Evolution of the Extraglottic Airway: a Review of Its History, Applications, and Practical Tips for Success Michael R
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
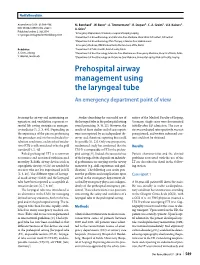
Prehospital Airway Management Using the Laryngeal Tube an Emergency Department Point of View
Notfallmedizin Anaesthesist 2014 · 63:589–596 M. Bernhard1 · W. Beres2 · A. Timmermann3 · R. Stepan4 · C.-A. Greim5 · U.X. Kaisers6 · DOI 10.1007/s00101-014-2348-1 A. Gries1 Published online: 2. Juli 2014 1 Emergency Department, University Hospital of Leipzig, Leipzig © Springer-Verlag Berlin Heidelberg 2014 2 Department of Anaesthesiology and Intensive Care Medicine, Main Klinik Ochsenfurt, Ochsenfurt 3 Department of Anaesthesiology, Pain Therapy, Intensive Care Medicine and Emergency Medicine, DRK Kliniken Berlin Westend und Mitte, Berlin Redaktion 4 Department of Public Health, Fulda County, Fulda A. Gries, Leipzig 5 Department of Anesthesiology, Intensive Care Medicine and Emergency Medicine, Hospital of Fulda, Fulda V. Wenzel, Innsbruck 6 Department of Anesthesiology and Intensive Care Medicine, University Leipzig, Medical Faculty, Leipzig Prehospital airway management using the laryngeal tube An emergency department point of view Securing the airway and maintaining ox- Studies describing the successful use of mittee of the Medical Faculty of Leipzig, ygenation and ventilation represent es- the laryngeal tube in the prehospital setting Germany. Single cases were documented sential life-saving strategies in emergen- sound promising [9, 10, 22]. However, the initially after ED admission. The case se- cy medicine [1, 2, 3, 40]. Depending on results of these studies and of case reports ries was evaluated retrospectively, was not the experience of the person performing were not reported by an independent ob- preregistered, and written informed con- the procedure and on the individual in- server and, therefore, reporting bias could tent could not be obtained. tubation conditions, endotracheal intuba- be possible [11, 22]. Only one prospective, tion (ETI) is still considered to be the gold randomized study has confirmed that the Results standard [4, 5, 40]. -

Evaluation of Different Positive End-Expiratory Pressures Using Supreme™ Airway Laryngeal Mask During Minor Surgical Procedure
medicina Article Evaluation of Different Positive End-Expiratory Pressures Using Supreme™ Airway Laryngeal Mask during Minor Surgical Procedures in Children Mascha O. Fiedler 1,* , Elisabeth Schätzle 2, Marius Contzen 3, Christian Gernoth 4, Christel Weiß 5, Thomas Walter 6, Tim Viergutz 2 and Armin Kalenka 7 1 Clinic of Anesthesiology, Heidelberg University Hospital, 69120 Heidelberg, Germany 2 Clinic of Anesthesiology and Surgical Intensive Care Medicine, University Medical Centre Mannheim, 68167 Mannheim, Germany; [email protected] (E.S.); [email protected] (T.V.) 3 Department of Anesthesiology and Intensive Care Medicine, Heilig-Geist-Hospital Bensheim, 64625 Bensheim, Germany; [email protected] 4 Department of Anesthesiology, Surgical Intensive Care Medicine, Pain Therapy, Helios Hospital Duisburg, 47166 Duisburg, Germany; [email protected] 5 Department of Medical Statistics, University Medical Centre Mannheim, 68167 Mannheim, Germany; [email protected] 6 Emergency Department, University Medical Centre Mannheim, 68167 Mannheim, Germany; [email protected] 7 Department of Anesthesiology and Intensive Care Medicine, Hospital Bergstrasse, 64646 Heppenheim, Germany; [email protected] * Correspondence: mascha.fi[email protected]; Tel.: +49-(0)-6222-1563-9434 Received: 21 September 2020; Accepted: 19 October 2020; Published: 21 October 2020 Abstract: Background and objectives: The laryngeal mask is the method of choice for airway management in children during minor surgical procedures. There is a paucity of data regarding optimal management of mechanical ventilation in these patients. The Supreme™ airway laryngeal mask offers the option to insert a gastric tube to empty the stomach contents of air and/or gastric juice. -

The Laryngeal Mask Airway: Potential Applications in Neonates
