma, of experience in life sciences equity research. Prior medical device and diagnostics companies. As to joining Edison, he covered the Canadian founder CEO of Physiomics, he devised the healthcare sector as a research analyst at strategy, raised funds and took the company to AIM Desjardins Capital Markets. He holds a doctor of in 2004. At Greig Middleton, John was director in optometry degree from the University of Montreal, charge of the pharma and biotech analyst team and and an MBA (finance concentration) from McGill worked with corporate finance on fund-raising, IPOs University. -

Summary Analgesics Dec2019
Status as of December 31, 2019 UPDATE STATUS: N = New, A = Advanced, C = Changed, S = Same (No Change), D = Discontinued Update Emerging treatments for acute and chronic pain Development Status, Route, Contact information Status Agent Description / Mechanism of Opioid Function / Target Indication / Other Comments Sponsor / Originator Status Route URL Action (Y/No) 2019 UPDATES / CONTINUING PRODUCTS FROM 2018 Small molecule, inhibition of 1% diacerein TWi Biotechnology / caspase-1, block activation of 1 (AC-203 / caspase-1 inhibitor Inherited Epidermolysis Bullosa Castle Creek Phase 2 No Topical www.twibiotech.com NLRP3 inflamasomes; reduced CCP-020) Pharmaceuticals IL-1beta and IL-18 Small molecule; topical NSAID Frontier 2 AB001 NSAID formulation (nondisclosed active Chronic low back pain Phase 2 No Topical www.frontierbiotech.com/en/products/1.html Biotechnologies ingredient) Small molecule; oral uricosuric / anti-inflammatory agent + febuxostat (xanthine oxidase Gout in patients taking urate- Uricosuric + 3 AC-201 CR inhibitor); inhibition of NLRP3 lowering therapy; Gout; TWi Biotechnology Phase 2 No Oral www.twibiotech.com/rAndD_11 xanthine oxidase inflammasome assembly, reduced Epidermolysis Bullosa Simplex (EBS) production of caspase-1 and cytokine IL-1Beta www.arraybiopharma.com/our-science/our-pipeline AK-1830 Small molecule; tropomyosin Array BioPharma / 4 TrkA Pain, inflammation Phase 1 No Oral www.asahi- A (ARRY-954) receptor kinase A (TrkA) inhibitor Asahi Kasei Pharma kasei.co.jp/asahi/en/news/2016/e160401_2.html www.neurosmedical.com/clinical-research; -

Regulation of Extracellular Arginine Levels in the Hippocampus in Vivo
Regulation of Extracellular Arginine Levels in the Hippocampus In Vivo by Joanne Watts B.Sc. (Hons) r Thesis submitted for the degree of Doctor of Philosophy in the Faculty of Science, University of London The School of Pharmacy University of London ProQuest Number: 10105113 All rights reserved INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted. In the unlikely event that the author did not send a complete manuscript and there are missing pages, these will be noted. Also, if material had to be removed, a note will indicate the deletion. uest. ProQuest 10105113 Published by ProQuest LLC(2016). Copyright of the Dissertation is held by the Author. All rights reserved. This work is protected against unauthorized copying under Title 17, United States Code. Microform Edition © ProQuest LLC. ProQuest LLC 789 East Eisenhower Parkway P.O. Box 1346 Ann Arbor, Ml 48106-1346 Abstract Nitric oxide (NO) has emerged as an ubiquitous signaling molecule in the central nervous system (CNS). NO is synthesised from molecular oxygen and the amino acid L-arginine (L- ARG) by the enzyme NO synthase (NOS), and the availability of L-ARG has been implicated as the limiting factor for NOS activity. Previous studies have indicated that L- ARG is localised in astrocytes in vitro and that the in vitro activation of non-N-methyl-D- aspartate (NMDA) receptors, as well as the presence of peroxynitrite (ONOO ), led to the release of L-ARG. Microdialysis was therefore used in this study to investigate whether this held true in vivo. -

