Brain Tumors Relevant to Clinical Neuro-Ophthalmology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pituitary Adenomas and Ophthalmology
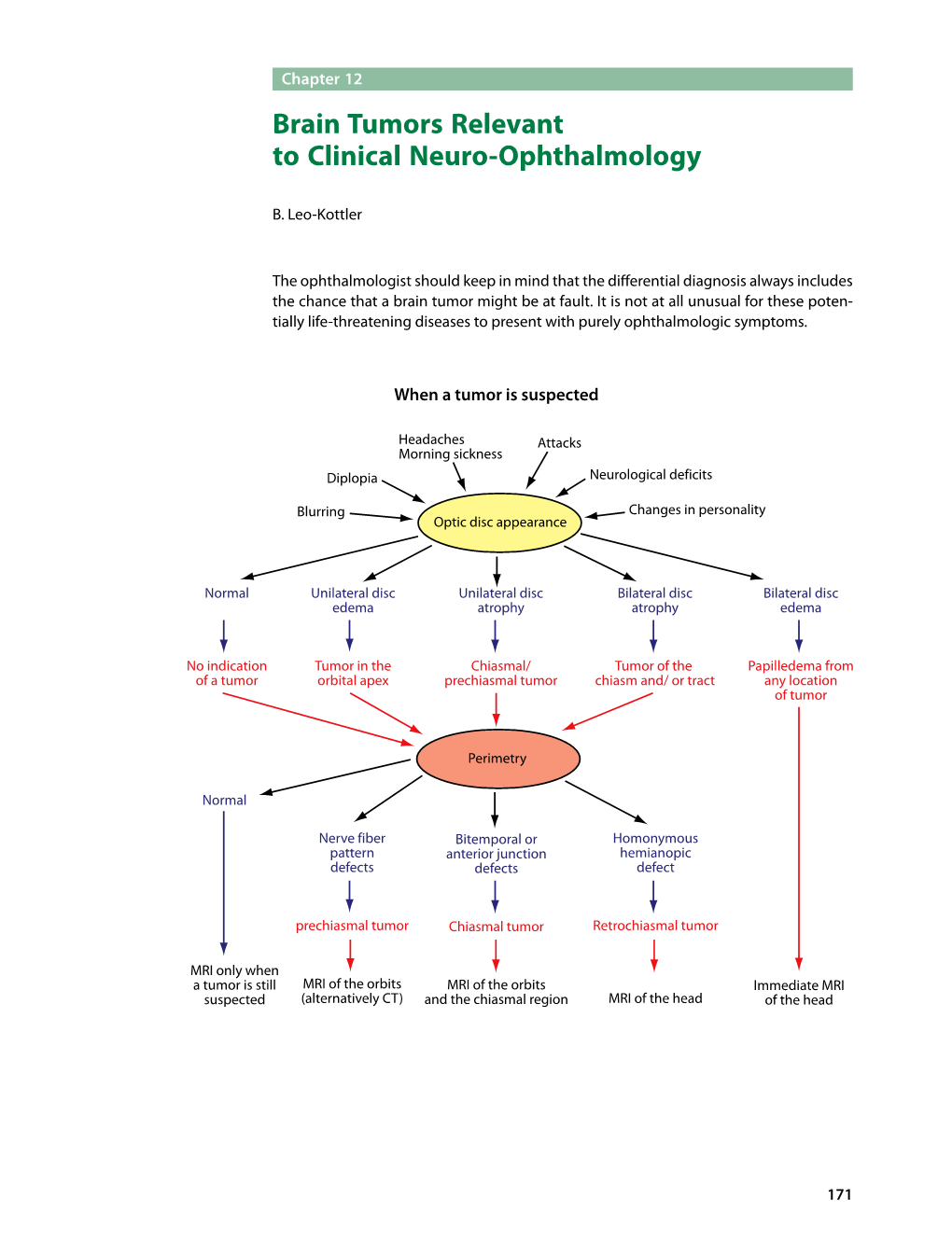
1 Pituitary Adenomas and Ophthalmology Santiago Ortiz-Perez and Bernardo Sanchez-Dalmau Hospital Clinic, University of de Barcelona, Ophthalmology department Spain 1. Introduction Pituitary gland, also called hypophysis, is a neuroendocrine organ placed in the “sella turcica” in the skull base. This gland consists of 2 main areas, the anterior and medial part constitute the adenohypophysis, the posterior part is called neurohypophysis. Pituitary gland is in charge of the internal constancy, homeostasis and reproductive function; this is why pituitary abnormalities cause a wide spectrum of signs and symptoms. Pituitary adenomas are a common pathology; they represent about 10% of all intracranial tumours and between 50-80% of pituitary tumours. Necropsy and imaging studies estimate an incident of 20-25% of pituitary adenomas in general population; however, only about 1/3 of them are clinically evident (Asa & Ezzat, 2009). The majority of these tumours have monoclonal origin (mutation of a single gonadotropic cell), but there are still some discrepancies about the pathogenesis of these neoplasms. The most common mutations seem in other human neoplasms are not frequent in pituitary adenomas, and only a minimum proportion of them are associated to other genetic disorders, such as MEN1 syndrome (multiple endocrine neoplasms type 1) or the Carney complex, due to mutations of the genes MEN1 and PRKAR1A (protein kinase A regulatory subunit 1A) respectively (Beckers & Daly, 2007). Hormones and growth factors involve in normal pituitary function can be also related to the growth of these tumours, although evident connection with the pathogenesis has not been demonstrated. Symptoms related to pituitary tumours are secondary to several factors. -