F485 Arch Dis Child Fetal Neonatal Ed: first published as 10.1136/adc.2003.038430 on 21 October 2004. Downloaded from PERSONAL PRACTICE The laryngeal mask airway: potential applications in neonates D Trevisanuto, M Micaglio, P Ferrarese, V Zanardo ............................................................................................................................... Arch Dis Child Fetal Neonatal Ed 2004;89:F485–F489. doi: 10.1136/adc.2003.038430 The laryngeal mask airway is a safe and reliable airway 2.5–5 kg.11 It has been postulated that a smaller size (0.5) could be useful in preterm management device. This review describes the insertion newborns. However, there are reports of techniques, advantages, limitations, and potential successful use of size 1 in preterm neonates applications of the laryngeal mask airway in neonates. weighing 0.8–1.5 kg.12–15 ........................................................................... (2) Fully deflate the cuff as described in the manual, and lubricate the back of the mask tip (for neonates in the labour ward, he ability to maintain a patent airway and lubrication may not be necessary, as oral provide effective positive pressure ventilation and pharyngeal secretions may reproduce T(PPV) is the main objective of neonatal this function). resuscitation and all anaesthesiological proce- (3) Press (flatten) the tip of the LMA against the dures.1–6 This is currently achieved with the use hard palate. During this manoeuvre, the of a face mask or an endotracheal tube. Both of these devices have major limitations from a operator should grasp the LMA like a pen strictly anatomical point of view and require with the index finger at the junction adequate operator skills. In certain situations, between the mask and the distal end of the both face mask ventilation and tracheal intuba- airway tube. -

A Randomized Prospective Controlled Trial Comparing the Laryngeal Tube
Somri et al. BMC Anesthesiology (2016) 16:87 DOI 10.1186/s12871-016-0237-7 RESEARCH ARTICLE Open Access A randomized prospective controlled trial comparing the laryngeal tube suction disposable and the supreme laryngeal mask airway: the influence of head and neck position on oropharyngeal seal pressure Mostafa Somri1, Sonia Vaida3, Gustavo Garcia Fornari4,6, Gabriela Renee Mendoza4,6, Pedro Charco-Mora5,6, Naser Hawash1, Ibrahim Matter2, Forat Swaid2 and Luis Gaitini1,6* Abstract Background: The Laryngeal Tube Suction Disposable (LTS-D) and the Supreme Laryngeal Mask Airway (SLMA) are second generation supraglottic airway devices (SADs) with an added channel to allow gastric drainage. We studied the efficacy of these devices when using pressure controlled mechanical ventilation during general anesthesia for short and medium duration surgical procedures and compared the oropharyngeal seal pressure in different head and-neck positions. Methods: Eighty patients in each group had either LTS-D or SLMA for airway management. The patients were recruited in two different institutions. Primary outcome variables were the oropharyngeal seal pressures in neutral, flexion, extension, right and left head-neck position. Secondary outcome variables were time to achieve an effective airway, ease of insertion, number of attempts, maneuvers necessary during insertion, ventilatory parameters, success of gastric tube insertion and incidence of complications. Results: The oropharyngeal seal pressure achieved with the LTS-D was higher than the SLMA in, (extension (p=0.0150) and right position (p=0.0268 at 60 cm H2O intracuff pressures and nearly significant in neutral position (p = 0.0571). The oropharyngeal seal pressure was significantly higher with the LTS-D during neck extension as compared to SLMA (p= 0.015). -
Lmas: Airway Management and Inhalant Anesthetics
LMAsLMAs:: AirwayAirway ManagementManagement andand InhalantInhalant AnestheticsAnesthetics Wanda O.Wilson, PhD, CRNA University of Cincinnati College of Nursing Nurse Anesthesia Major LMA:LMA: HistoryHistory First described by Dr. A. Brain. Introduced in the 1980’s in UK •In US in 1992 Alternative to mask and endotracheal intubation. Estimated over 200 million surgeries performed with LMA worldwide Brain AIJ: The Laryngeal Mask – A New Concept in Airway Management. Br J Anaesth; 55:801, 1983 LMA:LMA: HistoryHistory General Safety and Efficacy of the LMA • 39,824 patients underwent GA; 11,910 (30%) airways were managed with LMA 99.8% successful placement (LMA abandoned in 23 patients) 44% underwent PPV 44 critical incidents; 18 related to airway (none serious) Verghese C & Brimacombe JR: Anesth Analg; 82:129, 1996 LMALMA UseUse inin PediatricsPediatrics Mason & Bingham. Anaesthesia; 45:760, 1990 • 200 children • Difficulties encountered in 47 cases (23%), but LMA use abandoned in only 5 cases (2.5%). • Down folding of epiglottis over laryngeal inlet identified in 8 out of 24 patients where flexible laryngoscopy was performed; clinically all had unobstructed airways. LMA:LMA: AdvantagesAdvantages Advantages over ET tube and face mask: Improved hemodynamic stability at induction & during emergence. Maintenance of airway while freeing hands & reducing fatigue of Anesthetist. Avoidance of facial nerve & eye injuries due to face mask. Decreased frequency of coughing during emergence. Decreased incidence of sore throat. DecreasedDecreased CoughingCoughing withwith LMALMA 79 patients undergoing cataract surgery, randomized to ETT or LMA. • Greater incidence of coughing prior to, during, & after extubation in ETT group. Denny & Gadeirab. J Royal Soc Med; 86:521,1993 29 patients undergoing elective eye surgery under GA randomized to ETT or LMA. -

