Diffuse Embryoma of the Testis - a Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gonadal (Testicular and Ovarian Tumors)
Gonadal (Testicular and Ovarian Tumors) Gonadal (Testicular and Ovarian Tumors) Authors: Ayda G. Nambayan, DSN, RN, St. Jude Children’s Research Hospital Erin Gafford, Pediatric Oncology Education Student, St. Jude Children’s Research Hospital; Nursing Student, School of Nursing, Union University Content Reviewed by: Guillermo L. Chantada, MD, Hospital JP Garrahan, Buenos Aires, Argentina Cure4Kids Release Date: 1 September 2006 At 4 weeks gestation, germ cells begin to develop in the yolk sac in an undifferentiated state. These primordial germ cells migrate to the gonadal ridge by the 6th week of gestation, and descend into the pelvis or scrotal sac.This migratory route explains the midline location of most extra-gonadal germ cell tumors (intracranial, mediastinal, retroperitoneal or sacrococcygeal). (A -1 ) Germ cell neoplasms arise either from the primordial germ cells (gonadal) or indirectly through embryonic or extra-embryonic differentiation (extra-gonadal). The stromal tumors arise from the primitive sex cords of either the ovary or the testicles, and the rare epithelial tumors arise from the coelomic epithelium that have undergone neoplastic transformations. Though the morphology of each type of germ cell tumor is similar in all locations (whether gonadal or extragonadal), the morphologic type and biological characteristics vary depending on the site of origin and age of the patient. There are three (A – 2) biologically distinct subsets of germ cell tumors: - tumors of the adolescent testis and ovary - extragonadal germ cell tumors of older children - tumors of infants and young children Testicular Germ Cell Tumors: Approximately 7% of all germ cell tumors are testicular and 75% of all (A – 3) testicular tumors have a germ cell origin. -

PROSTATE and TESTIS PATHOLOGY “A Coin Has Two Sides”, the Duality of Male Pathology
7/12/2017 PROSTATE AND TESTIS PATHOLOGY “A Coin Has Two Sides”, The Duality Of Male Pathology • Jaime Furman, M.D. • Pathology Reference Laboratory San Antonio. • Clinical Assistant Professor Departments of Pathology and Urology, UT Health San Antonio. Source: http://themoderngoddess.com/blog/spring‐equinox‐balance‐in‐motion/ I am Colombian and speak English with a Spanish accent! o Shannon Alporta o Lindsey Sinn o Joe Nosito o Megan Bindseil o Kandace Michael o Savannah McDonald Source: http://www.taringa.net/posts/humor/7967911/Sindrome‐de‐la‐ Tiza.html 1 7/12/2017 The Prostate Axial view Base Apex Middle Apex Sagittal view Reference: Vikas Kundra, M.D., Ph.D. , Surena F. Matin, M.D. , Deborah A. Kuban, M.Dhttps://clinicalgate.com/prostate‐cancer‐4/ Ultrasound‐guided biopsy following a specified grid pattern of biopsies remains the standard of care. This approach misses 21% to 28% of prostate cancers. JAMA. 2017;317(24):2532‐2542. http://www.nature.com/nrurol/journal/v10/n12/abs/nrurol.2013.195.html Prostate Pathology Inflammation / granulomas Categories Adenosis, radiation, atrophy seminal vesicle Biopsy Benign TURP HGPIN Unsuspected carcinoma is seen in 12% of Atypical IHC TURP cases. glands Prostatectomy Subtype, Gleason, Malignant fat invasion, vascular invasion Other malignancies: sarcomas, lymphomas Benign Prostate Remember Malignant Glands Lack Basal Glands Cells Basal cells Secretory cells Stroma 2 7/12/2017 Benign Prostatic Lesions Atrophy Corpora amylacea (secretions) Seminal Vesicle Acute inflammation GMS Basal cell hyperplasia Basal cell hyperplasia Granulomas (BPH) (BPH) coccidiomycosis Mimics of Prostate Carcinoma Atrophy. Benign Carcinoma with atrophic features Prostate Carcinoma 1. Prostate cancer is the most common, noncutaneous cancer in men in the United States. -