Traumatic Disruption of the Optic Chiasm
PHOTO ESSAY Traumatic Disruption of the Optic Chiasm Laura Segal, MDCM, Jella Angela An, MDCM, and Mark Gans, MDCM, FRCSC FIG. 1. A. Goldmann visual field examination demonstrates complete bitemporal hemianopia. B. T2 coronal MRI performed on the day of the accident reveals enlargement and distortion of the optic chiasm, with high signal mostly on the left side due to intrinsic hemorrhage (arrow). C. T2 coronal MRI performed 4 weeks after the accident reveals thickening and distortion of the chiasm and complete transection on the left side (arrow). Abstract: A 27-year-old man developed a persistent (J Neuro-Ophthalmol 2009;29:308–310) bitemporal hemianopia after severe head trauma sustained in a high-speed motor vehicle accident. The 27-year-old male pedestrian was hit by a car while he initial brain MRI revealed hemorrhagic contusion of Awas crossing the highway. The initial Glasgow Coma the optic chiasm. A brain MRI performed 4 weeks Scale score was 8 with reactive pupils bilaterally. Non- later demonstrated complete chiasmal transection, contrast brain CT revealed multiple bilateral orbital wall a phenomenon rarely documented with imaging. and facial fractures including the sphenoid walls, but there was no evidence of muscle entrapment or optic nerve sheath pathologic changes. McGill University Health Centre, Montreal, Quebec, Canada. Address correspondence to Laura Segal, MDCM, Montreal General Full ophthalmologic examination performed 5 days Hospital, 1650 Cedar Avenue, Montreal, QC H3G 1A4, Canada. E-mail: after the trauma disclosed a visual acuity of 20/50 in both [email protected] eyes. Pupils measured 4.5 mm in the right eye and 2.5 mm 308 J Neuro-Ophthalmol, Vol. -

Clinical Characteristics and Ophthalmologic Findings of Pituitary
Int Ophthalmol (2019) 39:21–31 https://doi.org/10.1007/s10792-017-0778-x (0123456789().,-volV)(0123456789().,-volV) ORIGINAL PAPER Clinical characteristics and ophthalmologic findings of pituitary adenoma in Korean patients Tae Gi Kim . Kyung Hyun Jin . Jaheon Kang Received: 11 June 2017 / Accepted: 24 November 2017 / Published online: 22 December 2017 Ó Springer Science+Business Media B.V., part of Springer Nature 2017 Abstract visual field defects was found in 36.1% of patients. Purpose To investigate the clinical characteristics of Tumor volume was positively correlated with visual and ophthalmic findings in Korean patients diagnosed field pattern standard deviation (PSD, p = 0.020) and with a pituitary adenoma. best-corrected logMAR visual acuity (p = 0.000) and Methods The medical records of 534 patients diag- negatively associated with tumor volume and visual nosed with a pituitary adenoma at Kyung Hee field mean deviation (MD, p = 0.000). Best-corrected University Hospital between January 2007 and visual acuity (p = 0.000), MD (p = 0.001), and PSD December 2016 were retrospectively reviewed. (p = 0.028) significantly improved after surgery. Results Mean patient age was 47.9 ± 16.2 years. Conclusions Pituitary adenoma patients do not The most common symptoms at the time of presen- always have ocular symptoms at their first presenta- tation were headache (26.2%) and visual disturbance tion, even when optic chiasm compression and visual (12.4%). The referral rate to the ophthalmology field deficits are present. Therefore, collaboration with department was 18.44% and patients most often an ophthalmologist is important when evaluating presented to the neurosurgery department. -

