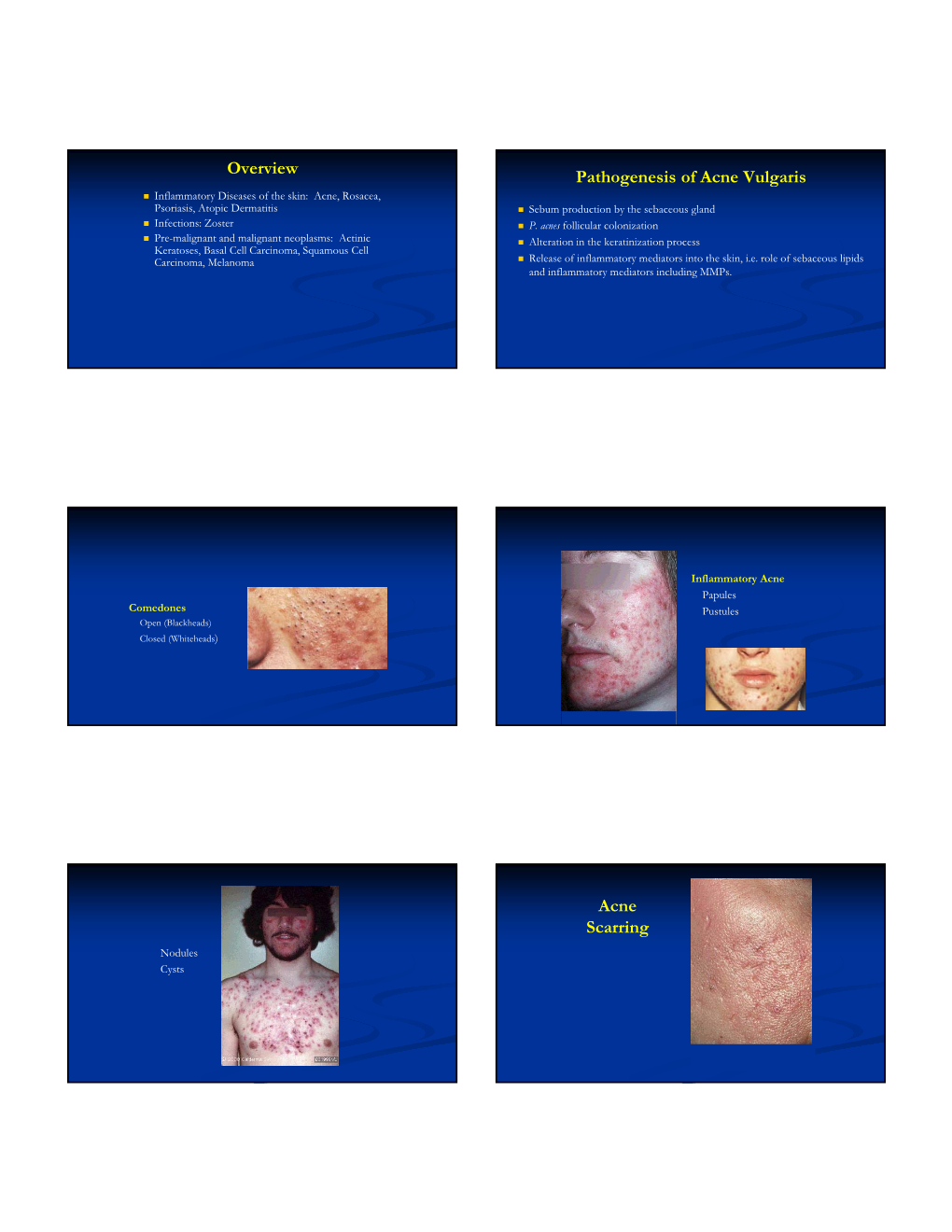
Overview Pathogenesis of Acne Vulgaris Acne Scarring
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Risk of Cancer in Patients with Psoriasis a Population-Based Cohort Study in the Health Improvement Network
Research Original Investigation The Risk of Cancer in Patients With Psoriasis A Population-Based Cohort Study in the Health Improvement Network Zelma C. Chiesa Fuxench, MD; Daniel B. Shin, MS; Alexis Ogdie Beatty, MD, MSCE; Joel M. Gelfand, MD, MSCE IMPORTANCE The risk of cancer in patients with psoriasis remains a cause of special concern due to the chronic inflammatory nature of the disease, the use of immune-suppressive treatments and UV therapies, and the increased prevalence of comorbid, well-established risk factors for cancer, such as smoking and obesity, all of which may increase the risk of carcinogenesis. OBJECTIVE To compare the overall risk of cancer, and specific cancers of interest, in patients with psoriasis compared with patients without psoriasis. DESIGN, SETTING, AND PARTICIPANTS Population-based cohort study of patients ages 18 to 89 years with no medical history of human immunodeficiency virus, cancer, organ transplants, or hereditary disease (albinism and xeroderma pigmentosum), prior to the start date, conducted using The Health Improvement Network, a primary care medical records database in the United Kingdom. The data analyzed had been collected prospectively from 2002 through January 2014. The analysis was completed in August 2015. EXPOSURES OF INTEREST Patients with at least 1 diagnostic code for psoriasis were classified as having moderate-to-severe disease if they had been prescribed psoralen, methotrexate, cyclosporine, acitretin, adalimumab, etanercept, infliximab, or ustekinumab or phototherapy for psoriasis. Patients were classified as having mild disease if they never received treatment with any of these agents. MAIN OUTCOMES AND MEASURES Incident cancer diagnosis. RESULTS A total of 937 716 control group patients without psoriasis, matched on date and practice visit, and 198 366 patients with psoriasis (186 076 with mild psoriasis and 12 290 with moderate-to-severe disease) were included in the analysis. -