Cytokeratin 7, Inhibin, and P63 in Testicular Germ Cell Tumor: Superior Markers of Choriocarcinoma Compared to Β-Human Chorionic Gonadotropin☆ Sonya J
Human Pathology (2019) 84,254–261 www.elsevier.com/locate/humpath Original contribution Cytokeratin 7, inhibin, and p63 in testicular germ cell tumor: superior markers of choriocarcinoma compared to β-human chorionic gonadotropin☆ Sonya J. Wegman BS, Anil V. Parwani MD, PhD, MBA, Debra L. Zynger MS, MD⁎ Department of Pathology, The Ohio State University Medical Center, Columbus, OH 43210, USA Received 22 August 2018; revised 2 October 2018; accepted 11 October 2018 Keywords: Summary Choriocarcinoma can be difficult to differentiate from other subtypes of testicular germ cell tumor Testicle; and can occur unexpectedly in a distant, late metastasis. The aim of this investigation was to identify a marker Germ cell tumor; superior to β-human chorionic gonadotropin (β-hCG) for choriocarcinoma. Sixty-two primary and metastatic Choriocarcinoma; testicular germ cell tumors (27 choriocarcinomas, 19 yolk sac tumors, 29 embryonal carcinomas, 28 semino- CK7; mas, 22 teratomas, 3 epithelioid trophoblastic tumors [ETTs]) were analyzed for immunohistochemical expres- Inhibin; sion of cytokeratin 7 (CK7), inhibin, p63, and β-hCG. All choriocarcinomas and ETTs were strongly positive p63; for CK7, whereas seminomas were negative and 52% of embryonal carcinomas had weak reactivity. Eighty- β-hCG four percent of yolk sac tumors and 59% of teratomas were CK7 positive. Eighty-nine percent of choriocarci- nomas and 100% of ETTs were positive for inhibin, with reactivity highlighting syncytiotrophoblasts, whereas seminomas, embryonal carcinomas, yolk sac tumors, and teratomas were negative. Eighty-five percent of cho- riocarcinomas expressed p63, with staining mostly in mononucleated trophoblasts, whereas seminomas, em- bryonal carcinomas, and yolk sac tumors were negative. -

Frequency of Malignant Ovarian Germ Cell Tumor and Distribution of Demographic Features in a Main Tertiary Hospital in Iran
©2018 ASP Ins., Afarand Scholarly Publishing Institute, Iran ISSN: 2476-5848; Journal of Obstetrics, Gynecology and Cancer Research. 2018;3(2):59-63. Frequency of Malignant Ovarian Germ Cell Tumor and Distribution of Demographic Features in a Main Tertiary Hospital in Iran A R T I C L E I N F O A B S T R A C T Aims Ovarian cancer is the 4th cause of women’s mortality occurring due to cancer. Malignant Article Type germ cell tumors (GCTs) account for 5% of malignant ovarian tumors and 70% of ovarian Original Research tumors in women between the ages of 10-30 years old. The aim of the present study was to detect the frequency of malignant ovarian germ cell tumor and distribution of demographic Authors features in the most crowded gynecology oncology clinic. 1 Setareh Akhavan MD, Materials and Methods This cohort descriptive-analytical study was conducted on cases 2 Jila Agah* MD, with malignant ovarian tumor managed in Vali-Asr hospital, Tehran, Iran, from 2001 to 2018 Abbas Alipour3 PhD (n=1540). The malignant germ cell tumors cases were extracted (n=128) and evaluated in point of epidemiologic and demographic data via the software SPSS 24. Findings 128 patients (8.3%) had GCTs. The average age was 23.88±7.85 years. 79.7% lived in the city, 76.6% had medium economic status and 53.6% had normal body mass index. Premature puberty was revealed in one person. Karyotype XY was detected in 5 persons. How to cite this article About 70.3% of the patients had no parity. -