Chiasmal and Retrochiasmal Lesions
CHIASMAL AND RETROCHIASMAL LESIONS Dr. Krati Gupta Dr. Saurabh Deshmukh www.eyelearn.in CHIASMAL AND RETROCHIASMAL LESIONS 1. Causes and ocular manifestations of chiasmal lesions. 3+7 (J2018) 2. Draw a diagram of visual pathway and show visual defects in craniopharyngioma and occipital lobe lesion. J2013 3. Describe anatomy and lesions of optic tracts, chiasma and optic radiations. J2014 4. Define scotoma. How do you differentiate between positive and negative scotoma. Discuss the approach to diagnosis in a patient presenting with left hemianopia. J2012 (optic tract + radiation lesion on right) Chiasmal Lesions i. With the segregation of nasal and temporal retinal fibers at the chiasm, visual field loss due to chiasmal and retrochiasmal lesions is characterized by temporal defects that align along the vertical meridian. ii. In chiasmal syndromes, the optic discs may appear normal initially, even with significant visual field loss. iii. Early on, peripapillary retinal NFL dropout and mild disc pallor develop. iv. With progressive damage, the optic discs show typical atrophy, often in the temporal portion of the disc. v. Cupping of the disc may or may not increase. vi. A tumor compressing the chiasm almost never produces optic disc edema. vii. Parasellar lesions that involve the chiasm—whether compressing or infiltrating this area—produce gradually progressive, bilateral, often asymmetric vision loss. viii. The peripheral (temporal) visual fields usually are involved first. ix. In any case of bilateral visual field loss, the clinician must carefully evaluate perimetry testing results for respect of the vertical midline. x. Any of the variations on bitemporal visual field loss may occur. -

Bitemporal Hemianopia Caused by an Intracranial Vascular Loop
ser photocoagulation to the tumor excision and has been shown to in- cluding tumors and carotid artery surface and surrounding retina was crease patient survival.5 aneurysms1; however, reports of bi- provided. Visual acuity continued to temporal field loss from compres- decrease to 20/70 OD at 17 months, Carol L. Shields, MD sion by an abnormal vessel are rare.2 so PDT was performed (Figure). Miguel A. Materin, MD We describe a patient with a non- The entire astrocytoma was treated Brian P. Marr, MD progressive bitemporal hemiano- with a single 83-second laser spot at Jaime Krepostman, MD pia in whom there appeared to be 689 nm (50 J/cm2) following intra- Jerry A. Shields, MD compression of the optic chiasm by 2 venous verteporfin (6 mg/m ). Af- Correspondence: Dr C. L. Shields, an elongated right anterior cerebral ter treatment, resolution of macu- Ocular Oncology Service, Wills Eye artery (ACA). lar exudation, edema, and subretinal Institute, Ste 1440, 840 Walnut St, fluid led to improved vision of 20/50 Philadelphia, PA 19107 (carol Report of a Case. A bitemporal OD (at 1 month) and 20/30 OD (at [email protected]). hemianopia was found in a 65-year- 4, 8, and 12 months). The tumor Author Contributions: Dr C. L. old woman with no vascular risk fac- showed minimal involution with de- Shields had full access to all the data tors during a routine eye examina- creased intrinsic vascularity. in the study and takes responsibil- tion in 2003. Magnetic resonance ity for the integrity of the data and imaging (MRI) results were nor- Comment. -