Jebmh.Com Original Research Article
Jebmh.com Original Research Article OCULAR INVOLVEMENT IN MUCOCUTANEOUS DISORDERS- A STUDY IN TERTIARY HOSPITAL IN SOUTH ORISSA Sarita Panda1, B. N. R. Subudhi2, Prangya Panda3, Santosh Kumar Padhi4 1Assistant Professor, Department of Ophthalmology, M.K.C.G. Medical College, Berhampur, Orissa. 2Professor and HOD, Department of Ophthalmology, M.K.C.G. Medical College, Berhampur, Orissa. 3Associate Professor, Department of Ophthalmology, M.K.C.G. Medical College, Berhampur, Orissa. 4Senior Medical Officer, Government City Hospital, Berhampur, Orissa. ABSTRACT BACKGROUND Diseases of skin, mucous membrane and mucocutaneous junctions may also affect the eyes. Physical findings of dermatological disorders and eyes overlap due to three factors- (i) Genodermatoses often affects both skin and eyes because of origin from embryonic ectodermal layers, (ii) Acquired dermatological disorders may affect the mucocutaneous tissue of periorbital regions, (iii) Systemic diseases can manifest as diseases of skin and periocular mucocutaneous tissue because of their superficial anatomical locations. The aim of the present study was observation and interpretation of changes in the eye in different mucocutaneous disorders and correlation of the eye changes with severity of the diseases. MATERIALS AND METHODS A prospective study was undertaken in the Department of Ophthalmology, M.K.C.G. Medical College and Hospital, Berhampur, South Orissa, during the period of 2014 to 2016 including the referred patients after being diagnosed with mucocutaneous disease from Department of Dermatology, Paediatric and Medicine from the same hospital. A case study of 204 patients (M- 164, F-40) was done. All patients underwent detailed ophthalmic examination inclusive of ocular movements, VA, IOP, S/L exam, blood and urine investigation and fundus examination. -

What Are Basal and Squamous Cell Skin Cancers?
cancer.org | 1.800.227.2345 About Basal and Squamous Cell Skin Cancer Overview If you have been diagnosed with basal or squamous cell skin cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to start. ● What Are Basal and Squamous Cell Skin Cancers? Research and Statistics See the latest estimates for new cases of basal and squamous cell skin cancer and deaths in the US and what research is currently being done. ● Key Statistics for Basal and Squamous Cell Skin Cancers ● What’s New in Basal and Squamous Cell Skin Cancer Research? What Are Basal and Squamous Cell Skin Cancers? Basal and squamous cell skin cancers are the most common types of skin cancer. They start in the top layer of skin (the epidermis), and are often related to sun exposure. 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 Cancer starts when cells in the body begin to grow out of control. Cells in nearly any part of the body can become cancer cells. To learn more about cancer and how it starts and spreads, see What Is Cancer?1 Where do skin cancers start? Most skin cancers start in the top layer of skin, called the epidermis. There are 3 main types of cells in this layer: ● Squamous cells: These are flat cells in the upper (outer) part of the epidermis, which are constantly shed as new ones form. When these cells grow out of control, they can develop into squamous cell skin cancer (also called squamous cell carcinoma). -

