Harborough District Profile
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Network Rail MHLSI Works.Pub
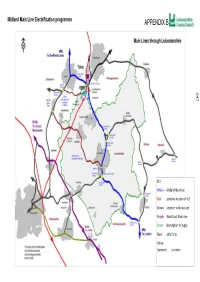
Midland Main Line Electrification programme 247 KEY MMLe — Midland Main Line Red potenal locaon of Hs2 Brown Leicester to Burton Line Purple West Coast Main Line Green Birmingham to ugby Black other lines Yellow diamonds %uncons POST HENDY REVIEW—UPDATE The Hendy Enhancements delivery plan update (Jan 2016) Electrification of the Midland Main Line has resumed under plans announced as part of Sir Peter Hendy’s work to reset Network Rail’s upgrade programme. Work on electrifying the Midland Main Line, the vital long-distance corridor that serves the UK’s industrial heartland, will continue alongside the line-speed and capacity improvement works that were already in hand. Electrification of the line north of Bedford to Kettering and Corby is scheduled to be completed by 2019, and the line north of Kettering to Leicester, Derby/Nottingham and Sheffield by 2023. Outputs The Midland Main line Electrification Programme known as the MMLe is split into two key output dates, the first running from 2014-2019 (known as CP5) and the second, 2019-2023 (CP6). There are a number of sub projects running under the main MMLe programme which are delivering various improvements in the Leicestershire area. Each sub project has dependencies with each other to enable the full ES001- Midland Main Line electrification programme to be achieved A number of interfaces and assumptions link to these programmes and their sub projects will affect Leicestershire. ES001A- Leicester Capacity The proposed 4 tracking between Syston and Wigston is located under sub project ES001A - Leicester Capacity which can be found on page 27 of Network Rails enhancements delivery plan . -
Report to the Development Control and Regulatory Board – 13Th November 2003
REPORT TO THE DEVELOPMENT CONTROL AND REGULATORY BOARD – 13TH NOVEMBER 2003 PROPOSED DEFINITIVE MAP MODIFICATION ORDER UPGRADING OF PUBLIC FOOTPATH C9 TO A BRIDLEWAY (C10) AND ADDITION OF PUBLIC FOOTPATH C104 AT SCOTLAND, BURTON OVERY REPORT OF THE CHIEF EXECUTIVE PART A PURPOSE 1. The purpose of this report is to seek the Board’s approval of the above- mentioned proposal. Recommendation 2. It is recommended that an Order be made under the provisions of Section 53 of the Wildlife and Countryside Act 1981, the effect of which will be to upgrade footpath C9 to a bridleway and also add footpath C104 at Scotland, Burton Overy to the Definitive Map of Public Rights of Way for Leicestershire, as shown on the plan attached to this report. Reason for Recommendation 3. That the statutory criteria in Section 53 of the Wildlife and Countryside Act 1981, have been met by historic evidence which supports the proposed modifications to the Definitive Map of Public Rights of Way. Circulation under Sensitive Issues Procedure 4. Dr. R.K.A. Feltham, County Councillor. Officer to Contact 5. Mr. Gary Jackson, Chief Executive’s Department, Tel 0116 2656159. PART B Background 6. During survey work carried out by an officer of this Council, it was observed that an inconsistency may exist between the use of the routes on the ground and the routes recorded on the Definitive Map. 7. Following investigation of the routes in question by the Director of Community Services, the matter is now being processed under the provisions of Section 53 of the Wildlife and Countryside Act 1981. -