Basic Airway Management & Decision Making
Roberts: Clinical Procedures in Emergency Medicine, 5th ed. CHAPTER 3 – Basic Airway Management and Decision-Making Robert F. Reardon, Phillip E. Mason, Joseph E. Clinton Over the last few decades, several important changes have occurred in emergency airway management. Bag-mask ventilation has been supplemented by intermediate, or backup, ventilation devices like the laryngeal mask airway (LMA), the Combitube, and the laryngeal tube. These have become important devices for the initial resuscitation of apneic patients and for rescue ventilation when intubation fails.[1] Noninvasive positive-pressure ventilation (NPPV) is now used in place of tracheal intubation in some critically ill patients. Despite these advances, basic techniques such as opening the airway, oxygenation, and bag-mask ventilation remain the cornerstones of good emergency airway management. [2] [3] Airway maintenance without endotracheal intubation is one of the most important emergency [4] airway management techniques to keep patients alive until a definitive airway can be established. This chapter describes basic airway skills including opening the airway, O2 therapy, NPPV, bag-mask ventilation, and intermediate ventilation devices. Because of the complexity of these skills and decisions, providers should develop a simple, organized approach to emergency airway management, being cognizant that when a specific intervention has failed, it is time to move rapidly to a different approach. Developing a simple preconceived algorithm that employs proven techniques and is applicable to a broad range of clinical scenarios will help providers manage difficult, anxiety-provoking emergency airways. THE CHALLENGE OF EMERGENCY AIRWAY MANAGEMENT Although other specialists are sometimes available, most emergency airways are managed by emergency clinicians.[5] Airway management in the emergency department (ED) is much different from airway management in the controlled setting of the operating room. -

Comparing No-Flow Time During Endotracheal Intubation Versus Placement of a Laryngeal Mask Airway During a Simulated Cardiac Arrest Scenario
Empirical Investigations Comparing No-Flow Time During Endotracheal Intubation Versus Placement of a Laryngeal Mask Airway During a Simulated Cardiac Arrest Scenario Vincent J. Miller, MD; Introduction: Traditionally, pausing chest compressions during airway management in a cardiac arrest has been the accepted norm. However, updated American Heart Erin E. Flaherty, MD Association and the European Resuscitation Council guidelines for Advanced Cardiac Life Support emphasize reducing pauses in chest compressions, often referred to as ‘‘no-flow time,’’ to improve return of spontaneous circulation. We used simulation to evaluate whether placing a laryngeal mask airway versus endotracheal intubation via direct laryngoscopy would reduce no-flow times during a simulated cardiac arrest. Methods: A crossover trial of 41 respiratory therapists (RTs) performed airway man- agement in a simulated cardiac arrest. The RTs were told that bag mask ventilation was inadequate, and either an endotracheal tube or laryngeal mask airway was needed. They were informed to request the cessation of chest compressions only if needed to complete the airway maneuver. The study was terminated when ventilation was achieved. The scenario was repeated with the same RT placing the alternative airway. Insertion time and no-flow times were recorded. Results: Neither endotracheal intubation via direct laryngoscopy nor laryngeal mask airway placement increased no-flow time. Only 1 participant requested cessation of chest compressions during direct laryngoscopy for 2.3 seconds (P = 0.175). However, ventilation was established significantly faster with a laryngeal mask airway compared with endotracheal intubation (49.2 vs. 31.6 seconds, respectively, P G 0.001). Conclusions: We conclude that although neither device was superior to the other with respect to the primary outcome of reducing no-flow time, effective ventilation was established more rapidly with the laryngeal mask airway in the hands of the RTs who participated in this study. -