Thrombotic Thrombocytopenic Purpura Due to Checkpoint Inhibitors
Hindawi Case Reports in Hematology Volume 2018, Article ID 2464619, 4 pages https://doi.org/10.1155/2018/2464619 Case Report Thrombotic Thrombocytopenic Purpura due to Checkpoint Inhibitors Alexey Youssef,1 Nawara Kasso,2 Antonio Sergio Torloni,3 Michael Stanek,4 Tomislav Dragovich,5 Mark Gimbel,6 and Fade Mahmoud 6 1Centre for Tropical Medicine and Global Health, Nuffield Department of Medicine, University of Oxford, Oxford, UK 2Faculty of Medicine, Tishreen University, Lattakia, Syria 3Medical Director, Stem Cell )erapy, Apheresis, and Transfusion Medicine, Banner MD Anderson Cancer Center, Gilbert, AZ, USA 4Division of Hematology, Banner MD Anderson Cancer Center, Gilbert, AZ, USA 5Chief, Division of Medical Oncology and Hematology, Banner MD Anderson Cancer Center, Gilbert, AZ, USA 6)e T.W. Lewis Melanoma Center of Excellence, Banner MD Anderson Cancer Center, Gilbert, AZ, USA Correspondence should be addressed to Fade Mahmoud; [email protected] Received 16 September 2018; Revised 23 November 2018; Accepted 28 November 2018; Published 20 December 2018 Academic Editor: Akimichi Ohsaka Copyright © 2018 Alexey Youssef et al. ,is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Ipilimumab is a monoclonal antibody that enhances the efficacy of the immune system by targeting a cytotoxic T-lymphocyte- associated protein 4 (CTLA-4), which is a protein receptor that downregulates the immune system. Nivolumab is also a hu- manized monoclonal antibody that targets another protein receptor that prevents activated T cells from attacking the cancer; this receptor is called programmed cell death 1 (PD-1). -

XERODERMA PIGMENTOSUM: a MULTIDISCIPLINARY APPROACH Mieran Sethi,1 Alan R
XERODERMA PIGMENTOSUM: A MULTIDISCIPLINARY APPROACH Mieran Sethi,1 Alan R. Lehmann,1,2 Hiva Fassihi1 1. National Xeroderma Pigmentosum Service, Department of Photodermatology, St John’s Institute of Dermatology, Guy’s and St Thomas’ NHS Trust, London, UK 2. Genome Damage and Stability Centre, University of Sussex, Falmer, Brighton, UK Disclosure: No potential conflict of interest. Received: 01.10.2013 Accepted: 06.11.13 Citation: EMJ Dermatol. 2013;1:54-63. ABSTRACT Xeroderma pigmentosum (XP) is a rare, autosomal recessive disorder of DNA repair. Affected individuals are unable to repair ultraviolet radiation (UVR)-induced DNA damage, leading to a variety of clinical manifestations: a dramatic increase in mucocutaneous malignancies, increased lentigines, extreme photosensitivity (in approximately 50% of cases), and neurodegeneration (in approximately 30% of affected individuals). Incidence in Western Europe is recorded as 2.3 per million live births. There are eight different complementation groups, XP-A to XP-G, and XP-variant (XP-V) corresponding to the eight affected genes. Classically, XP patients were identified by clinicians for their tendency to develop severe and exaggerated sunburn on minimal sun exposure, however recently it has been shown that XP-C, XP-E and XP-V patients have normal sunburn reactions for skin type compared to the other groups, who suffer not only with severe, exaggerated sunburn, but also have an increased incidence of neurodegeneration. A diagnosis of XP should be considered in a child with either severe sunburn, increasing lentigines at exposed sites, or development of multiple skin cancers at an early age. Skin biopsy and subsequent testing in cell cultures for defective DNA repair, confirms or excludes the diagnosis. -