Covid-19-Weekly-Hotspot-Report-For
Weekly COVID-19 Surveillance Report in Leicestershire Cumulative data from 01/03/2020 - 29/09/2021 This report summarises the information from the surveillance system which is used to monitor the cases of the Coronavirus Disease 2019 (COVID-19) pandemic in Leicestershire. The report is based on daily data up to 29th September 2021. The maps presented in the report examine counts and rates of COVID-19 at Middle Super Output Area. Middle Layer Super Output Areas (MSOAs) are a census based geography used in the reporting of small area statistics in England and Wales. The minimum population is 5,000 and the average is 7,200. Disclosure control rules have been applied to all figures not currently in the public domain. Counts between 1 to 5 have been suppressed at MSOA level. An additional dashboard examining weekly counts of COVID-19 cases by Middle Super Output Area in Leicestershire, Leicester and Rutland can be accessed via the following link: https://public.tableau.com/profile/r.i.team.leicestershire.county.council#!/vizhome/COVID-19PHEWeeklyCases/WeeklyCOVID- 19byMSOA Data has been sourced from Public Health England. The report has been complied by Business Intelligence Service in Leicestershire County Council. Weekly COVID-19 Surveillance Report in Leicestershire Cumulative data from 01/03/2020 - 29/09/2021 Breakdown of testing by Pillars of the UK Government’s COVID-19 testing programme: Pillar 1 + 2 Pillar 1 Pillar 2 combined data from both Pillar 1 and Pillar 2 data from swab testing in PHE labs and NHS data from swab testing for the -

Moving Order A426 Lutterworth, Bitteswell and Ashby Parva HTWMT
THE LEICESTERSHIRE COUNTY COUNCIL fA426 LUTTERWORTH, BITTESWELL AND ASHBY PARVA) (DISTRICT OF HARBOROUGH AND DISTRICT OF BLABY) . ~ (IMPOSITION OF 50 MPH SPEED LIMIT) ORDER 2020 The Leicestershire County Council ("the Council") in exercise of its powers under Sections 5 and 84 and Part IV of Schedule 9 of the Road Traffic Regulation Act 1984 ("the Act") and of all other enabling powers and after consultation with the chief officer of police in accordance with Part III of Schedule 9 to the Act, hereby makes the following Order:- 1. This Order may be cited as "The Leicestershire County Council (A426 Lutterworth, Bitteswell and Ashby Parva) (District of Harborough and District of Blaby) (Imposition of 50 mph Speed Limit) Order 2020" 2. The order shall come into force on the 16th day of March 2020. 3. No person shall drive any motor vehicle at a speed exceeding 50 miles per hour on the roads specified in the Schedule to this order. 4. The plan annexed to this Order and marked 'Drawing No. P640/T1/1' is for identification purposes only. SCHEDULE A426, Lutterworth Road From a point 165 metres south of its junction with Dog and Gun Lane, Whetstone to a point 257m North of its junction with the B581 Coopers Lane and Station Road, Dunton Bassett. A426, Lutterworth Road & Leicester Road From a point 215m South of its junction with Dunton Road, Ashby Magna to a point 173 metres north of its junction with Bill Crane Way, Lutterworth. z- \ft\s ^\^> ,^^, )1 i' THE COMMON SEAL of THE LEICESTERSHIRE ) s ^"^ COUNTY COUNCIL was hereunto affixed ) ^^.s^^' -

Leicestershire Sustainable Community Strategy
LEICESTERSHIRE SUSTAINABLE COMMUNITY STRATEGY FINAL DRAFT MARCH 2008 1 Introduction I am pleased to present our Sustainable Community Strategy to you on behalf of Leicestershire Together, the Local Strategic Partnership for Leicestershire. Leicestershire Together includes all of the organisations and partnerships that deliver public services in Leicestershire, and we seek to improve the quality of life and of public services in the County. This draft Sustainable Community Strategy proposes priorities for improvement in Leicestershire over the next 5 years. These are largely based upon two draft evidence base reports ‘This is Leicestershire’ and ‘Places in Leicestershire’. The structure of the new Sustainable Community Strategy is quite different to that of the previous Community Strategy in that it focuses on what we are going to do rather than how we are going to do it. Our second Local Area Agreement (LAA2) is the key delivery framework for the strategy (the ‘how’ bit) – and more details on the LAA can be found later in this document. The challenge that faces us now is to deliver the ambitions outlined in this Strategy, making a real and measurable difference to the lives of Leicestershire people. David Parsons Chair, Leicestershire Together Contact details: Telephone: 0116 305 6977/8137 E-mail: [email protected] Website: www.leicestershiretogether.org Write to us: Policy Team, Chief Executives Department, Leicestershire County Council, County Hall, Glenfield, Leicestershire LE3 8RA 2 EXECUTIVE SUMMARY Leicestershire Together Leicestershire Together is the Local Strategic Partnership for Leicestershire and includes all of the organisations and partnerships that deliver public services in the County. Our aim is to improve the quality of life for the people of Leicestershire and make Leicestershire the best possible place to live and work for everyone. -

