Yates High School Registration 2020-2021
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Office of Neighborhood & Strategic Initiatives
Office of Neighborhood & Strategic Initiatives Campus Newsletter March 2017 Education The University of Houston (UH) College of Education (COE) has been partnering with Houston Independent School District (HISD) since 2015-16 to work in six high-need schools in Third Ward. Blackshear, Hartsfield, Thompson and Foster elementary schools; Cullen Middle School; and Yates High School. The goal is to raise academic achievement and student success while creating a sustainable model that can be replicated nationwide. UH students in teacher preparation, counseling and social work degree programs are assisting the schools' teachers and professional staff and learning from them. Recent New Initiatives My Home Library – This new program allows students at Blackshear elementary and the Cuney Homes public housing project to create a wish list of books for donors who can then provide a child six books for $30. After School Program – COE has partnered with the Cuney Homes and the YMCA to deliver after school and summer programs to children where they live. The 30 participants in the after school program were also provided bicycles from a generous supporter of the program. CHAMP – This mathematics and stem outreach program connects Cullen Middle School students with Natural Science and Mathematics' graduate and undergraduate tutors. Page 1 of 6 College Readiness – UH Honors College students teach SAT preparation and provide mentoring to better prepare Yates High School students for college. Jack Yates High School Mentorship Program by ENACTUS (Entrepreneurial, Action, Us) ENACTUS is a global student organization with chapters at universities in over 35 countries around the world. Under the leadership of professor Jamie Belinne, the BAUER Enactus students established this program in the fall of 2016 as a group project under the BAUER Connecting Bauer to Business Class, GENB 3302. -
Web Stats Report: November
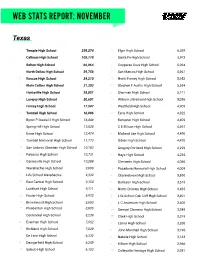
WEB STATS REPORT: NOVEMBER Texas 1 Temple High School 259,274 31 Elgin High School 6,029 2 Calhoun High School 108,778 32 Santa Fe High School 5,973 3 Belton High School 66,064 33 Copperas Cove High School 5,964 4 North Dallas High School 59,756 34 San Marcos High School 5,961 5 Roscoe High School 34,210 35 North Forney High School 5,952 6 Klein Collins High School 31,303 36 Stephen F Austin High School 5,554 7 Huntsville High School 28,851 37 Sherman High School 5,211 8 Lovejoy High School 20,601 38 William J Brennan High School 5,036 9 Forney High School 17,597 39 Westfield High School 4,909 10 Tomball High School 16,986 40 Early High School 4,822 11 Byron P Steele I I High School 16,448 41 Kempner High School 4,809 12 Spring Hill High School 13,028 42 C E Ellison High School 4,697 13 Ennis High School 12,474 43 Midland Lee High School 4,490 14 Tomball Memorial High School 11,773 44 Odem High School 4,470 15 San Antonio Christian High School 10,783 45 Gregory-Portland High School 4,299 16 Palacios High School 10,731 46 Hays High School 4,235 17 Gainesville High School 10,288 47 Clements High School 4,066 18 Waxahachie High School 9,609 48 Pasadena Memorial High School 4,009 19 Life School Waxahachie 9,332 49 Channelview High School 3,890 20 East Central High School 9,150 50 Burleson High School 3,615 21 Lockhart High School 9,111 51 North Crowley High School 3,485 22 Foster High School 8,972 52 Life School Oak Cliff High School 3,401 23 Brownwood High School 8,803 53 L C Anderson High School 3,400 24 Pleasanton High School 8,605 54 Samuel -
Web Stats Report: March
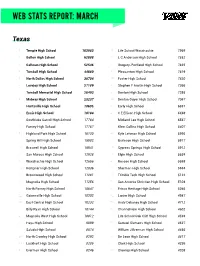