DEPARTMENT of OPHTHALMOLOGY FACULTY of MEDICINE UNIVERSITAS PADJAJARAN NATIONAL EYE CENTER CICENDO EYE HOSPITAL BANDUNG Case
0 DEPARTMENT OF OPHTHALMOLOGY FACULTY OF MEDICINE UNIVERSITAS PADJAJARAN NATIONAL EYE CENTER CICENDO EYE HOSPITAL BANDUNG Case Report : Chiasmal Syndrome with Mass in Sella Turcica Presenter : Magdalena Purnama Soeprajogo Supervisor : Antonia Kartika, MD Has been reviewed and approved by Supervisor of Neuro-Ophthalmology Unit Antonia Kartika, MD Monday, September 21th 2020 08.15 AM 1 Chiasmal Syndrome with Mass in Sella Turcica Abstract Introduction Undiagnosed chiasmal syndrome come to neurosurgeons only after being misdiagnosed leads to decreased visual acuity, progression of the pathological process, and irreversible loss of sight. Purpose to describe the clinical characteristics of patients with the chiasmal syndrome . Case Report a 26 years old male with a chief complaint of blurred vision on the right eye since 2 months. Visual acuity on the right eye was 0.63 and on the left eye was 1.0. The visual field testing showed bitemporal hemianopia. OCT RNFL showed marked thinning on right eye. The brain CT scan showed homogenous enhancing mass at sellar tursica. Neurosurgeon referral was advised to patient. Result The brain CT scan showed homogenous enhancing mass at sellar tursica. Neurosurgeon referral was advised to patient. Conclusion Bitemporal hemianopia are common visual field defect in chiasmal syndrome. Neuroimaging examination is mandatory to confirm the topical diagnosis. Chiasmal syndrome early detection of by ophthalmologists and timely referral to relevant specialists will facilitate improved visual function outcomes and quality of life for patients Keywords Chiasmal syndrome, bitemporal hemianopia, sellar tursica. I. Introduction Chiasmal syndrome is the name given to the group of symptoms and signs that occur together as a result of lesions affecting the optic chiasm. -

Print This Article
University Journal of Surgery and Surgical Specialities ISSN 2455-2860 2020, Vol. 6(2) 2 CASE REPORTS OF OPTIC CHIASMAL SYNDROME BAVYA M Department of Ophthalmology, MADRAS MEDICAL COLLEGE AND GOVERNMENT GENERAL HOSPITAL Abstract : The optic chiasm is one of the most important Anterior segment examination of the right eye was normal. Right structures in neuro ophthalmologic diagnosis. The eye showed sluggish pupillary reaction to light. Fundus of right arrangement of visual fibres in the chiasm accounts for eye showed disc edema with peripapillary hemaorrhages[FIG 1]. characteristic defects in the visual fields caused by such Left eye vision was 3/60 which improved to 6/36 with correction. diverse processes as compression , inflammation , Left eye showed sluggish pupillary reaction to light. Otherwise demyelination, ischemia and infiltration. Two cases are anterior segment was normal. Fundus showed disc edema with a presented here. The first case presented with right temporal haemorrhage in the superotemporal quadrant[FIG 2]. Both eyes field defect with central scotoma of the left eye and bilateral showed lens changes. papilledema. MRI SCAN showed it as suprasellar astrocytoma. The second case presented with temporal field defect and left eye optic atrophy. MRI SCAN showed it as pituitary macro adenoma or dorsal sella meningioma. Thus showing the importance of ocular examination in identifying intracranial tumours. Keyword :Optic chiasm, temporal field defect, papilledema, optic atrophy INTRODUCTION The optic chiasm is one of the most important structure in FIG 1: Right Eye papilledema neuro-ophthalmologic diagnosis. Damage to the optic chiasm can occur from direct or indirect effects of a variety of lesions. -