Integrated Recycling and Residual Waste Collection - Daventry District Council, a Beacon Council
SHOWCASING GOOD PRACTICE ENVIRONMENT Integrated Recycling and Residual Waste Collection - Daventry District Council, a Beacon Council Summary Daventry District Council is one of the UK's leading Officers and Elected Members worked closely to recycling authorities. For the past six years the develop a pioneering waste collection service, they had authority has diverted from landfill in excess of 40% of to think outside of the box and learn from their the household waste it has collected, through a mistakes, not being in a position to learn from others' combination of weekly collections of dry recyclables previous experience. and alternate weekly collections of compostable and residual wastes. Latest figures show an overall Daventry District Council has gained unprecedented recycling and composting rate of 45% (2005/06). levels of public participation, service satisfaction levels are high, 85% of users are satisfied with the waste In 1998, Daventry District Council was one of the first service (BVPI 90) and 60% think the council keeps authorities to introduce an integrated recycling and them well informed. Such praise resulted in Daventry waste collection service by virtue of its four-bin system. District Council receiving Beacon Status in 2006 for At the same time it was one of the first authorities in Waste and Recycling. England to successfully introduce an alternate weekly collection of recyclable and residual waste district wide, proving its value as a means of driving public participation in kerbside recycling services. ficiency through ef ovement Impr emce.gov.uk Project background Surveys were taken throughout the trial to ascertain householder perceptions and to obtain feedback on the Daventry District Council has made dramatic changes communication methods used. -

No. 153 December 2016 Web Edition
No. 153 December 2016 Web Edition Airfield Research Group Ltd Registered in England and Wales | Company Registration Number: 08931493 | Registered Charity Number: 1157924 Registered Office: 6 Renhold Road, Wilden, Bedford, MK44 2QA To advance the education of the general public by carrying out research into, and maintaining records of, military and civilian airfields and related infrastructure, both current and historic, anywhere in the world All rights reserved. No part of this publication may be reproduced in any form, by any means, without the prior permission in writing of the author and copyright holder. Any information subsequently used must credit both the author and Airfield Review / ARG Ltd. T HE ARG MA N ag E M EN T TE am Directors Chairman Paul Francis [email protected] 07972 474368 Finance Director Norman Brice [email protected] Director Peter Howarth [email protected] 01234 771452 Director Noel Ryan [email protected] Company Secretary Peter Howarth [email protected] 01234 771452 Officers Membership Secretary & Roadshow Coordinator Jayne Wright [email protected] 0114 283 8049 Archive & Collections Manager Paul Bellamy [email protected] Visits Manager Laurie Kennard [email protected] 07970 160946 Health & Safety Officer Jeff Hawley [email protected] Media and PR Jeff Hawley [email protected] Airfield Review Editor Graham Crisp [email protected] 07970 745571 Roundup & Memorials Coordinator Peter Kirk [email protected] C ON T EN T S I NFO rmati ON A ND RE G UL ar S F E at U R ES Information and Notices .................................................1 AW Hawksley Ltd and the Factory at Brockworth ..... -