WEB STATS REPORT: MARCH Texas 1 Temple High School 163983 31 Life School Waxahachie 7969 2 Belton High School 62888 32 L C Anderson High School 7852 3 Calhoun High School 52546 33 Gregory-Portland High School 7835 4 Tomball High School 44880 34 Pleasanton High School 7619 5 North Dallas High School 38704 35 Foster High School 7420 6 Lovejoy High School 27189 36 Stephen F Austin High School 7366 7 Tomball Memorial High School 26493 37 Denton High School 7295 8 Midway High School 23237 38 Denton Guyer High School 7067 9 Huntsville High School 18605 39 Early High School 6881 10 Ennis High School 18184 40 C E Ellison High School 6698 11 Southlake Carroll High School 17784 41 Midland Lee High School 6567 12 Forney High School 17767 42 Klein Collins High School 6407 13 Highland Park High School 16130 43 Kyle Lehman High School 5995 14 Spring Hill High School 15982 44 Burleson High School 5917 15 Braswell High School 15941 45 Cypress Springs High School 5912 16 San Marcos High School 12928 46 Elgin High School 5634 17 Waxahachie High School 12656 47 Roscoe High School 5598 18 Kempner High School 12036 48 Sherman High School 5564 19 Brownwood High School 11281 49 Trimble Tech High School 5122 20 Magnolia High School 11256 50 San Antonio Christian High School 5104 21 North Forney High School 10647 51 Frisco Heritage High School 5046 22 Gainesville High School 10302 52 Lanier High School 4987 23 East Central High School 10232 53 Andy Dekaney High School 4712 24 Billy Ryan High School 10144 54 Channelview High School 4602 25 Magnolia West High School -

2005 Area Non Participating Chapters
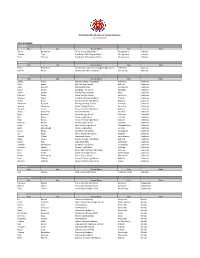
2005 TEXAS FFA LEADERSHIP DEVELOPMENT EVENTS NON-PARTICIPATING SCHOOLS Area I (School districts in the following counties: Armstrong, Bailey, Briscoe, Carson, Castro, Childress, Cochran, Collingsworth, Cottle, Crosby, Dallam, Deaf Smith, Dickens, Donley, Floyd, Gray, Hale, Hall, Hansford, Hartley, Hemphill, Hockley, Hutchinson, King, Lamb, Lipscomb, Lubbock, Moore, Motley, Ochiltree, Oldham, Parmer, Potter, Randall, Roberts, Sherman, Swisher, Wheeler.) School District Chapter Amarillo Caprock High School Boys Ranch Boys Ranch High School Canyon Canyon High School Canyon Randall High School Hart Hart High School Higgins Higgins High School Highland Park Highland Park High School Littlefield Littlefield High School Miami Miami High School Motley County Motley County High School River Road River Road High School Shamrock Shamrock High School Smyer Smyer High School Spade Spade High School LEADERSHIP DEVELOPMENT EVENTS—NON-PARTICIPATING SCHOOLS Area II Schools in the following counties: Andrews, Borden, Brewster, Coke, Crane, Crockett, Culberson, Dawson, Ector, El Paso, Fisher, Gaines, Garza, Glasscock, Haskell, Howard, Hudspeth, Irion, Jeff Davis, Jones, Kent, Loving, Lynn, Martin, Midland, Mitchell, Nolan, Pecos, Presidio, Reagan, Reeves, Schleicher, Scurry, Sterling, Stonewall, Sutton, Terrell, Terry, Tom Green, Upton, Ward, Winkler, and Yoakum. School District Chapter Big Spring Big Spring High School Bronte Bronte High School Christoval Chistoval High School Dell City Dell City High School Greenwood Greenwood High School Highland Highland -

DHS SLA Annual Report 2016
Texas Southern University Department of Homeland Security Scientific Leadership Award Program DHS-15-ST-062-001 Preparing Technically Savvy Homeland Security Professionals for Maritime Transportation Security AWARD NUMBER: 2014-ST-062-000057-02 Annual Report 2016 Department of Transportation Studies DHS SLA Annual Report 2016 TABLE OF CONTENTS 1 EXECUTIVE SUMMARY ....................................................................................................................... 4 2 COURSE DEVELOPMENT ..................................................................................................................... 5 2.1 New Course 1: Software for Scientific Computing ............................................................................ 5 2.2 New Course 2: Introduction to Operations Research .......................................................................... 9 2.3 New Course 3: Maritime Risk Assessment and Resiliency Analysis ............................................... 11 2.4 Improved Course 1: MTMS 341-Maritime Security Management ................................................... 12 2.5 Development of USCG Maritime Certificate Courses ...................................................................... 12 2.6 Development of Seminars and Workshops ....................................................................................... 13 3 COLLABORATIONS WITH DHS CENTER OF EXCELLENCE (COE) ............................................ 14 4 RESEARCH ............................................................................................................................................ -