Isolated Lymphoma of the Optic Nerve, Chiasm and Tract: a Case Report
ONCOLOGY LETTERS 10: 3013-3017, 2015 Isolated lymphoma of the optic nerve, chiasm and tract: A case report YUE‑LI ZHU1,2, XIU‑FENG SONG3 and BIN WANG1,4 1Shandong Medical Imaging Research Institution, Shandong University, Jinan, Shandong 250021; 2Department of Radiology, Qingdao Municipal Hospital, Qingdao, Shandong 266071; 3Department of Radiology, Qingdao University Affiliated Hospital, Qingdao, Shandong 266003; 4Medical Imaging Research Institute, Binzhou Medical University, Yantai, Shandong 264003, P.R. China Received October 16, 2014; Accepted July 17, 2015 DOI: 10.3892/ol.2015.3675 Abstract. The current study reports the case of a 68-year-old, in the immunocompetent population has been reported to have previously healthy female who presented with progressive increased >10-fold from 2.5 cases to 30 cases per 10 million visual impairment leading to blindness bilaterally. Brain population between 1973 and 1992 (2,3). The cause for the imaging features were suggestive of malignant glioma of the increase in incidence of this disease in the immunocompetent anterior visual pathway. Postoperative examination indicated population is unknown. Surgical resection is generally ineffec- a diagnosis of diffuse malignant lymphoma type B. As no tive due to the depth of the tumor. Furthermore, treatment with evidence of extracranial lymphoma was observed, the final radiotherapy and corticosteroids often only produce a partial diagnosis was primary central nervous system lymphoma response, and tumors recur in >90% of patients (4). Median (PCNSL). Following treatment with surgery and radiotherapy, survival is 10-18 months in immunocompetent patients, and the patient's symptoms went into remission. At a follow-up less in those with AIDS (5). -

An Unusual Chiasmal Visual Defect in a Patient with Neuromyelitis Optica: Case Report
RELATOS DE CASOS An unusual chiasmal visual defect in a patient with neuromyelitis optica: case report Comprometimento quiasmático incomum em um paciente com neuromielite óptica: relato de caso Roberta Martins da Silva Costa1 ABSTRACT Antonio Carlos Santos2 Laudo Silva Costa3 Purpose: To report the unusual visual field finding due to a chiasmal neuritis in a 33-year-old female with the diagnosis of optic neuromyelitis optica (Devic’s syndrome). Methods: We report a case of a 33 years old female with limb paraesthesias, weakness in the legs, bowel and bladder dysfunction that was referred to the “Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo” in October 1995. Six years and four months later she had an acute visual involvement. Ophthalmologic examination, laboratory studies, magnetic resonance imaging (MRI) and a 24-2 threshold visual field in the Humphrey field analyzer were performed. Results: The MRI scan showed enlargement and cavitation on the spinal cord and chiasmal involvement (thickening of the chiasm with contrast enhancement) and no demyelinating lesions in the brain, brainstem, or cerebellum. The central 24-degree threshold field examination showed an inferior visual field defect bitemporally, disclosing a chiasmal involvement. Conclusion: Chiasmal involvement may occur in neuromyelitis optica, probably due to a plaque within the chiasm. The authors call attention to the importance of visual field examination with particular regard to quantifying the visual impairment and follow-up of these patients. Keywords: Hemianopsia; Neuromyelitis optica/diagnosis; Optic chiasm; Scotoma; Perimetry; Optic neuritis INTRODUCTION Trabalho realizado no Hospital das Clínicas da Faculda- de de Medicina da Universidade de São Paulo - USP - The diagnosis of chiasmal syndrome can be divided into compressive and Ribeirão Preto (SP) - Brasil. -

Haemorrhage from a Cavernous Malformation in the Optic Chiasm
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.52.9.1095 on 1 September 1989. Downloaded from Journal ofNeurology, Neurosurgery, and Psychiatry 1989;52:1095-1099 Short report Chiasmal apoplexy: haemorrhage from a cavernous malformation in the optic chiasm LUCA REGLI,* NICOLAS DE TRIBOLET,* FRANCO REGLI,** JULIEN BOGOUSSLAVSKY** From the Departments ofNeurosurgery* and Neurology**, University Hospital, Lausanne, Switzerland SUMMARY We present a patient who experienced sudden onset of orbital headache, visual loss and bitemporal visual field defect. MRI of the optic chiasm suggested a diagnosis of haemorrhage and hence a vascular malformation. Pterional craniotomy revealed an intrachiasmatic haematoma with a cavernous angioma. The malformation was totally excised and vision improved after surgery. The syndrome of chiasmal apoplexy is discussed. Protected by copyright. Visual field defects due to chiasmal compression from no pupillary defect. Computerised tomography showed a a tumour usually progress slowly. An acute syndrome high-density, poorly enhanced mass in the anterior part of may be due to ischaemic, haemorrhagic or demyelin- the right optochiasmal cistern (fig 2). The carotid angiogra- iating disease. phy was normal. MRI, performed three days after onset, "Chiasmal showed enlargement of the chiasm on the right side by an apoplexy" is essentially associated with intrachiasmal lesion with a mixed hypo- and a slight hyperin- haemorrhage in the chiasm itself and is typically of tense signal, when compared with grey matter, on mildly Tl- sudden onset. We report a case of spontaneous and proton-weighted images (figs 3 and 4). haematoma in the optic chiasm from a cavernous malformation which could be suspected on magnetic Operation resonance imaging (MRI). -