Leicestershire
Archaeological Investigations Project 2003 Post-Determination & Non-Planning Related Projects East Midlands LEICESTERSHIRE Blaby 3/25 (E.31.L024) SP 57609800 LE2 9TL GLEN PARVA MOAT, THE FORD, LITTLE GLEN ROAD An Archaeological watching Brief at Glen Parva Moat Hyam, A Leicester : University of Leicester Archaeological Services, 2003, 7pp, refs Work undertaken by: University of Leicester Archaeological Services There was high potential for buried archaeological remains as the site incorporated a moat which is a Scheduled Monument. A shallow pathway 0.15 to 0.2m in depth was excavated in a circular route to the west of the Moat revealing mid grey-brown topsoil on top of grey-brown silty loam subsoil. No archaeological features were observed. Foundations for a site access bridge and gates were also excavated revealing dark brown silty loam above the natural substrate of orange-brown silty clay. No archaeological features or deposits were recorded. [Au(adp)] 3/26 (E.31.L026) SP 50309645 LE9 3JQ POTTERS KILN, STANTON LANE CROFT An Archaeological Watching Brief at Potters Kiln, Stanton Lane, Croft Jarvis, W Leicester : University of Leicester Archaeological Services, 2003, 13pp, figs, tabs Work undertaken by: University of Leicester Archaeological Services An archaeological watching brief was carried out during the groundworks for a new m#nage and associated access road and car park. No archaeological deposits were identified, with artefacts being restricted to occasional unstratified finds of Potter's Marston ware, probably from manuring of the fields. These finds were restricted to the south of the area. [Au(adp)] Archaeological periods represented: PM 3/27 (E.31.Q011) SP 49109470 LE9 4DQ TUDOR COTTAGE, CAREY HILL ROAD, STONEY STANTON An Archaeological Impact Assessment Concerning the Impact of Proposed Works to be Carried Out on the Grade II Listed Building Known as: Tudor Cottage, Carey Hill, Stoney Stanton. -

Harborough District Information Sheet
Harborough District Information Sheet Local Council Information and Support Harborough District Council Address: The Symington Building, Adam & Eve Street, Market Harborough LE16 7AG Phone: 01858 828282 Email: [email protected] Website: https://www.harborough.gov.uk/ (This site provides an A-Z list of all services provided and recent updates). Hours: Monday 8:45am–5pm Tuesday 8:45am–5pm Wednesday 9:30am–5pm Thursday 8:45am–5pm Friday 8:45am–5pm Saturday Closed Sunday Closed Note: Harborough District Council are currently experiencing an issue with the processing of all card payments. This issue will be resolved as soon as possible. COVID-19 Community Support Hub – Open Monday to Friday 9am-5pm. https://www.harborough.gov.uk/hd-community-hub Please note that this service will prioritise those who are most vulnerable and in urgent need of help and support, these include people who are over the age of 70 people with underlying health conditions people who have received an NHS letter stating that they are in a 'shielded' group families who are struggling to cope Complete the online referral form or use the email below and a member of the Community Hub will make contact to see how they can help. Online Form: https://www.harborough.gov.uk/xfp/form/299 Email: [email protected] Social Care Tel: 01858 465331 Website: https://www.leicestershire.gov.uk/adult-social-care-and-health Supermarkets and Food Deliveries Local meal delivery services may be available from some cafés, pubs and restaurants, and some supermarkets can deliver frozen or chilled meals. -