Yates High School Faqs
Yates High School FAQs General Is Jack Yates High School staying open? Yes. HISD is committed to Yates High School, and we’re investing in the school’s future. As part of the 2012 Bond Program, HISD is building a new state-of-the-art campus with 21st century learning spaces that will serve Yates students for generations to come. Planning and design for the new school is currently underway. Yates also was included in the 2007 Bond Program and received various upgrades, repairs and renovations designed to sustain the school and maintain a safe and suitable learning environment until a new campus could be built. Our goal is to strengthen Jack Yates High School so it can continue to build its enrollment and serve as a school of choice for students in the Third Ward and beyond. The district is also working with the school leadership and the community to improve the academic program at Yates so all students who attend will be prepared for college and careers. Are you keeping the name of the school? Yes. The name of Jack Yates High School reflects its storied history, and HISD values that history. Why is the school being built for 1,300 to 1,500 students? Jack Yates’ current enrollment is just over 1,000 students. The new school will allow for projected growth in the Third Ward area. HISD demographers considered birth data, historical school enrollment data, and micro- and macro-economic projection data to determine the range of capacities included for all schools in the 2012 bond referendum. -

The History of the National Basketball Tournaments for Black High Schools
Louisiana State University LSU Digital Commons LSU Historical Dissertations and Theses Graduate School 1980 The iH story of the National Basketball Tournaments for Black High Schools. Charles Herbert Thompson Louisiana State University and Agricultural & Mechanical College Follow this and additional works at: https://digitalcommons.lsu.edu/gradschool_disstheses Recommended Citation Thompson, Charles Herbert, "The iH story of the National Basketball Tournaments for Black High Schools." (1980). LSU Historical Dissertations and Theses. 3500. https://digitalcommons.lsu.edu/gradschool_disstheses/3500 This Dissertation is brought to you for free and open access by the Graduate School at LSU Digital Commons. It has been accepted for inclusion in LSU Historical Dissertations and Theses by an authorized administrator of LSU Digital Commons. For more information, please contact [email protected]. INFORMATION TO USERS This was produced from a copy of a document sent to us for microfilming. While the most advanced technological means to photograph and reproduce this document have been used, die quality is heavily dependent upon die quality of the material submitted. The following explanation of techniques is provided to help you understand markings or notations which may appear on this reproduction. 1.The sign or “target” for pages apparently lacking from the document photographed is “Missing Page(s)”. If it was possible to obtain die missing page(s) or section, they are spliced into the film along with adjacent pages. This may have necessitated cutting through an image and duplicating adjacent pages to assure you of complete continuity. 2. When an image on the film is obliterated with a round black mark it is an indication that die film inspector noticed either blurred copy because of movement during exposure, or duplicate copy. -

Key Issue: Enhancing Teacher Leadership