Isolated Bitemporal Hemianopsia Due to Traumatic Chiasmal Syndrome
CASE REPORT Isolated bitemporal hemianopsia due to traumatic chiasmal syndrome Bulent Yazici, M.D., Sertac Argun Kivanc, M.D. Department of Ophthalmology, Uludağ University Faculty of Medicine, Bursa, Turkey ABSTRACT A 20-year-old man presented with complaints of inability to see the outer half of objects and blurred near vision while reading. His complaints began one year ago after a motor vehicle accident that caused cranio-orbital fractures. Ocular examination revealed com- plete bitemporal hemianopsia and slight exotropia. Central visual acuity was 20/20 in both eyes. Radiologic studies demonstrated frac- tures in the fronto-ethmoid and sphenoid bones and thinning of the optic chiasm. No hypothalamic-pituitary abnormality was detected. Clinical findings remained unchanged during follow-up. Although rare, blunt head trauma may cause an isolated damage to the chiasmal crossing nerve fibers, resulting in a complete, bitemporal hemianopsia associated with normal visual acuity. Traumatic chismal syndrome should be considered in the differential diagnosis of patients presenting with bitemporal hemianopsia. Keywords: Bitemporal hemianopsia; head trauma; optic chiasmal injury; traumatic chiasmal syndrome. INTRODUCTION Bitemporal hemianopsia is a sign that typically indicates an mission to an emergency clinic, he was conscious and com- optic chiasmal involvement, mostly caused by a compressive plained of blurred vision, and bilateral periorbital ecchymosis tumor.[1] Traumatic chiasmal injury, also called traumatic chi- was noted. Computed tomography showed frontal, ethmoid, asmal syndrome (TCS), is a rare phenomenon and can mani- and maxillary fractures in the right orbit, fractures in the sel- fest with a variety of visual defects.[2] Herein, it was aimed to lar region of the sphenoid bone, and air in the orbit and cra- report a case of TCS with an isolated, complete bitemporal nium (Fig. -

Chiasmal Syndrome Chiasmal Syndrome
10/3/2016 Chiasmal Syndrome • Online notes – richardtrevino.net • Email me Everything You Always Wanted – [email protected] to Know About PITUITARY ADENOMA • Disclosures But Were Afraid to Ask! – None Rick Trevino, OD, FAAO Rosenberg School of Optometry Chiasmal Syndrome Chiasmal Syndrome • Chiasmal syndrome is the constellation of • Causes of chiasmal syndrome include tumor, signs and symptoms associated with lesions inflammation, and ischemia of the optic chiasm • Findings suggestive of an etiology other than – Pituitary adenoma is the most common cause pituitary adenoma: – Visual sxs (blur or difficulties with side vision) • 25% of all brain tumors occur in this region – Younger age – 50% are pituitary ademomas – Unilateral optic disk pallor – Visual disturbance is common – RAPD • Patients with chiasmal lesions may present – A complete hemianopic VF defect c/o headache and/or visual disturbances – VF defect greater inferiorly than superiorly AJO 2004;137:908-913 Incomplete bitemporal Chiasmal Syndrome hemianopic defect greater above than below – highly • Anatomy Review suggestive of pituitary anenoma • All About Pituitary Pituitary Adenomas • Incomplete Clinical Features of bitemporal Chiasmal Syndrome hemianopia greater below • Clinical Pearls than above – highly suggestive of – Red Flag Warning Signs something other – Chiasmal Work-up than pituitary Something Else adenoma 1 10/3/2016 The pituitary gland is located 10mm immediately below the optic chiasm T1-weighted T2-weighted coronal MRI sagital MRI Pituitary Adenoma Pituitary