Testicular Mixed Germ Cell Tumors
Modern Pathology (2009) 22, 1066–1074 & 2009 USCAP, Inc All rights reserved 0893-3952/09 $32.00 www.modernpathology.org Testicular mixed germ cell tumors: a morphological and immunohistochemical study using stem cell markers, OCT3/4, SOX2 and GDF3, with emphasis on morphologically difficult-to-classify areas Anuradha Gopalan1, Deepti Dhall1, Semra Olgac1, Samson W Fine1, James E Korkola2, Jane Houldsworth2, Raju S Chaganti2, George J Bosl3, Victor E Reuter1 and Satish K Tickoo1 1Department of Pathology, Memorial Sloan Kettering Cancer Center, New York, NY, USA; 2Cell Biology Program, Memorial Sloan Kettering Cancer Center, New York, NY, USA and 3Department of Internal Medicine, Memorial Sloan Kettering Cancer Center, New York, NY, USA Stem cell markers, OCT3/4, and more recently SOX2 and growth differentiation factor 3 (GDF3), have been reported to be expressed variably in germ cell tumors. We investigated the immunohistochemical expression of these markers in different testicular germ cell tumors, and their utility in the differential diagnosis of morphologically difficult-to-classify components of these tumors. A total of 50 mixed testicular germ cell tumors, 43 also containing difficult-to-classify areas, were studied. In these areas, multiple morphological parameters were noted, and high-grade nuclear details similar to typical embryonal carcinoma were considered ‘embryonal carcinoma-like high-grade’. Immunohistochemical staining for OCT3/4, c-kit, CD30, SOX2, and GDF3 was performed and graded in each component as 0, negative; 1 þ , 1–25%; 2 þ , 26–50%; and 3 þ , 450% positive staining cells. The different components identified in these tumors were seminoma (8), embryonal carcinoma (50), yolk sac tumor (40), teratoma (40), choriocarcinoma (3) and intra-tubular germ cell neoplasia, unclassified (35). -

Dysgerminoma: Diagnostic Impasse
International Surgery Journal Anandakannan I et al. Int Surg J. 2020 Nov;7(11):3811-3814 http://www.ijsurgery.com pISSN 2349-3305 | eISSN 2349-2902 DOI: http://dx.doi.org/10.18203/2349-2902.isj20204700 Case Report Dysgerminoma: diagnostic impasse Indrajit Anandakannan*, Shanthi Ponnandai Swaminathan, Vikas Kawarat, Rajeshwari Mani, Kannan R. Institute of General Surgery, Madras Medical College and Rajiv Gandhi Government General Hospital, Chennai, Tamil Nadu, India Received: 13 August 2020 Revised: 07 October 2020 Accepted: 12 October 2020 *Correspondence: Dr. Indrajit Anandakannan, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Dysgerminoma is a rare malignant ovarian tumour in women of reproductive age group, featuring lower abdominal pain and abdominal mass with elevated tumour markers. The tumour grows rapidly and diagnosed at an earlier stage. We present a short-statured 20 years girl with intermittent abdominal pain and distention for 4 months, on examination huge abdominal mass of size 20x15 cm, firm in consistency was palpable, lower limit not ascertained. Routine blood investigations normal, thyroid function test showed hypothyroidism. A plain abdominal radiograph shows a large homogenous mass fitting mid part of abdomen with displaced bowel loop. Contrast-enhanced computed tomography abdomen and pelvis show up 20x18.5x9.5 cm well defined heterogeneous mass, with areas of necrosis suggesting mesenchymal tumour or germ cell tumour. -

About Testicular Cancer Overview and Types
cancer.org | 1.800.227.2345 About Testicular Cancer Overview and Types If you have been diagnosed with testicular cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to start. ● What Is Testicular Cancer? Research and Statistics See the latest estimates for new cases of testicular cancer and deaths in the US and what research is currently being done. ● Key Statistics for Testicular Cancer ● What’s New in Testicular Cancer Research? What Is Testicular Cancer? Cancer starts when cells begin to grow out of control. Cells in nearly any part of the body can become cancer and spread to other parts of the body. To learn more about how cancers start and spread, see What Is Cancer?1 Cancer that starts in the testicles is called testicular cancer. To understand this cancer, it helps to know about the normal structure and function of the testicles. 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 What are testicles? Testicles (also called testes; a single testicle is called a testis) are part of the male reproductive system. The 2 organs are each normally a little smaller than a golf ball in adult males. They're held within a sac of skin called the scrotum. The scrotum hangs under the base of the penis. Testicles have 2 main functions: ● They make male hormones (androgens) such as testosterone. ● They make sperm, the male cells needed to fertilize a female egg cell to start a pregnancy. Sperm cells are made in long, thread-like tubes inside the testicles called seminiferous tubules. -