Central Valley Toxicology Drug List
Chloroform ~F~ Lithium ~A~ Chlorpheniramine Loratadine Famotidine Acebutolol Chlorpromazine Lorazepam Fenoprofen Acetaminophen Cimetidine Loxapine Fentanyl Acetone Citalopram LSD (Lysergide) Fexofenadine 6-mono- Clomipramine acetylmorphine Flecainide ~M~ Clonazepam a-Hydroxyalprazolam Fluconazole Maprotiline Clonidine a-Hydroxytriazolam Flunitrazepam MDA Clorazepate Albuterol Fluoxetine MDMA Clozapine Alprazolam Fluphenazine Medazepam Cocaethylene Amantadine Flurazepam Meperidine Cocaine 7-Aminoflunitrazepam Fluvoxamine Mephobarbital Codeine Amiodarone Fosinopril Meprobamate Conine Amitriptyline Furosemide Mesoridazine Cotinine Amlodipine Methadone Cyanide ~G~ Amobarbital Methanol Cyclobenzaprine Gabapentin Amoxapine d-Methamphetamine Cyclosporine GHB d-Amphetamine l-Methamphetamine Glutethamide l-Amphetamine ~D~ Methapyrilene Guaifenesin Aprobarbital Demoxepam Methaqualone Atenolol Desalkylfurazepam ~H~ Methocarbamol Atropine Desipramine Halazepam Methylphenidate ~B~ Desmethyldoxepin Haloperidol Methyprylon Dextromethoraphan Heroin Metoclopramide Baclofen Diazepam Hexobarbital Metoprolol Barbital Digoxin Hydrocodone Mexiletine Benzoylecgonine Dihydrocodein Hydromorphone Midazolam Benzphetamine Dihydrokevain Hydroxychloroquine Mirtazapine Benztropine Diltiazem Hydroxyzine Morphine (Total/Free) Brodificoum Dimenhydrinate Bromazepam ~N~ Diphenhydramine ~I~ Bupivacaine Nafcillin Disopyramide Ibuprofen Buprenorphine Naloxone Doxapram Imipramine Bupropion Naltrexone Doxazosin Indomethacin Buspirone NAPA Doxepin Isoniazid Butabarbital Naproxen -

Download Product Insert (PDF)
PRODUCT INFORMATION Fantofarone Item No. 26381 CAS Registry No.: 114432-13-2 Formal Name: 3,4-dimethoxy-N-methyl-N-[3-[4-[[2- N (1-methylethyl)-1-indolizinyl]sulfonyl] O phenoxy]propyl]-benzeneethanamine S O Synonym: SR 33557 MF: C31H38N2O5S FW: 550.7 Purity: ≥98% N O UV/Vis.: λmax: 233, 304 nm Supplied as: A crystalline solid O Storage: -20°C O Stability: ≥2 years Information represents the product specifications. Batch specific analytical results are provided on each certificate of analysis. Laboratory Procedures Fantofarone is supplied as a crystalline solid. A stock solution may be made by dissolving the fantofarone in the solvent of choice. Fantofarone is soluble in organic solvents such as DMSO and dimethyl formamide, which should be purged with an inert gas. The solubility of fantofarone in these solvents is approximately 10 mg/ml. Description Fantofarone is a calcium channel inhibitor.1 It selectively inhibits the L-type voltage-gated calcium channel in isolated rat aorta (IC50 = 0.61 nM) over α1- and β-adrenergic, muscarinic, and histamine H2 receptors in rat heart homogenates (IC50s = >10, >10, 4, and >10 µM, respectively), and the serotonin receptor subtypes 5-HT1 and 5-HT2, as well as histamine H1 and adenosine A1 receptors, in rat brain homogenates (IC50s = >10, 4, >10, and >10 µM, respectively). Fantofarone inhibits peak calcium current in depolarized 2 and hyperpolarized L-type voltage-gated calcium channels (IC50s = 1.4 and 150 nM, respectively). It inhibits potassium chloride- and norepinephrine-induced contractions in isolated rat aorta (IC50s = 5.64 and 96 nM, respectively).1 It enhances recovery of cardiac output during reperfusion of isolated rat hearts when used at a concentration of 10 nM.3 Fantofarone prevents angioplasty-induced vasospasms in the femoral artery in a rabbit model of focal atherosclerosis when administered at a dose of 50 µg/kg.4 References 1. -