Table S1. Checklist for Documentation of Google Trends Research
Table S1. Checklist for Documentation of Google Trends research. Modified from Nuti et al. Section/Topic Checklist item Search Variables Access Date 11 February 2021 Time Period From January 2004 to 31 December 2019. Query Category All query categories were used Region Worldwide Countries with Low Search Excluded Volume Search Input Non-adjusted „Abrasion”, „Blister”, „Cafe au lait spots”, „Cellulite”, „Comedo”, „Dandruff”, „Eczema”, „Erythema”, „Eschar”, „Freckle”, „Hair loss”, „Hair loss pattern”, „Hiperpigmentation”, „Hives”, „Itch”, „Liver spots”, „Melanocytic nevus”, „Melasma”, „Nevus”, „Nodule”, „Papilloma”, „Papule”, „Perspiration”, „Petechia”, „Pustule”, „Scar”, „Skin fissure”, „Skin rash”, „Skin tag”, „Skin ulcer”, „Stretch marks”, „Telangiectasia”, „Vesicle”, „Wart”, „Xeroderma” Adjusted Topics: "Scar" + „Abrasion” / „Blister” / „Cafe au lait spots” / „Cellulite” / „Comedo” / „Dandruff” / „Eczema” / „Erythema” / „Eschar” / „Freckle” / „Hair loss” / „Hair loss pattern” / „Hiperpigmentation” / „Hives” / „Itch” / „Liver spots” / „Melanocytic nevus” / „Melasma” / „Nevus” / „Nodule” / „Papilloma” / „Papule” / „Perspiration” / „Petechia” / „Pustule” / „Skin fissure” / „Skin rash” / „Skin tag” / „Skin ulcer” / „Stretch marks” / „Telangiectasia” / „Vesicle” / „Wart” / „Xeroderma” Rationale for Search Strategy For Search Input The searched topics are related to dermatologic complaints. Because Google Trends enables to compare only five inputs at once we compared relative search volume of all topics with topic „Scar” (adjusted data). Therefore, -

Diagnosis and Management of Cutaneous Psoriasis: a Review
FEBRUARY 2019 CLINICAL MANAGEMENT extra Diagnosis and Management of Cutaneous Psoriasis: A Review CME 1 AMA PRA ANCC Category 1 CreditTM 1.5 Contact Hours 1.5 Contact Hours Alisa Brandon, MSc & Medical Student & University of Toronto & Toronto, Ontario, Canada Asfandyar Mufti, MD & Dermatology Resident & University of Toronto & Toronto, Ontario, Canada R. Gary Sibbald, DSc (Hons), MD, MEd, BSc, FRCPC (Med Derm), ABIM, FAAD, MAPWCA & Professor & Medicine and Public Health & University of Toronto & Toronto, Ontario, Canada & Director & International Interprofessional Wound Care Course and Masters of Science in Community Health (Prevention and Wound Care) & Dalla Lana Faculty of Public Health & University of Toronto & Past President & World Union of Wound Healing Societies & Editor-in-Chief & Advances in Skin and Wound Care & Philadelphia, Pennsylvania The author, faculty, staff, and planners, including spouses/partners (if any), in any position to control the content of this CME activity have disclosed that they have no financial relationships with, or financial interests in, any commercial companies pertaining to this educational activity. To earn CME credit, you must read the CME article and complete the quiz online, answering at least 13 of the 18 questions correctly. This continuing educational activity will expire for physicians on January 31, 2021, and for nurses on December 4, 2020. All tests are now online only; take the test at http://cme.lww.com for physicians and www.nursingcenter.com for nurses. Complete CE/CME information is on the last page of this article. GENERAL PURPOSE: To provide information about the diagnosis and management of cutaneous psoriasis. TARGET AUDIENCE: This continuing education activity is intended for physicians, physician assistants, nurse practitioners, and nurses with an interest in skin and wound care. -