Handbook for Children with Germ Cell Tumors
Handbook for Children with TM Germ Cell Tumors Winter 2018 from the Cancer Committee of the American Pediatric Surgical Association ©2018, American Pediatric Surgical Association I CONTRIBUTORS Brent R. Weil, MD Boston Children’s Hospital Boston, MA Rebecca A. Stark, MD UC Davis Children’s Hospital Sacramento, CA Deborah F. Billmire, MD Riley Children’s Hospital Indianapolis, IN Frederick J. Rescorla, MD Riley Children’s Hospital Indianapolis, IN John Doski MD San Antonio, TX NOTICE The authors, editors, and APSA disclaim any liability, loss, injury or damage incurred as a consequence, directly or indirectly, of the use or application of any of the contents of this volume. While authors and editors have made every effort to create guidelines that should be helpful, it is impossible to create a text that covers every clinical situation that may arise in regards to either diagnosis and/or treatment. Authors and editors cannot be held responsible for any typographic or other errors in the printing of this text. Any dosages or instructions in this text that are questioned should be cross referenced with other sources. Attending physicians, residents, fellows, students and providers using this handbook in the treatment of pediatric patients should recognize that this text is not meant to be a replacement for discourse or consultations with the attending and consulting staff. Management strategies and styles discussed within this text are neither binding nor definitive and should not be treated as a collection of protocols. TABLE OF CONTENTS 1. Introduction 2. One-Minute Reviews 3. Classification and Differential Diagnosis 4. Staging 5. Risk Groups 6. -

Leydig Cell Tumour
Non-germ cell tumours of the testis Testis: non-germ cell tumours . Sex cord-stromal tumours Dr Jonathan H Shanks . Haemolymphoid neoplasms . Other neoplasms The Christie NHS . Tumour-like conditions Foundation Trust, Manchester, UK . Metastases The Christie NHS Foundation Trust The Christie NHS Foundation Trust Testis: sex cord-stromal tumours . Leydig cell tumour . Sertoli cell tumour, NOS . Sclerosing Sertoli cell tumour . Large cell calcifying Sertoli cell tumour . Granulosa cell tumour, adult-type . Juvenile granulosa cell tumour . Fibroma . Brenner tumour . Sertoli-Leydig cell tumours (exceptionally rare in testis) Leydig cell tumour . Sex cord-stromal tumour, unclassified . Mixed germ cell-sex cord stromal tumour - gonadoblastoma - unclassified (some may be sex cord stromal tumours with entrapped germ cells – see Ulbright et al., 2000) - collision tumour The Christie NHS Foundation Trust The Christie NHS Foundation Trust Differential diagnosis of Leydig cell TTAGS tumour . Testicular tumour of adrenogenital syndrome (TTAGS) . Multifocal/bilateral lesions (especially in a child/young adult) . Seen in patients with congenital adrenal hyperplasia . Leydig cell hyperplasia (<5mm) . 21 hydroxylase deficience most common . Large cell calcifying Sertoli cell tumour . Elevated serum ACTH . Sertoli cell tumour . Seminoma (rare cases with cytoplasmic clearing) . Benign lesion treated with steroids; partial orchidectomy reserved for steroid unresponsive cases . Mixed sex cord stromal tumours . Sex cord stromal tumour unclassified . Fibrous bands; lipofuscin pigment ++; nuclear pleomorphism but no mitosis . Metastasis e.g. melanoma The Christie NHS Foundation Trust The Christie NHS Foundation Trust Immunohistochemistry of testicular Histopathological and immunophenotypic features of testicular tumour of adrenogenital Leydig cell tumour syndrome Wang Z et al. Histopathology 2011;58:1013-18 McCluggage et al Amin, Young, Scully . -
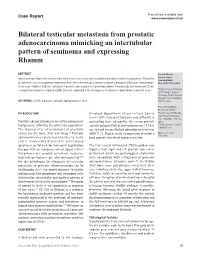
Bilateral Testicular Metastasis from Prostatic Adenocarcinoma Mimicking an Intertubular Pattern of Seminoma and Expressing Rhamm
Free full text available from Case Report www.cancerjournal.net Bilateral testicular metastasis from prostatic adenocarcinoma mimicking an intertubular pattern of seminoma and expressing Rhamm ABSTRACT Santosh Menon, Adenocarcinoma of prostate metastasizing to testis is a rare occurrence and is incidentally detected in orchiectomy specimens. The pattern Sumeet Gujral, Ganesh Bakshi1, of metastasis may mimic a primary neoplasm of testis like a seminoma or lymphoma and pose a diagnostic difficulty for the pathologist. Hemant B. Tongaonkar1 A rare case of bilateral testicular metastasis of prostatic adenocarcinoma is presented wherein the metastatic cells expressed CD168, a receptor for hyaluronan mediated motility (Rhamm), implicated in the development of androgen independence in prostate cancer. Departments of Pathology, and 1Urologic Surgical Oncology, Tata Memorial Hospital, Parel, Mumbai- KEY WORDS: CD168, metastasis, prostatic adenocarcinoma, testis 400 012, India For correspondence: Dr. Santosh Menon, INTRODUCTION Oncology department of our tertiary Cancer Department of Pathology, Tata Memorial Hospital, Center with history of backache and difficulty in Parel, Mumbai - 400 012, Prostatic adenocarcinoma is one of the commonest micturition since six months. The serum prostate India. malignancies afflicting the adult male population. specific antigen (PSA) at presentation was 173.433 E-mail: santosh.menon@ rediffmail.com The favored sites of metastasis of prostatic ng / ml and serum alkaline phosphatase level was cancer are the bone, -