(12) United States Patent (10) Patent No.: US 8,748,131 B2 Ford (45) Date of Patent: Jun
USOO8748131B2 (12) United States Patent (10) Patent No.: US 8,748,131 B2 Ford (45) Date of Patent: Jun. 10, 2014 (54) CHIMERIC NEUREGULINS AND METHOD in Neuregulin-1/ErbB Signaling. The Journal of Biological Chemis OF MAKING AND USE THEREOF try vol. 285, No. 41, pp. 31388-31398, Oct. 8, 2010.* Veronese et al., PEGylation. Successful approach to drug delivery. (71) Applicant: Morehouse School of Medicine, Drug Discovery Today vol. 10, No. 21 Nov. 2005, 1451-1458.* Atlanta, GA (US) Carraway et al., Neuregulin-2, a new ligand ErbB3/ErbB4-receptor tyrosine kinases. Nature, vol. 387, May 29, 1997, 512-516.* (72) Inventor: Byron D. Ford, Atlanta, GA (US) Higashiyamaet al., ANovel Brain-Derived Member of the Epidermal Growth Factor Family That Interacts with ErbB3 and ErbB4. J. (73) Assignee: Morehouse School of Medicine, Biochem. 122,675-680 (1997).* Atlanta, GA (US) Fischbach et al., “ARIA: A Neuromuscular Junction Neuregulin.” Annual Review of Neuroscience, 1997, pp. 429–458, vol. 20. (*) Notice: Subject to any disclaimer, the term of this Buonanno et al., “Neuregulin and ErbB receptor signaling pathways patent is extended or adjusted under 35 in the nervous system.” Current Opinion in Neurobiology, 2001, pp. U.S.C. 154(b) by 0 days. 287-296, vol. 11. Burden et al., “Neuregulins and Their Receptors: A Versatile Signal Appl. No.: 13/627,555 ing Module in Organogenesis and Oncogenesis. Neuron, 1997, pp. (21) 847-855, vol. 18. Fu et al., “Cdk5 is involved in neuregulin-induced AChR expression (22) Filed: Sep. 26, 2012 at the neuromuscular junction.” Nature Neuroscience, Apr. -

About Pain Pharmacology: What Pain Physicians Should Know Kyung-Hoon Kim1, Hyo-Jung Seo1, Salahadin Abdi2, and Billy Huh2
Korean J Pain 2020;33(2):108-120 https://doi.org/10.3344/kjp.2020.33.2.108 pISSN 2005-9159 eISSN 2093-0569 Review Article All about pain pharmacology: what pain physicians should know Kyung-Hoon Kim1, Hyo-Jung Seo1, Salahadin Abdi2, and Billy Huh2 1Department of Anesthesia and Pain Medicine, School of Medicine, Pusan National University, Yangsan, Korea 2Department of Pain Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX, USA Received February 8, 2020 Revised March 12, 2020 From the perspective of the definition of pain, pain can be divided into emotional Accepted March 13, 2020 and sensory components, which originate from potential and actual tissue dam- age, respectively. The pharmacologic treatment of the emotional pain component Correspondence includes antianxiety drugs, antidepressants, and antipsychotics. The anti-anxiety Kyung-Hoon Kim drugs have anti-anxious, sedative, and somnolent effects. The antipsychotics are Department of Anesthesia and Pain effective in patients with positive symptoms of psychosis. On the other hand, the Medicine, Pusan National University sensory pain component can be divided into nociceptive and neuropathic pain. Yangsan Hospital, 20 Geumo-ro, Non-steroidal anti-inflammatory drugs (NSAIDs) and opioids are usually applied for Mulgeum-eup, Yangsan 50612, Korea Tel: +82-55-360-1422 somatic and visceral nociceptive pain, respectively; anticonvulsants and antide- Fax: +82-55-360-2149 pressants are administered for the treatment of neuropathic pain with positive and E-mail: [email protected] negative symptoms, respectively. The NSAIDs, which inhibit the cyclo-oxygenase pathway, exhibit anti-inflammatory, antipyretic, and analgesic effects; however, they have a therapeutic ceiling. -