Skin Signs of Rheumatic Disease Gideon P
Skin Signs of Rheumatic Disease Gideon P. Smith MD PhD MPH Vice Chair for Clinical Affairs Director of Rheumatology-Dermatology Program Director of Connective Tissue Diseases Fellowship Associate Director of Clinical Trials Department of Dermatology Massachusetts General Hospital Harvard University www.mghcme.org Disclosures “Neither I nor my spouse/partner has a relevant financial relationship with a commercial interest to disclose.” www.mghcme.org CONNECTIVE TISSUE DISEASES CLINIC •Schnitzlers •Interstitial •Chondrosarcoma •Eosinophilic Fasciitis Granulomatous induced •Silicone granulomas Dermatitis with Dermatomyositis Arthritis •AML arthritis with •Scleroderma granulomatous papules •Cutaneous Crohn’s •Lyme arthritis with with arthritis •Follicular mucinosis in papular mucinosis JRA post-infliximab •Acral Anetoderma •Celiac Lupus •Calcinosis, small and •Granulomatous exophytic •TNF-alpha induced Mastitis sarcoid •NSF, Morphea •IgG4 Disease •Multicentric Reticul •EED, PAN, DLE ohistiocytosis www.mghcme.org • Primary skin disease recalcitrant to therapy Common consults • Hair loss • Nail dystrophy • Photosensitivity • Cosmetic concerns – post- inflammatory pigmentation, scarring, volume loss, premature photo-aging • Erythromelalgia • Dry Eyes • Dry Mouth • Oral Ulcerations • Burning Mouth Syndrome • Urticaria • Itch • Raynaud’s • Digital Ulceration • Calcinosis cutis www.mghcme.org Todays Agenda Clinical Presentations Rashes (Cutaneous Lupus vs Dermatomyositis vs ?) Hard Skin (Scleroderma vs Other sclerosing disorders) www.mghcme.org -

An Uncommon but Often Lethal Skin Cancer Could Be That Individual Melanoma Patients Cancers Can Be Assessed by Gene Expression to Answer These Questions
HEALTH in the US and Australia are successfully actions of vitamin D, genetic alterations CONCLUSION treated by early surgery. However, 10 in the gene that controls the vitamin D At this point, the role of genetics in percent of melanomas have been highly receptor or related genes might reasonably melanoma is still unclear. While intense, recalcitrant to treatment. In the quest for be associated with poorer survival from intermittent sun exposure is clearly better understanding, multiple investiga- melanoma. It may be that individuals who important in the etiology of melanoma, tors are evaluating the role of genetic factors have aggressive melanoma have a different its importance for survival is not known. in survival. While excessive, intermittent set of genetic mutations from those com- Therefore, one cannot reliably say whether sun exposure is an important risk factor mon in more indolent melanomas. nature or nurture (i.e., behavior) is more Merkel Cell Carcinoma: for melanoma, it does not appear to be as- The genetic factors associated with important in either the etiology or the sociated with poorer melanoma survival. melanoma progression and survival are progression of melanoma. Hopefully, this Thus, genetic factors may be the culprit; it still being explored. While genetics in other uncertainty will continue to spur research An Uncommon But Often Lethal Skin Cancer could be that individual melanoma patients cancers can be assessed by gene expression to answer these questions. JAYASRI IYER, MD, AND PAUL NGHIEM, MD, PHD with a particular constellation of inherited analyses from fresh tumor tissue, this is ex- genetic mutations are those who have tremely difficult in melanoma, as primary DR. -

A Brighter Future for Psoriasis Patients Melanoma and Skin Cancer Center
Skin Health FROM THE MOUNT SINAI DEPARTMENT OF DERMATOLOGY FALL 2013 MESSAGE FROM THE CHAIR A Brighter Future for Psoriasis Patients By Mark G. Lebwohl, MD, Sol and Clara Kest Professor and Chair ount Sinai has been at the forefront of psoriasis research since Mthe 1980’s, when we introduced a topical combination regimen that remains the standard of care around the world even today. This consists of both a superpotent corticosteroid and a vitamin-D analog such as calcipotriene (Dovonex®) or calcitriol (Vectical®). The use of combination therapy led to the invention of Taclonex®, a popular and effective psoriasis formula that contains two topical agents. While refining the concept of combination therapy, we discovered that some topical preparations inactivate others, and subsequently we fostered the understanding that two or more ingredients, when applied together, must be shown to be compatible. In recent years this rule has been Dr. Mark G. Lebwohl embraced for all topical medicines, not just for psoriasis drugs. continued on page 4 BREAKING NEWS In This Issue Melanoma and Skin Cancer Center By Philip Friedlander, MD, PhD LASER HAIR REMOVAL Alan Kling, MD Page 2 he Tisch Cancer Institute is pleased to announce the creation of the Melanoma and TSkin Cancer Center, a virtual gathering place designed to provide a full array of medical LOOKING FAB THIS FALL resources to skin cancer patients. As part of its mission to deliver the highest quality of care, David S. Orentreich, MD the Center has assembled a team of leading specialists representing the fields of dermatology, Marina I. Peredo, MD medical oncology, surgery, dermatopathology, podiatry, and social work. -