Everything You Need to Know
Anesthesia 101 Everything you need to know Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. 2.8 1.5 ANCC CONTACT HOURS CONTACT HOURS By Laura Palmer, DNP, CRNA, MNEd Successful patient outcomes from an operative procedure require vigilance, diligence, and teamwork among the various providers involved with the surgical procedure. An understanding of the responsibilities and appreciation for the complexities of each healthcare provider’s role in the operative process is essential to a harmonious relationship among the perioperative Steam to improve the working environment and provide safe patient care. The information provided in this article is based on commonly observed practices in the anesthesia community with the caveat that the choices can vary considerably and are influenced by patient presentation and surgical requirements. Provision of anesthesia services Several regulatory agencies at state and federal levels, along with reimburse- ment requirements, control who can provide anesthesia services. Providers are generally limited to physicians, certified registered nurse anesthetists (CRNAs), and anesthesia assistants (AAs) in a limited number of states. The practice patterns commonly seen are: anesthesiologists or CRNAs indepen- dently providing direct anesthesia care, CRNAs and anesthesiologists work- ing together in the anesthesia care team model, or physicians medically directing AAs. CRNAs receive direct reimbursement from the Centers for Medicare and Medicaid Services, but AAs must always work with anesthesiologists in the medical direction model.1 Although the provider administering anesthesia can vary by practice setting and geographic location, the process and goals are comparable. Types of anesthesia When anesthesia services are necessary, there are several options to provide the patient with pain relief, reduce anxiety, and meet the requirements of the surgical procedure. -

This Procedure Includes the Following: • Endotracheal Intubation (Plus Use of Supraglottic Airway Laryngopharyngeal Tube (S.A
ADVANCED AIRWAY PROCEDURES This procedure includes the following: Endotracheal intubation (plus use of Supraglottic Airway Laryngopharyngeal Tube (S.A.L.T. device), gum elastic bougie assisted tracheal intubation, video laryngoscopy) Non-Visualized Airways (Dual lumen airway, King LT-D™ Airway, Laryngeal Mask Airway (LMA)) Cricothyroidotomy – needle and surgical GENERAL CONSIDERATIONS Rescuers must be aware of the risks and benefits of advanced airway management techniques. In cases of cardiac arrest the insertion of an advanced airway may require interruption of chest compressions for many seconds, the rescuer should weigh the need for compressions against the need for insertion of an advanced airway. Rescuers may defer insertion of an advanced airway until the patient fails to respond to initial CPR and defibrillation attempts or demonstrates return of spontaneous circulation. Providers should have a second (back-up) strategy for airway management and ventilation if they are unable to establish the first-choice airway adjunct. Bag-mask ventilation may provide that back-up strategy. ENDOTRACHEAL INTUBATION A. Indications for emergency endotracheal intubation are: 1. Inability of the rescuer to adequately ventilate the patient with a bag-mask device 2. The absence of airway protective reflexes (coma and cardiac arrest) B. In most case, endotracheal intubation provides definite control of the airway. Its purposes include: 1. Actively ventilating the patient 2. Delivering high concentrations of oxygen 3. Suctioning secretions and maintaining airway patency 4. Preventing aspiration of gastric contents, upper airway secretions or blood 5. Prevented gastric distention due to assisted ventilations 6. Administering positive pressure when extra fluid is present in alveoli 7. Administering medications during resuscitation for absorption through lungs as a last resort C. -
Effect of a Strategy of Initial Laryngeal Tube Insertion Vs Endotracheal