Premises, Sites Etc Within 30 Miles of Harrington Museum Used for Military Purposes in the 20Th Century
Premises, Sites etc within 30 miles of Harrington Museum used for Military Purposes in the 20th Century The following listing attempts to identify those premises and sites that were used for military purposes during the 20th Century. The listing is very much a works in progress document so if you are aware of any other sites or premises within 30 miles of Harrington, Northamptonshire, then we would very much appreciate receiving details of them. Similarly if you spot any errors, or have further information on those premises/sites that are listed then we would be pleased to hear from you. Please use the reporting sheets at the end of this document and send or email to the Carpetbagger Aviation Museum, Sunnyvale Farm, Harrington, Northampton, NN6 9PF, [email protected] We hope that you find this document of interest. Village/ Town Name of Location / Address Distance to Period used Use Premises Museum Abthorpe SP 646 464 34.8 km World War 2 ANTI AIRCRAFT SEARCHLIGHT BATTERY Northamptonshire The site of a World War II searchlight battery. The site is known to have had a generator and Nissen huts. It was probably constructed between 1939 and 1945 but the site had been destroyed by the time of the Defence of Britain survey. Ailsworth Manor House Cambridgeshire World War 2 HOME GUARD STORE A Company of the 2nd (Peterborough) Battalion Northamptonshire Home Guard used two rooms and a cellar for a company store at the Manor House at Ailsworth Alconbury RAF Alconbury TL 211 767 44.3 km 1938 - 1995 AIRFIELD Huntingdonshire It was previously named 'RAF Abbots Ripton' from 1938 to 9 September 1942 while under RAF Bomber Command control. -

Vebraalto.Com
BROOKFIELD COTTAGE 4, CRANOE ROAD, GLOOSTON, LE16 7SR PRICE GUIDE £200,000 A charming two bedroomed 19th Century terraced Road (B6047), turning right at Church Langton, cottage of character offering potential for continuing out of the village, turning right at the next T modernisation and improvement, enjoying views over junction, and after approximately 1 mile, fork left as fields on the edge of the picturesque south east signposted to Glooston. In the centre of the village, turn Leicestershire village of Glooston. right onto Cranoe Road, with the property located on the right hand side with an Andrew Granger & Co for Built predominently of brick and slate construction, this sale board erected to identify the property. pretty cottage has electric night storage heating and wooden framed double glazed windows, and includes a ACCOMMODATION IN DETAIL sitting room with cast iron log burner, inner hall with With the benefit of electric night storage heating and staircase off and cupboard beneath, shower room/wc wooden framed double glazed windows, the interior and fitted dining kitchen with stable type door out. comprises: On the upper floor off a small landing are two bedrooms GROUND FLOOR with pleasant views. SITTING ROOM 14' x 10'10 (4.27m x 3.30m ) Pine panelled entrance door with bullseye pane, electric Outside, there is a paved covered area to the rear with a radiator, pine framed double glazed window to front brick retaining wall and steps up to a tiered garden enjoying a pleasant aspect, attractive fireplace with cast rising to a lawned area backing onto open countryside. -

North Kilworth News, 2019-11
NORTH KILWORTH NEWS November 2019 KEEPING YOU INFORMED Flashes of colour….. It may feel like winter with the (they hope to be back running it next booking and names and numbers are needed longer nights and cooler weather, year). Instead there is a firework and by the middle of December. Details inside. but are there some positives to bonfire display at Lutterworth Golf Club nd November as well? Certainly the on the 2 November if you are looking for Belinda and Sharon beautiful Autumn colour is still all something local to attend. [email protected] around us, you only have to look at the beech trees that are growing This month sees several opportunities for well on the South Kilworth Road, us to sign up to local events that will be and if you get the chance to visit taking place in 2020. The first is the New one of the arboretums you will have Year Quiz on the 11th January in the a stunning display of the most Village Hall. A great opportunity to show vibrant hues nature can throw at us. off your knowledge and enjoy a fun There is the Batsford Arboretum, evening. Then on the 7th of March we Moreton-in-the-Marsh, where this have one of the highlights of the village photo was taken and the National calendar with the Safari Supper. This Arboretum in Staffordshire, both has now been running in the village for within reach for a days outing. many years, but shows no sign of Then, of course, there are the reducing momentum because it is such a fireworks of Bonfire Night to look fantastic evening.