Merkel Cell Carcinoma: Update and Review Timothy S
Merkel Cell Carcinoma: Update and Review Timothy S. Wang, MD,* Patrick J. Byrne, MD, FACS,† Lisa K. Jacobs, MD,‡ and Janis M. Taube, MD§ Merkel cell carcinoma (MCC) is a rare, aggressive, and often fatal cutaneous malignancy that is not usually suspected at the time of biopsy. Because of its increasing incidence and the discovery of a possible viral association, interest in MCC has escalated. Recent effort has broadened our breadth of knowledge regarding MCC and developed instruments to improve data collection and future study. This article provides an update on current thinking about the Merkel cell and MCC. Semin Cutan Med Surg 30:48-56 © 2011 Elsevier Inc. All rights reserved. erkel cell carcinoma (MCC) is a rare, aggressive, and current thinking, including novel insights into the Merkel Moften fatal cutaneous malignancy. It usually presents as cell; a review of the 2010 National Comprehensive Cancer a banal-appearing lesion and the diagnosis is rarely suspected Network (NCCN) therapeutic guidelines and new American at the time of biopsy. Because of increasing incidence and the Joint Committee on Cancer (AJCC) staging system; recom- discovery of a possible viral association, interest in MCC has mendations for pathologic reporting and new diagnostic escalated rapidly. codes; and the recently described Merkel cell polyoma virus From 1986 to 2001, the incidence of MCC in the United (MCPyV). States has tripled, and approximately 1500 new cases are diagnosed each year.1,2 MCC occurs most frequently among elderly white patients and perhaps slightly more commonly History in men. MCCs tend to occur on sun-exposed areas, with Merkel cells (MCs) were first described by Friedrich Merkel 3 nearly 80% presenting on the head, neck, and extremities. -

Treatment of Psoriasis After Initiation of Nivolumab Therapy for Metastatic Malignant Melanoma: an Ancient Drug Revisited
LETTER TO THE EDITOR DOI: 10.4274/jtad.galenos.2020.13007 J Turk Acad Dermatol 2020;14(3):93-94 Treatment of Psoriasis After Initiation of Nivolumab Therapy for Metastatic Malignant Melanoma: An Ancient Drug Revisited Gökhan Okan1, Kezban Nur Pilancı2, Cuyan Demirkesen3 1Private Dermatologist, Istanbul, Turkey 2Memorial Bahcelievler Hospital, Clinic of Oncology, Istanbul, Turkey 3Acibadem University Faculty of Medicine, Department of Pathology, Istanbul, Turkey Keywords: Checkpoint inhibitors, Nivolumab, Psoriasis, Melanoma, Sulfasalazine Dear Editor, Checkpoint inhibition can cause various immune-related adverse events in any organ but skin toxicity occurs most frequently [1]. We report de novo development of psoriasis vulgaris in a patient receiving nivolumab for treatment of metastatic melanoma which was controlled with sulfasalazine (SSZ). A 69-year-old male was initiated with nivolumab 3 mg/kg every two weeks for metastatic BRAF-negative melanoma of the back. The patient’s medical history was notable for arterial hypertension and dyslipidemia for which he has been medically treated. There was no personal or family history of psoriasis. One week after the fourth cycle of nivolumab, asymptomatic, sharply bordered, erythematous and scaly plaques were seen on the the anterolateral aspects of shins, dorsa of hands, feet, scalp, and trunk (Figure 1a). A skin biopsy revealed psoriasiform epidermal hyperplasia with prominent orthohyperkeratosis, and mounds of parakeratosis, containing neutrophils. The suprapapillary epidermis was thinned, and there were collections of neutrophils in the spinous layers which were consistent with psoriasis (Figure 1b, 1c). The patient had psoriasis area and severity index score of 12. He did not have psoriatic arthritis. The patient’s melanoma improved with nivolumab therapy but the skin lesions increased.