Key Issue: Enhancing Teacher Leadership All resources contained within the TQ Tips & Tools documents have been reviewed for their quality, relevance, and utility by TQ Center staff and three content-area experts. These experts usually have a policy, practice or research background. The strategies and resources are provided to help regional comprehensive center and state education agency staff to be aware of the initiatives, programs or activities taking place in other settings. Our provision of the links to these resources should not be considered an endorsement but a qualified suggestion that they be considered as an option to study and/or pursue given the needs and context of the inquiring region, state, or district. Evidence of the impact of initiatives, programs or activities is provided where available or appropriate. October 2007 1100 17th Street N.W., Suite 500 Washington, DC 20036-4632 877-322-8700 y 202-223-6690 www.ncctq.org Copyright © 2007 National Comprehensive Center for Teacher Quality, sponsored under government cooperative agreement number S283B050051. All rights reserved. This work was originally produced in whole or in part by the National Comprehensive Center for Teacher Quality with funds from the U.S. Department of Education under cooperative agreement number S283B050051. The content does not necessarily reflect the position or policy of the Department of Education, nor does mention or visual representation of trade names, commercial products, or organizations imply endorsement by the federal government. The National Comprehensive Center for Teacher Quality is a collaborative effort of Education Commission of the States, ETS, Learning Point Associates, and Vanderbilt University. -

Lone Star College System Spring 2014 High School Graduates From
Lone Star College System Spring 2014 High School Graduates from Service Area ISDs and High Schools Enrolled at LSCS Official Day Fall 2014 ISD High School Total Aldine Aldine High School 116 18.0% Carver High School 55 8.5% Eisenhower High School 150 23.3% Hall Center for Education 13 2.0% MacArthur High School 145 22.5% Nimitz High School 152 23.6% Victory Early College High School 14 2.2% Aldine Total 645 100.0% Cleveland Cleveland High School 33 100.0% Cleveland Total 33 100.0% Conroe Caney Creek High School 108 14.0% Conroe High School 163 21.2% Hauke Academic Alternative High School 11 1.4% Oak Ridge High School 205 26.7% The Woodlands College Park High School 130 16.9% The Woodlands High School 152 19.8% Conroe Total 769 100.0% Cy-Fair Cy-Fair High School 175 9.3% Cypress Creek High School 225 11.9% Cypress Falls High School 205 10.9% Cypress Lakes High School 195 10.3% Cypress Ranch High School 135 7.2% Cypress Ridge High School 202 10.7% Cypress Springs High School 130 6.9% Cypress Woods High School 175 9.3% Jersey Village High School 242 12.8% Langham Creek High School 178 9.4% Windfern High School 26 1.4% Cy-Fair Total 1,888 100.0% Humble Atascocita High School 197 30.3% Humble High School 69 10.6% Kingwood High School 122 18.8% Kingwood Park High School 119 18.3% Quest High School 45 6.9% Summer Creek High School 98 15.1% Humble Total 650 100.0% Huntsville Huntsville High School 41 100.0% Huntsville Total 41 100.0% Katy* Cinco Ranch High School 57 10.4% James E Taylor High School 65 11.9% Katy High School 74 13.5% Martha Raines -

FINAL RANK TEAM NAME CITY SCORE 1 Alamo Heights High
Texas State Spirit Championships January 1, 2016 FINALISTS- 5A FINAL RANK TEAM NAME CITY SCORE 1 Alamo Heights High School San Antonio 223.267 2 Prosper High School Prosper 214.566 3 Woodrow Wilson High School Dallas 212.000 4 Lumberton High School Lumberton 210.434 5 New Caney High School New Caney 210.000 6 Brenham High School Brenham 209.000 7 Willis High School Willis 207.100 8 The Colony High School The Colony 205.933 9 Dayton High School Dayton 205.733 10 Vandegrift High School Austin 205.700 11 Denison High School Denison 204.700 12 Temple High School Temple 204.599 13 Cedar Park High School Cedar Park 204.433 14 Magnolia High School Magnolia 203.567 15 North Forney High School Forney 200.833 16 Seguin High School Seguin 200.767 17 Frisco High School Frisco 200.433 18 Magnolia West High School Magnolia 200.400 19 Birdville High School North Richland Hills 200.166 20 Donna High School Donna 199.967 21 Livingston ISD Livingston 199.834 22 George Ranch High School Richmond 199.666 23 Marble Falls High School Marble Falls 199.300 24 McKinney North High School McKinney 196.199 25 Newman Smith High School Carrollton 194.900 26 Huntsville High School Huntsville 192.266 27 Royse City High School Royse City 191.667 28 Grapevine High School Grapevine 191.500 29 Del Valle High School El Paso 190.933 30 Lovejoy High School Allen 190.867 31 Ridge Point High School Missouri City 190.801 32 McKinney High School McKinney 190.500 33 Tyler High School Tyler 190.133 34 Little Elm High School Little Elm 189.067 Texas State Spirit Championships January -