Treating Testicular Cancer If You’Ve Been Diagnosed with Testicular Cancer, Your Treatment Team Will Discuss Your Options with You
cancer.org | 1.800.227.2345 Treating Testicular Cancer If you’ve been diagnosed with testicular cancer, your treatment team will discuss your options with you. It’s important to weigh the benefits of each treatment option against the possible risks and side effects. How is testicular cancer treated? Depending on the type and stage of the cancer, as well as other factors, treatment options for testicular cancer can include: ● Surgery for Testicular Cancer ● Radiation Therapy for Testicular Cancer ● Chemotherapy for Testicular Cancer ● High-Dose Chemotherapy and Stem Cell Transplant for Testicular Cancer Common treatment approaches In recent years, a lot of progress has been made in treating testicular cancer. Surgical methods have been refined, and doctors know more about the best ways to use chemotherapy and radiation to treat different types of testicular cancer. In some cases, more than one of type of treatment might be used. ● Treatment Options for Testicular Cancer, by Type and Stage Who treats testicular cancer? You may have different types of doctors on your treatment team, depending on the stage of your cancer and your treatment options. These doctors may include: 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 ● A urologist: a surgeon who specializes in treating diseases of the urinary system and male reproductive system ● A radiation oncologist: a doctor who treats cancer with radiation therapy ● A medical oncologist: a doctor who treats cancer with medicines like chemotherapy You might have many other specialists on your treatment team as well, including physician assistants, nurse practitioners, nurses, nutrition specialists, social workers, and other health professionals. -

Ovary (Germ Cell Tumour) Fact Sheet
Cancer Association of South Africa (CANSA) Fact Sheet on Germ Cell Tumour of the Ovary Introduction Germ cell tumours begin in the reproductive cells (egg or sperm) of the body. Ovarian germ cell tumours usually occur in teenage girls or young women and most often affect just one ovary. [Picture Credit: Germ Cell Ovarian Tumours] The ovaries are a pair of organs in the female reproductive system. They are situated in the pelvis, one on each side of the uterus. Each ovary is about the size and shape of an almond. The ovaries make ova (eggs) and female hormones. Ovarian germ cell tumour is a general name that is used to describe several different types of cancer. The most common ovarian germ cell tumour is called dysgerminoma. Acosta, A.M., Sholl, L.M., Cin, P.D., Howitt, B.E., Otis, C.N. & Nucci, M.R. 2020. Aims: Tumours of the female genital tract with a combination of malignant Mullerian and germ cell or trophoblastic tumour (MMGC/T) components are usually diagnosed in postmenopausal women, and pursue an aggressive clinical course characterised by poor response to therapy and early relapses. These clinical features suggest that MMGC/T are somatic in origin, but objective molecular data to support this interpretation are lacking. This study evaluates the molecular features of nine MMGC/T, including seven tumours containing yolk sac tumour (YST), one tumour containing choriocarcinoma and one tumour containing epithelioid trophoblastic tumour. The objectives were to: (i) investigate whether MMGC/T show a distinct genetic profile and (ii) explore the relationship between the different histological components.