CAS Number Index
2334 CAS Number Index CAS # Page Name CAS # Page Name CAS # Page Name 50-00-0 905 Formaldehyde 56-81-5 967 Glycerol 61-90-5 1135 Leucine 50-02-2 596 Dexamethasone 56-85-9 963 Glutamine 62-44-2 1640 Phenacetin 50-06-6 1654 Phenobarbital 57-00-1 514 Creatine 62-46-4 1166 α-Lipoic acid 50-11-3 1288 Metharbital 57-22-7 2229 Vincristine 62-53-3 131 Aniline 50-12-4 1245 Mephenytoin 57-24-9 1950 Strychnine 62-73-7 626 Dichlorvos 50-23-7 1017 Hydrocortisone 57-27-2 1428 Morphine 63-05-8 127 Androstenedione 50-24-8 1739 Prednisolone 57-41-0 1672 Phenytoin 63-25-2 335 Carbaryl 50-29-3 569 DDT 57-42-1 1239 Meperidine 63-75-2 142 Arecoline 50-33-9 1666 Phenylbutazone 57-43-2 108 Amobarbital 64-04-0 1648 Phenethylamine 50-34-0 1770 Propantheline bromide 57-44-3 191 Barbital 64-13-1 1308 p-Methoxyamphetamine 50-35-1 2054 Thalidomide 57-47-6 1683 Physostigmine 64-17-5 784 Ethanol 50-36-2 497 Cocaine 57-53-4 1249 Meprobamate 64-18-6 909 Formic acid 50-37-3 1197 Lysergic acid diethylamide 57-55-6 1782 Propylene glycol 64-77-7 2104 Tolbutamide 50-44-2 1253 6-Mercaptopurine 57-66-9 1751 Probenecid 64-86-8 506 Colchicine 50-47-5 589 Desipramine 57-74-9 398 Chlordane 65-23-6 1802 Pyridoxine 50-48-6 103 Amitriptyline 57-92-1 1947 Streptomycin 65-29-2 931 Gallamine 50-49-7 1053 Imipramine 57-94-3 2179 Tubocurarine chloride 65-45-2 1888 Salicylamide 50-52-2 2071 Thioridazine 57-96-5 1966 Sulfinpyrazone 65-49-6 98 p-Aminosalicylic acid 50-53-3 426 Chlorpromazine 58-00-4 138 Apomorphine 66-76-2 632 Dicumarol 50-55-5 1841 Reserpine 58-05-9 1136 Leucovorin 66-79-5 -

Draft COMP Agenda 16-18 January 2018
12 January 2018 EMA/COMP/818236/2017 Inspections, Human Medicines Pharmacovigilance and Committees Committee for Orphan Medicinal Products (COMP) Draft agenda for the meeting on 16-18 January 2018 Chair: Bruno Sepodes – Vice-Chair: Lesley Greene 16 January 2018, 09:00-19:30, room 2F 17 January 2018, 08:30-19:30, room 2F 18 January 2018, 08:30-18:30, room 2F Health and safety information In accordance with the Agency’s health and safety policy, delegates are to be briefed on health, safety and emergency information and procedures prior to the start of the meeting. Disclaimers Some of the information contained in this agenda is considered commercially confidential or sensitive and therefore not disclosed. With regard to intended therapeutic indications or procedure scopes listed against products, it must be noted that these may not reflect the full wording proposed by applicants and may also vary during the course of the review. Additional details on some of these procedures will be published in the COMP meeting reports once the procedures are finalised. Of note, this agenda is a working document primarily designed for COMP members and the work the Committee undertakes. Note on access to documents Some documents mentioned in the agenda cannot be released at present following a request for access to documents within the framework of Regulation (EC) No 1049/2001 as they are subject to on- going procedures for which a final decision has not yet been adopted. They will become public when adopted or considered public according to the principles stated in the Agency policy on access to documents (EMA/127362/2006). -

Glutamate and Microglia Activation As a Driver of Dendritic Apoptosis: a Core Pathophysiological Mechanism to Understand Schizop
Parellada and Gassó Translational Psychiatry (2021) 11:271 https://doi.org/10.1038/s41398-021-01385-9 Translational Psychiatry PERSPECTIVE Open Access Glutamate and microglia activation as a driver of dendritic apoptosis: a core pathophysiological mechanism to understand schizophrenia Eduard Parellada 1,2,3 and Patricia Gassó 1,2,4 Abstract Schizophrenia disorder remains an unsolved puzzle. However, the integration of recent findings from genetics, molecular biology, neuroimaging, animal models and translational clinical research offers evidence that the synaptic overpruning hypothesis of schizophrenia needs to be reassessed. During a critical period of neurodevelopment and owing to an imbalance of excitatory glutamatergic pyramidal neurons and inhibitory GABAergic interneurons, a regionally-located glutamate storm might occur, triggering excessive dendritic pruning with the activation of local dendritic apoptosis machinery. The apoptotic loss of dendritic spines would be aggravated by microglia activation through a recently described signaling system from complement abnormalities and proteins of the MHC, thus implicating the immune system in schizophrenia. Overpruning of dendritic spines coupled with aberrant synaptic plasticity, an essential function for learning and memory, would lead to brain misconnections and synaptic inefficiency underlying the primary negative symptoms and cognitive deficits of schizophrenia. This driving hypothesis has relevant therapeutic implications, including the importance of pharmacological interventions during