Pragmatic Trial of Airway Management in Out-of-Hospital Cardiac Arrest (Pragmatic Airway Resuscitation Trial) Clinical Trial Protocol Version 5.0 February 19, 2015 –revised and approved protocol Version 5.1 April 1, 2015 –Minor changes to DSMB revised and approved protocol Version 6.0 July 13, 2016 – Minor updates Version 7.0 November 29, 2016 – Revisions PRAGMATIC AIRWAY RESUSCITATION TRIAL This trial protocol is adapted with permission from the ROC CCC Trial protocol. This protocol may not be used or reproduced without permission. Downloaded From: https://jamanetwork.com/ on 09/28/2021 Pragmatic Airway Resuscitation Trial Version 7.0 – November 29, 2016 Clinical Trial Protocol TABLE OF CONTENTS 1. Key Study Information ........................................................................................................ 5 1.1 Clinical Trial Registration .................................................................................................... 5 1.2 Funding and Support .......................................................................................................... 5 1.3 Study Leadership and Key Personnel ................................................................................. 5 1.3.1 Principal Investigator, Lead Facilitator ..........................................................................5 1.3.2 Co-Investigators ...........................................................................................................5 2. Acronyms and Abbreviations ............................................................................................ -

Airway Management
AIRWAY MANAGEMENT Angkana Lurngnateetape, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is “management of the patient’s airway” Miller RD’s Anesthesia 2000 Barash PG, Cullen BF, Stoelting RK’s Clinical Anesthesia 2001 What should we know about “airway management”? ● Airway anatomy and function ● Evaluation of airway ● Clinical management of the airway - Maintenance and ventilation - Intubation and extubation - Difficult airway management Airway anatomy The term “airway” refers to the upper airway, consisting of ● Nasal and oral cavities ● Pharynx ● Larynx ● Trachea ● Principle bronchi Anatomy of upper airway Larynx in laryngoscopic view Nerves V1 V2 V3 IX Vagus nerve • Superior laryngeal n – External br (Motor) • cricothyroid m SL – Internal br (Sensory) • area above cord • Recurrent laryngeal n - Motor br • intrinsic m RL – Sensory br • area below cord Evaluation of the airway ● History ● Physical examination ● Special investigation Evaluation of the airway “History” ● Previous history of difficult airway ● Airway-related untoward events ● Airway-related symptoms/diseases Evaluation of the airway Physical examination ● Ease of open airway and maintenance ● Ease of tracheal intubation ● Teeth ● Neck movement ● Intubation hazards ● Signs of airway distress Evaluation of the airway Anatomic characteristics associated with difficult airway management ● Short muscular neck ● Receding mandible ● Protruding maxillary incisors ● Long high-arched palate ● Inability to visualize -

Comparison of Midazolam and Dexmedetomidine As an Adjuvant
Global Anesthesia and Perioperative Medicine Research Article ISSN: 2059-0512 Comparison of midazolam and dexmedetomidine as an adjuvant for proseal laryngeal mask airway insertion: A randomized control trial Satveer Singh Gurjar1, Babita1, Kamlesh Kumar Sharma1, Roncall Bhim Raju2, Bhupendra Singh1 and Rakesh Karnawat2* 1Department of Anesthesia, S.N Medical College, Jodhpur, Rajasthan, India 2Senior Residence, AIIMS, New Delhi, India Abstract Background: Proseal Laryngeal mask airway(PLMA), a modification of classical LMA, is safe and effective alternative airway device to endotracheal intubation. PLMA incorporates a drain tube ending at the tip so that there are less chances of aspiration. Use of muscle relaxant is not a must for PLMA insertion. Methods: 100 patients of ASA grade I/II divided in two groups (50 in each group). Group A received inj. midazolam 0.03 mg kg-1IV and group B received inj. dexmedetomidine 0.4 mcg kg-1. Induction was done with inj. propofol 2.5 mg/kg IV. Ease of PLMA insertion without using muscle relaxant was studded. Time taken and number of insertion attempts, intraoperative haemodynamic parameters and complications were recorded. Results: The resistance to mouth opening was significantly less (p=0.003) in the group B(significant resistance encountered in 2% cases) in compare togroup A (14% cases).The PLMA insertion conditions were better in group B compared to the group A (p<0.05). Time taken (11.48 ± 3.34 sec)and number of attempts in PLMA insertion were significantly less (p<0.05) in group B when compare to group A (11.48 ± 3.34 sec) without significant intraoperative haemodynamic changes except at 5th min post-insertion.