SCHOOL RATINGS Distinctions & Designations
Ratings by ISD Greater Houston Area Student Progress Student Achievements SCHOOL RATINGS Distinctions & Designations 2019 oldrepublictitle.com/Houston 09/2019 | © Old Republic Title | This material is for educational purposes only and does not constitute legal advice. We assume no liability for errors or omissions. Old Republic Title’s underwriters are Old Republic National Title Insurance Company and American Guaranty Title Insurance Company. | SW-HOU-PublicSchoolRatings-2019 | SWTD_SS_0094 TEXAS EDUCATION AGENCY ACCOUNTABILITY RATING SYSTEM DISTRICTS AND CAMPUSES RECEIVE AN OVERALL RATING, AS WELL AS A RATING FOR EACH DOMAIN. • A, B, C, or D: Assigned for overall performance and for performance in each domain to districts and campuses (including those evaluated under alternative education accountability [AEA]) that meet the performance target for the letter grade • F: Assigned for overall performance and for performance in each domain to districts and campuses (including AEAs) that do not meet the performance target to earn at least a D. • Not Rated: Assigned to districts that—under certain, specific circumstances—do not receive a rating. NOTE: Single-campus districts must meet the performance targets required for the campus in order to demonstrate acceptable performance. The Texas Education Agency looks at three domains in determining a school’s accountability rating: Evaluates performance across all subjects for all Student students, on both general and alternate assessments, Achievement College, Career, and Military Readiness (CCMR) indicators, and graduation rates. Measures district and campus outcomes in two areas: the School number of students that grew at least one year academically (or are on track) as measured by STAAR results and the achievement Progress of all students relative to districts or campuses with similar economically disadvantaged percentages. -
2018-Mcdaag-Nominees-List.Pdf
2018 McDonald's All American Games Nominees As of 1/10/2018 BOYS NOMINEES ALABAMA First Last School Name City State Alston Humphrey Park Crossing High School Montgomery Alabama Akwuba Theo Brewbaker Tech Magnet School Montgomery Alabama Kevin Winslow Brewbaker Tech Magnet School Montgomery Alabama ARKANSAS First Last School Name City State Ethan Henderson Parkview Arts and Science Magnet High School Little Rock Arkansas Kamren Roelke Christian Ministries Academy Hot Springs Arkansas CALIFORNIA First Last School Name City State James Akinjo Salesian College Preparatory Richmond California Riley Battin Oak Park High School Oak Park California Jules Bernard Windward School Los Angeles California Darius Brown Pasadena High School Pasadena California Jordan Brown Prolific Prep Academy Napa California Harrison Butler Mater Dei High School Santa Ana California Taeshon Cherry Foothills Christian Academy El Cajon California Shane Dolan Bishop O'Dowd High School Oakland California Devonaire Doutrive Birmingham High School Van Nuys California Spencer Freedman Mater Dei High School Santa Ana California Naseem Gaskin Bishop O'Dowd High School Oakland California Adam Grabowski Vacaville Christian Vacaville California Bryce Hamilton Pasadena High School Pasadena California Eric Hancik Damien High School La Verne California Elijah Hardy Bishop O'Dowd High School Oakland California Mobeen Hirbod Bentley Upper School Lafayette California Logan Johnson Saint Francis High School Mountain View California Elijah McCullough Damien High School La Verne California David Mixon Cathedral High School Los Angeles California Jay Nagle Will C. Wood High School Vacaville California Shareef O'Neal Crossroads School Santa Monica California Miles Owens Bishop O'Dowd High School Oakland California Darryl Polk Long Beach Poly Long Beach California Orlando Robinson Jr.